 Time to Open8-16 weeksLaunch runway
Time to Open8-16 weeksLaunch runwayHow To Open A Hospital Cleaning Service In 8 To 16 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open8-16 weeksLaunch runway  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckApproval gateApproval path
Key BottleneckApproval gateApproval path First Revenue StepFirst contractPilot starts
First Revenue StepFirst contractPilot starts


Key Takeaways
- Written SOPs are the launch credibility base.
- Trained staff prevent unsafe work and complaints.
- Insurance and vendor approval can delay first revenue.
- Scheduling and quality control protect renewals after go-live.
Time to Open8-16 weeksLaunch runwayLaunch Sequence6 stagesCompliance firstKey BottleneckApproval gateApproval pathFirst Revenue StepFirst contractPilot startsLaunch timeline
This short web timeline summarizes the launch plan, and the XLSX export contains the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12Week 13Week 14Week 15Week 16
Legal / compliance
- File entity
- Bind insurance
- Bloodborne training
- SOP manual
- Approval packet
Vendors / equipment
- Source disinfectants
- Order cart kits
- Set floor kit
- Open vendor accounts
Staffing / training
- Post roles
- Screen hires
- Train techs
- Set coverage roster
Sales / outreach
- Build target list
- Schedule walkthroughs
- Set vendor portals
- Send proposals
- Close first account
Operations / readiness
- Map routes
- Review approval gate
- Start pilot service
- Confirm coverage
Finance / admin
- Build cash plan
- Set CAC model
- Set pay billing
- Track KPIs
Why test launch plans before hiring?
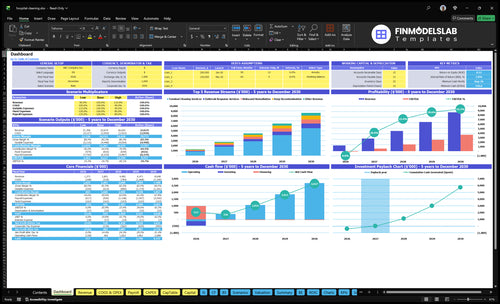
Hospital Cleaning Service uses the Hospital Cleaning Service Financial Model Template to test revenue, costs, cash, and break-even. Open it.
Launch model highlights
- Month 1-60 assumptions
- $120,000 Year 1 marketing
- $2,400 CAC
- 32 billable hours
- Four technicians planned
- 36% variable costs
- Service pricing range
- Break-even path visible
What hospital cleaning business mistakes should you avoid?
If you sell the Hospital Cleaning Service before your SOPs, training, insurance, disinfectant records, and documentation are ready, you’re setting up avoidable risk. Here’s the quick math: with 4 sanitation technicians, 32 billable hours per active customer each month, and 36% variable costs before fixed overhead and wages, sloppy scheduling or one missed shift can hit margin fast.
Launch risks
- Weak infection-control procedures
- Untrained cleaners on day one
- Wrong or undocumented disinfectants
- Underinsured operations and claims risk
Fix first
- Tighten SOPs before selling
- Assign supervisors for inspections
- Run mock audits and incident reports
- Build backup staffing and diversify leads
How long does it take to start a hospital cleaning service?
A Hospital Cleaning Service can be operationally ready in about 8 to 16 weeks, but contract-ready hospital revenue usually takes longer because vendor portals, RFPs, insurance review, background checks, infection-control approval, and walkthroughs add steps. A clinic or urgent care account can move faster than a full hospital contract, so separate launch-ready from contract-ready. Plan for Month 1 setup, $13,600 in monthly fixed overhead before wages, and a $120,000 Year 1 marketing budget; if onboarding slips, cash runway and technician scheduling need a second look.
Launch timing
- 8 to 16 weeks for readiness
- Legal setup starts the clock
- Training and supplies run in parallel
- Hospital contracts take longer
Cash planning
- $13,600 monthly fixed overhead
- $120,000 Year 1 marketing budget
- Month 1 setup needs cash
- Delay means runway recheck
How do you get hospital cleaning contracts?
