 Owner income$35.5k
Owner income$35.5kHow Much Can An In-Home IV Therapy Owner Make? $120K Plus Profit

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$35.5k  Net margin31.6%
Net margin31.6% Revenue for target pay$112k
Revenue for target pay$112k Business difficultyHard
Business difficultyHard
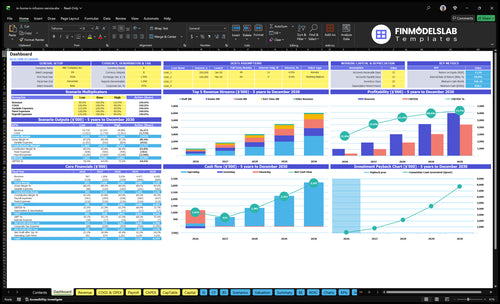


You’re estimating owner pay from a mobile infusion service, not a nurse wage This first-year model shows $120,000 owner salary, about $966,960 revenue, and about $354,338 EBITDA before taxes, debt, capex, and reserves
Owner income$35.5kNet margin31.6%Revenue for target pay$112kBusiness difficultyHardWant to test your own owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want the full forecast view for In-Home IV Therapy?
This In-Home IV Therapy Financial Model Template shows revenue, margin, costs, reserves, and owner take-home assumptions—open the model.
Owner-income model highlights
- Owner pay stays separate
- Revenue and margin tracked
- Scenarios compare ramp speed
Can a non-nurse own an IV therapy business?
Yes—a non-nurse can often own In-Home IV Therapy, but the state’s medical, nursing, pharmacy, and corporate practice rules decide how the model can be set up. Here’s the quick math: medical oversight can add a $3,000 monthly fee plus a 0.5 FTE Medical Director at about $30,000 per year, and hiring clinicians can grow visits but usually cuts per-visit margin. If licensing allows, an owner-operator may keep more early gross profit, but you should verify the structure with qualified healthcare counsel before launch.
Owner setup
- Non-clinical ownership can still earn profit.
- State rules control the legal structure.
- Owner-operator models may keep more early gross profit.
- Verify licensing before you launch.
Cost and margin
- $3,000 monthly oversight fee.
- $30,000 yearly for a 0.5 FTE Medical Director.
- Hired clinicians can scale visits.
- More visits can mean lower per-visit margin.
What expenses reduce in-home IV therapy business profit?
In-Home IV Therapy profit gets squeezed first by service costs: 8% IV fluids and formulations, 4% medical supplies, 5% practitioner per-visit pay, and 2% vehicle and travel. Fixed overhead adds another $9,700/month in year one, and payroll is $312,500 in year one; for launch cost context, see How Much Does It Cost To Launch The In-Home IV Therapy Business?. The other profit drains are waste, payment fees, customer acquisition, taxes, reserves, and owner distributions.
Variable cost hits
- 8% IV fluids and formulations
- 4% medical supplies
- 5% practitioner per-visit pay
- 2% vehicle and travel
Fixed cost pressure
- $3,000 medical director oversight
- $1,500 technology
- $1,000 professional liability insurance
- $2,500 office rent
How many IV therapy appointments are needed to make owner income?
In-Home IV Therapy needs about 199 completed appointments per month to cover the modeled $10,000 owner salary, payroll, fixed overhead, and variable costs; see What Is The Current Customer Satisfaction Level For In-Home IV Therapy? when checking demand quality. Here’s the quick math: $35,742 monthly overhead and payroll ÷ $180 contribution per visit = 199 visits.
Owner income math
- Target 199 completed visits monthly
- Contribution per visit: $180
- Monthly overhead and payroll: $35,742
- Base volume: 362 visits monthly
Watch the risks
- 163 visits sit above break-even
- Average ticket below $223 raises volume
- Variable costs above 19% raise volume
- Payer mix and staffing change cash
What drives owner income the most?
1
199/moAppointment Volume
You clear first-year break-even at about 199 visits a month, and the model shows 362, so filling the calendar is the main profit swing.
2
$223Average Ticket
The modeled average visit price is about $223, so even small price changes move monthly revenue fast.
3
$312.5KClinician Labor
Year 1 payroll totals $312,500, so the FTE mix and utilization rate drive take-home more than small cost tweaks.
4
81%Supply Margin
At 81% first-year contribution margin, direct cost slippage shows up fast in owner pay.
5
19%Route Density
Tighter routing helps hold variable cost load near 19% and protects margin when visits are spread out.
6
10 moRepeat Customers
More repeat visits lower selling cost per booking and help the model reach the 10-month payback sooner.
In-Home IV Therapy Core Six Income Drivers
Appointment Volume
Appointment Volume
Appointment volume means completed, paid visits, not inquiries or followers. In year one, the model books 362 visits per month and about $80,580 in monthly revenue. The break-even point is about 199 visits per month at $180 contribution per visit, so every filled slot moves owner pay faster.
