 Time to Open8-16 weeksSetup window
Time to Open8-16 weeksSetup windowHow to Open an Independent Medical Examination Service in 8-16 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open8-16 weeksSetup window  Launch Sequence5 stagesCompliance first
Launch Sequence5 stagesCompliance first Key BottleneckLicense gateProvider coverage
Key BottleneckLicense gateProvider coverage First Revenue StepPaid examsBooking live
First Revenue StepPaid examsBooking live


Key Takeaways
- Physician panel readiness is the launch bottleneck.
- Compliance setup must come before first referral.
- Outreach should match specialty coverage and pricing.
- Capacity and cash timing must support operations.
Time to Open8-16 weeksSetup windowLaunch Sequence5 stagesCompliance firstKey BottleneckLicense gateProvider coverageFirst Revenue StepPaid examsBooking liveLaunch timeline
Short web summary of the launch plan; the XLSX export includes the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Compliance
- State rule review
- Policy drafts
- Consent forms
- Compliance signoff
Physician panel
- Specialty list
- Recruit examiners
- Credential checks
- Availability grid
- Onboard physicians
Exam site
- Secure exam space
- Room layout
- Privacy buildout
- Telehealth setup
Records intake
- Intake workflow
- Upload portal
- Chain log setup
- Intake testing
Reports and billing
- Report template
- QA checklist
- Billing rules
- Denial process
Referrals and launch
- Referral list
- Outreach scripts
- Pilot cases
- Feedback review
Can the Independent Medical Examination Service financial model prove the launch plan?
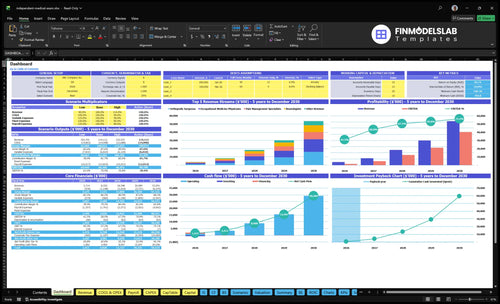
Yes—the dashboard tests revenue, costs, cash needs, assumptions, and break-even logic. Open the Independent Medical Examination Service Financial Model Template.
Financial model highlights
- 50 examiners in year one
- 8-20 exams per examiner
- 35%-50% capacity ramp
- $309,500 monthly revenue
- Runway and break-even path
How long does it take to start an IME company?
An Independent Medical Examination Service can usually launch in 8-16 weeks. It moves faster if physicians, exam rooms, billing terms, and referral relationships already exist, and it takes longer if you start from zero and must recruit specialists, verify credentials, build records workflow, or negotiate payer requirements. The Year 1 model starts with 50 examiners across five specialties—orthopedic, neurology, pain management, psychiatry, and occupational medicine—so first case scheduling depends on coverage in those areas.
Launch speed
- 8-16 weeks is the practical range
- Faster with existing physicians and rooms
- Slower from zero setup
- 50 examiners drives Year 1 coverage
What changes the clock
- Recruiting specialists adds time
- Credential checks add time
- Records workflow adds time
- Payer terms and first cases add time
How do IME companies get clients?
IME companies get clients by earning trust with adjusters, TPAs, workers’ comp admins, plaintiff and defense attorneys, employers, nurse case managers, and claims teams, then proving credibility, specialty coverage, fast turnaround, and defensible documentation. Revenue starts only when a paid exam is completed and billed, and in Year 1 a specialty price of $800-$1,500 per exam helps test referral sources and billing setup. For cost planning, see What Are Operating Costs For Independent Medical Examination Service?
Who buys
- Insurance adjusters need clear files
- TPAs want clean scheduling
- Defense attorneys need defensible reports
- Employers want faster claim answers
What wins work
- Sell neutrality first
- Show specialty coverage
- Promise report turnaround
- Charge $800-$1,500 per exam
Do you need a license to start an IME business?