To win hospital cleaning contracts, start with smaller healthcare sites and turn that work into proof before you pitch hospital departments or vendor portals; the fastest path is recurring cleaning or a controlled pilot, not a full-campus promise. If you need the setup and cost logic, see How Much Does It Cost To Open And Launch Your Hospital Cleaning Service Business? and use the same process for outpatient clinics, urgent care centers, dental offices, surgery centers, medical office buildings, property managers, and procurement teams. With a $120,000 Year 1 marketing budget and $2,400 CAC (customer acquisition cost), that implies about 50 customers, but healthcare references still matter a lot.
Start small first
- Target outpatient clinics first
- Use urgent care pilot jobs
- Serve dental offices and surgery centers
- Build references before larger bids
Lead with proof
- Share infection-control SOPs
- Include OSHA training records
- Attach EPA-registered disinfectant lists
- Offer insurance and checklists
Verify go or no-go readiness before opening
Launch readiness checklist
Use this go-live approval checklist before opening the Hospital Cleaning Service.
Compliance
- Business registration filedCritical
You need a legal entity before contracts, billing, and hiring start.
- Service scope approvedCritical
The scope must match terminal cleaning, outbreak response, and documentation work.
- Insurance boundCritical
Coverage should be active before staff enter any healthcare site.
- Bloodborne training loggedHigh
Training cuts exposure risk and supports site access approvals.
Protocols
- Written SOPs approvedCritical
Clear steps keep crews consistent when they clean, document, and report.
- High-touch steps signed offHigh
These steps protect patients and reduce missed surfaces during routine work.
- Terminal cleaning testedCritical
Terminal cleaning is a core service, so the process must work before launch.
- Incident reporting flow readyHigh
Fast reporting helps fix exposure, spill, or damage issues before they spread.
Tools
- EPA disinfectant list approvedCritical
Only approved disinfectants should go on site, so the team avoids bad product use.
- PPE inventory countedCritical
PPE must cover the first jobs without forcing unsafe reuse or delays.
- Vendor accounts openedHigh
Active supplier accounts keep disinfectants, PPE, and parts available on time.
- Equipment leases activeHigh
The fleet and cleaning gear must be live before first site work starts.
Staffing
- Four technicians hiredCritical
Year 1 assumes 4 technicians, so launch labor must be in place on day one.
- Shift coverage roster builtCritical
Hospitals need reliable coverage, plus backup for absences and rush jobs.
- Background checks clearedCritical
Cleared staff are often required before they can enter healthcare facilities.
- Certification records completeHigh
Records prove workers can handle infection control and site-specific tasks.
Sales
- Facility walkthrough list readyHigh
A clean walkthrough list speeds pricing, scoping, and first-customer approval.
- First-contract target setHigh
The first revenue path should be clear before launch spend ramps up.
- Pricing and proposal approvedCritical
Pricing must support margin and match the services in the signed scope.
- Booking workflow testedHigh
A working booking path keeps the first contract from stalling after approval.
Cash
- CAC model under $2,400High
Year 1 CAC is $2,400, so early lead costs need to stay near that level.
- 32-hour capacity confirmedHigh
Year 1 assumes 32 billable hours per active customer, so staffing must support it.
- 64% contribution confirmedCritical
The model needs 64% contribution before fixed labor and overhead.
- Cash runway covers launchCritical
Runway must cover the $437k minimum cash point before breakeven in month 8.
- Go-live signoff completedCritical
Final signoff should confirm safe work, clean reporting, and a real sales path.
Want to see the six launch drivers that matter?
1Compliance & Infection Control
8-16 wksWritten SOPs and infection-control review are the launch gate for hospital approval.
2Trained Cleaning Staff
4 techsFour technicians trained on PPE and room checks cut rework and complaints.
3Equipment & Disinfectants
36% loadStocked disinfectants, PPE, and equipment keep the first contract from stalling.
4Insurance & Risk Controls
$2.8K/moInsurance certificates and incident rules drive vendor approval and procurement trust.
5Contract Approval
$120K / $2.4K CACOutreach and vendor portals turn readiness into pilots, but not a signed hospital contract.
6Scheduling & QA
32 hrs/customerShift plans and QA checks keep 32 billable hours per customer on track.
Compliance And Infection-Control Systems
Compliance and Infection-Control Readiness
Compliance is the license to be trusted in healthcare cleaning. If launch starts without a written SOP pack for high-touch surfaces, restrooms, waiting rooms, approved patient areas, terminal cleaning, PPE use, disinfectant contact times, documentation, and escalation, client review slows fast. One failed infection-control review can block onboarding, delay first revenue, and force rework before the crew can enter a facility.