Utilization runs from 50% to 70% in year one by registered nurse type, so travel gaps, cancellations, and idle staff can cut cash flow fast. One empty route can erase the gain from several booked visits. If staffing and scheduling hold, more completed appointments flow straight into profit.
Track completed visits, not interest
Measure booked visits, completed visits, no-shows, and nurse utilization by role every week. Keep the key inputs tight: visit count, price, contribution per visit, travel time, and staff hours. If completion drops below 199 visits per month, owner income starts to tighten fast.
Use the schedule to protect volume: cluster visits by area, confirm appointments early, and watch cancellation patterns by time of day. Push for more filled appointment blocks before adding staff. Higher volume only helps if the clinic can deliver it without extra idle time.
1
Average Ticket And Service Mix
Average Ticket and Service Mix
If your average ticket stays near $223, the mix of drips, add-ons, group visits, packages, and memberships matters as much as visit count. The modeled price range is $200 to $280, based on RN category and event work. At 362 monthly visits, every $10 lift adds about $3,620 in monthly revenue before added costs.
The upside is simple: higher-value services can lift take-home income if customers accept the price and the visit still covers labor, travel, and supplies. The hidden risk is selling more revenue without more profit. Watch contribution per visit, not just headline price, and avoid medical-benefit claims when you test a higher rate.
Test Price Before You Raise It
Track booked revenue per completed visit by service type, RN category, and event work. That shows which offers actually pay. Test one $10 price step at a time, then compare conversion, cancellations, and contribution.
- Measure revenue per completed visit.
- Split results by service mix.
- Watch demand before changing prices.
- Use packages to lift ticket.
If a higher ticket drops bookings, the gain can disappear fast. On a base of 362 visits a month, even a small mix shift can move cash flow by thousands, so keep the change tied to real demand and real margin.
2
Clinician Labor Model
Clinician Labor Mix
Clinician labor mix drives take-home fast because pay is tied to each completed visit, not just booked demand. The first-year model starts with 1 Lead RN, 2 Senior RNs, 3 Staff RNs, 2 Part-Time RNs, and 1 Event RN. At 5% of revenue per visit, labor stays variable until fixed pay like the $80,000 Lead RN salary starts to pressure margin.
Here’s the quick math: on $80,580 monthly revenue, the 5% visit pay is about $4,029 before admin wages. If the owner can legally work as a clinician, owner-clinician pay can keep more margin early. Hired RN models can scale volume, but only if utilization stays tight and scope rules are followed; otherwise payroll rises faster than completed visits.
Tighten Pay per Visit
Track completed visits, revenue per visit, RN utilization, and Lead RN salary each week. Compare paid clinical hours to billable hours so you can see where time leaks. If utilization is soft, pause adds to staffing before you add more routes or event shifts.
- Completed visits by RN type
- Realized revenue per visit
- Billable hours per clinician
- Lead RN salary load
Test owner-clinician coverage against hired RN coverage. The best mix is the one that protects scope compliance and keeps labor near the 5% variable pay target while the $80,000 supervisory role does not crowd out owner draw.
3
Supply Margin And Waste Control
Supply Margin And Waste Control
Supply cost is a small line item, but it still moves owner pay. In year one, COGS is 12% of revenue: 8% for IV fluids and formulations plus 4% for medical supplies. On a $223 average ticket, that is about $26.76 per visit before labor and travel, so waste or supplier price drift cuts straight into cash flow.
By year five, modeled COGS falls to 10%. On the first-year monthly revenue of $80,580, that shift is about $1,611.60 more gross profit per month. The risk is simple: overbuying, expired stock, and loose purchasing rules eat margin fast, even if visit volume stays strong.
Track COGS Per Visit And Waste
Measure supplies by cost per completed visit, not by total spend. Track purchase price, units used, expiration loss, and on-hand inventory for fluids and medical supplies. If the mix stays near 12%, you know the model is on plan; if it drifts higher, the owner’s draw gets squeezed before staffing or travel even show up.
Use standardized ordering, tighter par levels, and expiration checks to cut waste. Here’s the quick math: every 1% drop in COGS on $80,580 monthly revenue saves about $805.80 per month. That’s real cash that can fund payroll, travel, or owner profit without needing more bookings.
4
Route Density And Travel Efficiency
Route Density
Route density means how many paid visits fit into one service area and one shift. In year one, vehicle and travel expense is modeled at 2% of revenue, or about $1,612 a month on $80,580 in monthly revenue. That cost falls to 1% by year five. Tight routes raise visits per day and protect margin; wide routes add drive time, mileage, and paid gaps that come straight out of owner profit.