No, an Independent Medical Examination Service usually does not need a medical license just to coordinate exams, but every physician who performs an IME must be properly licensed and qualified; verify the operating rules before booking the first referral, and track them with What Are The 5 KPI Metrics For Independent Medical Examination Service Business?. Treat readiness as 100% verification of entity registration, examiner license, specialty fit, records handling, and report standards.
Verify Before Launch
- Register the business entity first
- Check state medical board rules
- Confirm each physician license
- Match specialty to claim type
Control Referral Risk
- Follow workers’ compensation IME rules
- Protect records under HIPAA
- Keep HIPAA records for 6 years
- Run conflict checks every case
Define what must be ready before accepting IME referrals
Launch readiness checklist
Use this go-live approval checklist before opening to confirm compliance, staffing, workflow, and cash are ready.
Compliance
- Business registration filedCritical
You need a legal entity before contracts, banking, and billing start.
- State licensure scope confirmedCritical
Each state rule can change who may examine and report.
- Workers comp rules mappedCritical
Workers' compensation cases need the right process before first referral.
- Professional liability reviewedHigh
Coverage must fit impartial exams, reports, and legal exposure.
Examiners
- Lead examiner roster signedCritical
No roster means no exams, so revenue stalls on day one.
- Conflict screens clearedCritical
Impartiality breaks trust and can void cases.
- Availability meets forecastCritical
The model assumes enough examiner time to handle booked cases.
- Backup coverage namedHigh
A backup keeps cases moving when a specialist is out.
Site flow
- Exam rooms securedHigh
You need private rooms for fair exams and smooth handoffs.
- Accessibility path confirmedHigh
Patients and attorneys need clear access without delay.
- Consent script approvedCritical
Consent and notice steps must be clear before the exam starts.
- Appointment flow testedHigh
Scheduling breaks fast if the first booking path is clumsy.
Records
- HIPAA workflow approvedCritical
Protected records need clear handling before any case file moves.
- Secure file transfer testedCritical
Files must move securely or case handling is blocked.
- Report template approvedHigh
A standard report keeps findings consistent and usable in court.
- Quality review step liveCritical
Reports without review can miss errors that hurt case quality.
Referrals
- Referral intake liveCritical
No intake path means no case flow from insurers or counsel.
- Billing terms signedHigh
Payment terms should be clear before the first report goes out.
- First referral channel activeCritical
Revenue starts only when at least one referral source is live.
- Notice letters readyMedium
Clear notices cut confusion and prevent avoidable reschedules.
Finance
- Cash runway covers Month 2Critical
Minimum cash hits $796k in Month 2, so opening cash must cover the dip.
- Assumptions match forecastHigh
The case volume, price, and capacity inputs must match the launch plan.
- Fixed costs loadedHigh
Rent, insurance, cloud, legal, telecom, and admin costs must be funded.
- Go-live signoff completeCritical
Do not open until compliance, staffing, records, and cash all pass.
Which launch drivers decide IME opening readiness?
1Physician Panel Readiness
50 examinersA complete, credentialed panel is the opening gate, and delays can stretch launch into an 8-16 week build.
2Compliance And Neutrality Standards
Go-live gateSet neutrality, licensure, HIPAA, and conflict rules first, or disputes and delays will slow the launch.
3Referral Channel Development
Pre-openStart outreach before opening month so the first paid exams arrive as soon as the panel is ready.
4Records And Report Workflow
35-50% capSecure intake and report drafting keep turnaround realistic while volume sits in the 35% to 50% Year 1 band.
5Scheduling And Site Operations
20/mo eachTight scheduling and site handoffs protect utilization, and missed appointments can damage referral trust fast.
6Pricing Billing Capacity Planning
$309.5K/moPrice by specialty in the $800 to $1,500 range, and cash model clears month-one revenue at $309.5K before overhead.
Physician Panel Readiness
Physician Panel Readiness
For an Independent Medical Examination (IME) service, the physician panel is the first opening gate. Year 1 assumes 50 physicians across 15 orthopedic surgeons, 10 neurologists, 8 pain management specialists, 5 psychiatrists, and 12 occupational medicine physicians; if one specialty is thin, referrals stall because clients want credible coverage from day one.