The pack also needs OSHA bloodborne pathogen training, EPA-registered disinfectant selection, facility-specific protocols, and inspection logs. Those inputs tie to insurance and staff training, so weak paperwork can stall vendor approval even when labor is ready. If approval slips, first invoices slip too, so cash stays tied up longer. The result is simple: weaker proposals, more questions from facilities, and a later start date.
Build the review packet first
Start with a control set the facility can review in minutes: SOP index, training records, insurance certificate, disinfectant list, and inspection-log template. That is the readiness signal. It shows the work is documented, repeatable, and safe, so sales meetings turn into approvals instead of long back-and-forth.
Then test the process before opening. Run a mock walkthrough, assign who signs off on protocols, and confirm who escalates exceptions after a job. If the client wants changes, update the pack before day one so the crew is not improvising in front of a healthcare team.
- Verify insurance and staff training first
- Match SOPs to each facility
- Log contact times and exceptions
- Get client approval before first shift
1
Trained Cleaning Staff
Trained Cleaning Staff
Training is what decides if a healthcare cleaning team can work safely on day one. The readiness signal is simple: every assigned cleaner can follow PPE rules, bloodborne pathogen training, room-by-room SOPs, high-touch checklists, and documentation steps without improvising.
Here’s the quick math: 4 sanitation technicians at $48,000 each means $192,000 per year in salary, or about $16,000 per month before payroll taxes and benefits. If training slips, the launch bottleneck is not labor supply; it’s unsafe or inconsistent service on patient-area and terminal cleans, which can slow first contracts and hurt retention.
Train Before You Promise Patient-Area Work
Start with the basics: onboarding, any required background checks, shadow shifts, supervisor review, and backup coverage. Do not schedule patient-area or terminal cleaning until each cleaner has repeated the same SOPs enough times to do them the same way every time.
Keep the launch tight by linking training to the real work order flow. Verify written SOPs, disinfectants, equipment, and shift schedules before the first job. A clean launch here means fewer complaints, fewer re-dos, and better account retention in the first months.
- Test PPE use before field work.
- Review each room-by-room SOP.
- Require documented checklist completion.
- Hold a backup cleaner for coverage.
2
Healthcare-Grade Equipment And Disinfectants
Stocked Supply System
For a hospital cleaning service, the launch does not really start until the supply room is ready. A stocked, documented system for EPA-registered disinfectants, PPE, carts, microfiber tools, floor-care equipment, labels, and waste boundaries is what lets crews work safely on day one and support infection-control claims without improvising.
Here’s the quick math: Year 1 assumes 12% of revenue for cleaning supplies and disinfectants, 35% for equipment maintenance, and 4% for PPE. If any of those inputs are missing, the first contract can stall, work slows, and inspection risk goes up fast. One empty shelf can delay an entire site start.
Build Reorder Rules First
Before opening, lock supplier setup, usage tracking, SDS access, storage rules, and backup vendors. That means every cleaner knows where products live, how they are logged, and when to reorder. It also means the team can show proof of control during client review or a site audit.
Use a simple launch check: no single-source item, all disinfectants documented, and replacement stock on hand for the first contract. If deliveries slip or a product is out of stock, day-one service can still continue without breaking workflow or forcing a delay.
- Confirm EPA-registered disinfectant inventory.
- Store PPE and chemicals separately.
- Keep SDS sheets easy to reach.
- Assign backup vendors before launch.
- Track use to trigger reorder points.
3
Insurance And Risk Controls
Insurance And Vendor Readiness
For a hospital cleaning service, insurance is often the gatekeeper before the first job starts. Healthcare facilities want current certificates, contract-ready coverage, and clear incident rules before they approve a vendor. The model assumes $2,800 per month in premiums, so this is a real launch cost, not just paperwork.
Here’s the quick risk: missing certificates or weak incident procedures can stall vendor approval, which delays opening and first revenue. You also need workers’ compensation where required, bonding if requested, and a review of vehicle and equipment risk. That same documentation discipline helps build procurement trust from day one.