What this hides is simple: revenue can look fine while cash flow weakens if too much time is spent in the car. Inputs are service-area size, visits per day, miles per visit, cancellations, and schedule gaps. If route planning slips, the owner keeps paying for labor and fuel without adding billable sessions.
Cut Paid Miles
Track paid visits per route hour, miles per completed visit, and drive time as a share of shift time. Then cluster appointments by zip code, time block, and clinician so one run serves more booked visits. The goal is fewer dead miles and more billable stops, which lifts daily capacity and leaves more room for owner pay.
Test tighter service boundaries before adding more staff or more territory. If a wider area creates long gaps, it should be priced in or dropped. A route that saves even a small slice of the $1,612 monthly travel cost can improve gross margin and free cash for the owner much faster than chasing extra low-density bookings .
5
Repeat Customer Acquisition
Repeat Clients and Referrals
Repeat clients, referrals, memberships, and corporate wellness accounts lift take-home income by keeping more drips booked without paying for every new visit. That matters because the model adds a Marketing Manager after year one at 0.5 FTE, or $32,500 in year two and $65,000 from year three, so recurring demand has to cover a bigger fixed cost base.
Track booked revenue, not leads. A lead only helps if it turns into a paid drip, and the risk is assuming every client becomes recurring. The real win is lower acquisition cost per completed drip and steadier RN utilization, which supports more predictable owner draw.
Measure Repeat Revenue by Source
Split booked revenue into repeat clients, referrals, memberships, and corporate wellness accounts. That shows which source is filling the schedule and which one is just creating interest. If one source is thin, the business still depends on paid marketing, so cash flow gets tighter and owner pay gets less stable.
- Track repeat booking rate monthly.
- Count completed, paid drips only.
- Compare referral and membership revenue.
- Watch corporate accounts by booked visits.
One clean test: if recurring bookings do not rise, the marketing manager cost can outpace margin. When repeat demand is steady, the owner buys less traffic and keeps more profit from each completed drip.
6
Compare low, base, and high owner-income scenarios
Owner income scenarios
Owner income rises fast as visit volume, ticket size, and margin improve from ramp to scale. These cases show the range from early launch to fuller capacity.
| Scenario | Low CaseEarly ramp | Base CaseCore case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the lower-income ramp case with modest volume and a tight operating margin. | This is the modeled midpoint case with steadier demand and more efficient staffing. | This is the stronger-income case with higher visit density and better margin capture. |
| Typical setup | First-year ramp at 362 visits per month, $223 average ticket, and 81% contribution margin, with about $80,580 monthly revenue and $29,528 monthly EBITDA after owner salary. | Year three at 1,102 visits per month, $230 average ticket, and 83% contribution margin, with about $253,020 monthly revenue and $163,848 monthly EBITDA after owner salary. | Year five at 2,115 visits per month, $238 average ticket, and 85% contribution margin, with about $503,530 monthly revenue and $378,092 monthly EBITDA after owner salary. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $29,528/moLower income | $163,848/moMain case | $378,092/moHigh upside |
| Best fit | Use this to stress-test the business if bookings build slowly and capacity stays under plan. | Use this as the main planning case for hiring, cash use, and owner pay expectations. | Use this to test what happens if demand stays strong and the team keeps most of the schedule full. |
Planning note: Scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions; they are before taxes, debt, capex, and reserves.
Related Products
- In-Home IV Therapy Porter's Five Forces Analysis
- In-Home IV Therapy BCG Matrix
- In-Home IV Therapy Business Model Canvas
- 7 Critical KPIs for Scaling In-Home IV Therapy
- In-Home IV Therapy Business Plan Template in Pre-Written Word
- How to Increase In-Home IV Therapy Profitability in 7 Steps
- Running Costs for In-Home IV Therapy: A Monthly Financial Breakdown
- In-Home IV Therapy Startup Costs: $165K Setup, $828K Cash Need
- In-Home IV Therapy Financial Model Template in Excel
- How To Open An In-Home IV Therapy Business In 8–16 Weeks
- How to Write an In-Home IV Therapy Business Plan: 7 Action Steps
- In-Home IV Therapy Marketing Mix
- In-Home IV Therapy Marketing Plan
- In-Home IV Therapy Business Proposal
- In-Home IV Therapy PESTEL Analysis
- In-Home IV Therapy Pitch Deck Example Editable PPTX
- In-Home IV Therapy Business SWOT Analysis
- In-Home IV Therapy Value Proposition Canvas
Frequently Asked Questions
The first-year model pays the owner a $120,000 salary, or $10,000 per month It also shows about $354,338 in annual EBITDA after modeled payroll, fixed overhead, and variable costs That profit is not the same as cash you can take home because taxes, debt, capex, and reserves still come next