Readiness means licenses checked, schedules open, conflicts screened, report standards accepted, and turnaround expectations clear. One weak specialty can slow booking, delay first revenue, and make the launch look bigger than the real panel can support.
Verify backup coverage before open
Before launch, confirm every physician’s license, availability, conflict rules, and report template, then map a backup examiner for each high-demand specialty. One line matters here: no verified panel, no first referral.
- Check state licenses and expirations.
- Lock open calendars by specialty.
- Screen conflicts before intake.
- Document report and turnaround rules.
If a specialty has no backup, a single cancellation can create a gap in day-one capacity and weaken client trust fast.
1
Compliance And Neutrality Standards
Compliance and Neutrality Standards
If IME compliance is not built before the first referral, opening slips fast. You need state-specific rules, medical board requirements, workers compensation procedures, physician licensure, consent steps, and HIPAA-safe record handling in place so the first case can move from intake to report without legal or privacy gaps.
Neutrality is the launch risk control. This service has to work for legal, insurance, employer, and workers compensation cases without looking biased. If conflict screening and defensible exam protocols are weak, reports get challenged, referrals slow down, and first-day operations turn into rework instead of revenue.
Build the Compliance File First
Before opening, verify the rules for every state you plan to serve, then map them into one intake checklist. That checklist should cover licensure, consent, records handling, conflict checks, exam standards, and report language. One clean process matters more than speed on day one.
- Confirm physician licensure by state.
- Screen conflicts before scheduling.
- Document consent steps for each case.
- Use HIPAA-safe file transfer only.
- Standardize defensible exam notes.
Any gap here can delay the first exam, hold up report delivery, or trigger a dispute with a payer or attorney. That means more cash tied up in unfinished work and less confidence from referral sources. A tight process keeps the first cases clean, consistent, and ready to bill.
2
Referral Channel Development
Pre-Open Referral Pipeline
If outreach starts after opening month, the calendar stays empty while fixed costs still run. For an IME service, the first revenue step is a completed paid exam, so the referral list has to exist before day one. Match outreach to the Year 1 specialty panel and the $800 to $1,500 pricing band, or clients may see weak coverage and delay booking.
Target insurance carriers, third-party administrators, claims adjusters, workers compensation administrators, plaintiff and defense attorneys, employers, nurse case managers, and claims organizations. Lead with specialty coverage, neutral reports, scheduling reliability, and turnaround discipline. That is what turns interest into the first scheduled case.
Build First-Case Conversion
Before opening, verify the referral list, decision makers, intake steps, and who can actually send a case. Tie each outreach path to a specific service line, so a payer asking for neurology, orthopedics, or psychiatry can be booked without delay. If the panel and the pitch do not match, launch traction will be weak.
Lock the launch sequence in writing: specialty coverage, pricing, scheduling response time, and report turnaround. Use a simple rule for readiness: if you cannot quote the exam, schedule it, and confirm the report handoff in one pass, the referral channel is not ready for opening week.
- Confirm referral contacts before open
- Map each specialty to a payer
- Publish the turnaround promise
- Test first paid exam workflow
3
Records And Report Workflow
Records And Report Workflow
Day-one IME quality depends on a tight records-and-report workflow: secure intake, file transfer, medical record indexing, physician review, report drafting, quality assurance, and final delivery. If any step is slow, the first cases slip, and you can’t credibly promise turnaround that the process cannot support.
The big launch risk is volume. The source assumptions only support 35%-50% Year 1 capacity by specialty, so records volume has to be tested before referrals scale. Weak handling here creates delays, messy documentation, more physician rework, and lower payer confidence from the first month.
Test Records Flow Before You Open
Before launch, run a full test on the first case path and time each step. Confirm secure intake, file naming, indexing, reviewer assignment, draft templates, QA sign-off, and final delivery all work with real records, not just a mock file. One broken handoff can stall the whole case queue.