Lock Coverage Before Outreach
Start with a contract-risk review by a qualified professional, then align coverage to client requirements before you send proposals. The readiness stack should include general liability, workers’ compensation where required, and any bonding the facility asks for. If the client’s vendor packet is missing one item, approval can stall.
- Collect certificates before walkthroughs.
- Write incident steps in plain English.
- Assign one owner for renewals.
- Keep safety rules with staff training.
- Store proof for every client file.
What this setup hides is timing. Insurance, staffing, and training all have to move together, because a facility will not treat you as day-one ready if the team cannot show safety rules and clean documentation on the spot.
4
Contract Acquisition And Vendor Approval
Contract Approval Pipeline
For a hospital cleaning launch, contract acquisition is the gate to day-one revenue. A facility can want the service and still block work until vendor approval is done. So the launch needs a complete packet: outreach list, proof-of-capability packet, proposal template, insurance certificates, SOP summary, training records, references when available, and vendor portal tracking.
Here’s the quick math: with a $120,000 marketing budget and $2,400 CAC (customer acquisition cost), the plan funds about 50 contract wins if the model holds. The real risk is long hospital approval cycles, so early pilots with clinics, urgent care centers, surgery centers, dental offices, and medical property managers help bring in revenue before one large bid closes.
Build The Approval Packet First
Before outreach starts, verify compliance, staff coverage, and walkthrough readiness. Those three inputs decide whether procurement will review you now or send you back for missing proof. One missing document can stall first revenue.
- Keep one master packet version.
- Track every portal submission.
- Attach current insurance proof.
- Include SOP and training records.
- Log follow-up dates by facility.
Use the same packet for every channel, then adjust only scope and pricing. That keeps proposals fast, lowers back-and-forth, and helps land pilot work while larger hospital approvals are still moving.
5
Scheduling, Supervision, And Quality Assurance
Scheduling and Quality Control
Scheduling and quality control keep the first contract from slipping on day one. With the Year 1 model at 32 billable hours per active customer per month and 4 sanitation technicians, every job needs a named shift, a backup, and a check process before start date.
The real risk is missed coverage or undocumented work. Since quality assurance specialist and compliance officer roles start in Month 13, early supervision has to sit with operations leadership, or service failures can show up before the first renewal cycle.
Build the shift control before opening
Set the launch plan around shift plan, supervisor assignment, backup roster, inspection checklist, issue-escalation path, and client reporting cadence. Tie each account to access rules, SOPs, and the equipment needed for that site so the team can work without improvising.
Before opening, verify who covers nights, call-outs, and client sign-off. Use one clean rule: if a task is not assigned, checked, and reported, it is not ready. That protects first-revenue work, limits rework, and keeps leadership in control until Month 13 roles come online.
- Assign every site to one supervisor.
- Keep one backup per shift.
- Track every inspection the same day.
- Escalate access issues immediately.
- Send client reports on a fixed cadence.
6
Related Products
- Hospital Cleaning Service Porter's Five Forces Analysis
- Hospital Cleaning Service BCG Matrix
- Hospital Cleaning Service Business Model Canvas
- 7 Critical KPIs to Track for Hospital Cleaning Service Growth
- Hospital Cleaning Service Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Hospital Cleaning Service Profitability
- How Much Does It Cost To Run A Hospital Cleaning Service Monthly?
- Hospital Cleaning Service Startup Costs: $328k CAPEX and $437k Cash
- Hospital Cleaning Service Financial Model Template in Excel
- How Much Hospital Cleaning Service Owners Make With $254M Year 1 Revenue
- How to Write a Hospital Cleaning Service Business Plan in 7 Steps
- Hospital Cleaning Service Marketing Mix
- Hospital Cleaning Service Marketing Plan
- Hospital Cleaning Service Business Proposal
- Hospital Cleaning Service PESTEL Analysis
- Hospital Cleaning Service Pitch Deck Example Editable PPTX
- Hospital Cleaning Service Business SWOT Analysis
- Hospital Cleaning Service Value Proposition Canvas
Frequently Asked Questions
You need documented training more than a single universal certificate OSHA bloodborne pathogen training, PPE procedures, infection-control SOPs, EPA-registered disinfectants, and facility-specific onboarding matter most The 8 to 16 week launch window assumes those items move in parallel with insurance and staffing