- Verify secure intake and transfer
- Assign indexing and QA owners
- Set specialty-specific turnaround limits
- Test record volume against capacity
Do not open with broad turnaround promises unless the workflow already supports them. If records arrive faster than staff can index and route them, first-day service quality drops fast, and the business spends more time fixing reports than finishing them.
4
Scheduling And Exam-Site Operations
Scheduling And Exam-Site Operations
For this IME business, scheduling is not admin work; it is the gate to opening on time. The first day only works if claimant notices, physician calendars, interpreter support, room access, and day-of-exam handoffs are already set, because the 12 occupational medicine physicians at 20 monthly exams each and 50% modeled capacity still equal 120 exams a month to coordinate.
Weak scheduling shows up fast as missed appointments, empty rooms, and complaints from payers or attorneys. The launch risk is not just lost revenue; it is damaged trust, since one no-show can force rebooking, delay reports, and make the panel look unreliable before the service has a track record.
Build the day-one booking playbook
Before opening, verify the full chain: notice template, confirmation call or message, interpreter booking, room assignment, accessibility check, cancellation rule, and who hands the claimant off when they arrive. Keep a simple schedule log so every case has one owner and one status.
Test the process with early cases using the real physician calendar, not a mock version. If the calendar, room, or interpreter step breaks, block the slot before referral outreach starts, because the business can only scale when booked exams actually happen on time.
- Confirm physician calendar access.
- Block rooms before sending notices.
- Prebook interpreter coverage.
- Publish cancellation rules clearly.
- Assign a day-of-exam handoff owner.
5
Pricing, Billing, And Capacity Planning
Pricing, Billing, And Capacity Planning
If pricing or billing is off, the clinic may be open but the business still runs short on cash. This driver sets the price card, client terms, contractor pay, and monthly exam load, so it decides whether day-one operations can fund physicians, records work, and scheduling without a cash gap.
The model assumes Year 1 prices from $800 for occupational medicine to $1,500 for psychiatry, with about $309,500 in monthly revenue at stated capacity before fixed overhead. If medical examiner payouts run at 120% and record retrieval fees hit 25%, margin and runway change fast.
Test cash timing before launch
Build the billing test around the first paid exam, not the forecast. Confirm who bills the client, when invoices go out, when payors pay, when contractors get paid, and how record fees are recovered. If cash lands late, launch slips.
- Set prices by specialty.
- Match invoices to collections.
- Document contractor pay terms.
- Cap volume to staffed capacity.
Before opening, tie each specialty’s monthly exam target to real staffing and billing load. If referral ramp is slow, hold back spend on extra scheduling and physician slots; if volume shows up faster than cash, tighten terms before the backlog hits.
6
Related Products
- Independent Medical Examination Service Porter's Five Forces Analysis
- Independent Medical Examination Service BCG Matrix
- Independent Medical Examination Service Business Model Canvas
- What Are The 5 KPI Metrics For Independent Medical Examination Service Business?
- Independent Medical Examination Business Plan Template in Pre-Written Word
- How Increase Independent Medical Examination Service Profits?
- What Are Operating Costs For Independent Medical Examination Service?
- Independent Medical Examination Startup Costs: $796K Cash Need
- Independent Medical Examination Financial Model Template in Excel
- How Much an Independent Medical Examination Owner Can Make at 309 Cases/Month
- How To Write An Independent Medical Examination Service Business Plan?
- Independent Medical Examination Service Marketing Mix
- Independent Medical Examination Service Marketing Plan
- Independent Medical Examination Service Business Proposal
- Independent Medical Examination Service PESTEL Analysis
- Independent Medical Examination Service Pitch Deck Example Editable PPTX
- Independent Medical Examination Service Business SWOT Analysis
- Independent Medical Examination Service Value Proposition Canvas
Frequently Asked Questions
Start with specialties that match your referral market The researched Year 1 panel uses 15 orthopedic surgeons, 10 neurologists, 8 pain management specialists, 5 psychiatrists, and 12 occupational medicine physicians That mix supports workers compensation, injury, disability, and medical-legal cases Don’t add a specialty until you can staff it, schedule it, and review reports well