 Owner income$199k to $4.6M
Owner income$199k to $4.6MHow Much Integrative Medicine Clinic Owners Make In A 5-Year Model

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$199k to $4.6M  Net margin16% to 61%
Net margin16% to 61% Revenue for target pay$1.25M
Revenue for target pay$1.25M Business difficultyHard
Business difficultyHard


In the researched five-year model, clinic profit before personal taxes, debt service, reserves, and owner distributions ranges from $384k in Year 1 to $47M in Year 5 If the owner also fills the Medical Director role, the modeled $240k annual salary is separate from clinic profit This planning view covers revenue, margins, costs, owner role, and reserves, but excludes personal taxes, debt terms, physician salary benchmarking, and guaranteed earnings
Owner income$199k to $4.6MNet margin16% to 61%Revenue for target pay$1.25MBusiness difficultyHardWant to test your owner income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the financial model?
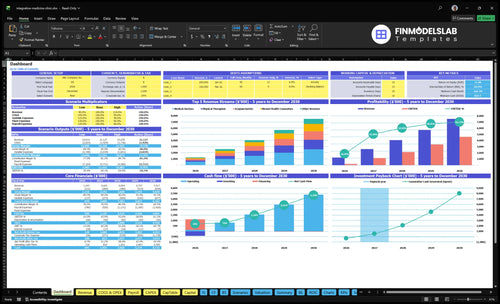
See owner income in the Integrative Medicine Clinic Financial Model Template: dashboard, assumptions, staffing, revenue, costs, cash flow.
Owner-income model highlights
- Medical Director salary split
- Revenue, margin, overhead
- Low, base, high cases
Can an integrative medicine clinic owner earn more by seeing patients?
Yes, an Integrative Medicine Clinic owner can earn more by seeing patients if they’re licensed and working in a billable clinical role; see How Increase Profits For Integrative Medicine Clinic? for the profit side. In the researched model, the Medical Director salary is $240,000/year, while clinic profit is $384,000 in Year 1 and $47M in Year 5 before taxes, reserves, debt, and distributions.
Owner-provider upside
- Earns clinical salary if licensed
- May receive management pay
- May receive profit distributions
- Salary plus distributions can stack
Owner limits
- Non-clinical owners can’t bill medically
- Licensing rules control income type
- Supervision rules affect service delivery
- Entity rules affect distributions
Can an integrative medicine clinic owner make more by hiring providers?
Yes—if provider schedules fill at profitable rates, hiring can raise owner income at an Integrative Medicine Clinic. The model grows from 7 providers in Year 1 to 26 providers in Year 5, with monthly visits rising from 583 to 3,161 and annual revenue rising from $125M to $752M. Utilization moves from 50% to 65% during early ramp-up to 85% to 88% by Year 5, but weak clinician pay, supervision, billing, or admin systems can drag margin down.
When hiring helps
- 7 providers scale to 26
- Monthly visits rise to 3,161
- Revenue grows to $752M
- Utilization reaches 85% to 88%
When payroll hurts
- Weak compensation cuts margin
- Poor supervision slows output
- Billing gaps delay cash
- Admin gaps block scale
Which integrative medicine services are most profitable?
If you’re mapping the economics of How To Launch Integrative Medicine Clinic Business?, the highest-price service is Medical Doctors, so they are the strongest revenue line on a per-visit basis. Year 1 collected prices are $250, $180, $160, $150, and $120; by Year 5 they rise to $290, $200, $180, $170, and $140.
That means Medical Doctors and then Physical Therapists lead on price, but the real margin is limited by staffing and visit capacity, not just the ticket price. Longer consults, programs, memberships, and products can lift revenue per patient, but they also use more time, so the clinic’s throughput matters a lot.
Top price lines
- Medical Doctors: $250 to $290
- Physical Therapists: $180 to $200
- Mental Health Counselors: $160 to $180
- Nutritionists: $150 to $170
Margin reality
- Gross margin is modeled at 895% to 915%
- Supplies and lab fees are already netted out
- Service-level payroll is not provided
- Capacity can cap margin fast
Want the six income drivers?
1
583-3,161Patient Volume
More visits drive the biggest jump in revenue, since the clinic scales from 583 to 3,161 monthly visits.
2
$178-$198Collected Revenue
Higher cash collected per visit lifts take-home income without needing the same jump in volume.
3
50%-88%Utilization
Better provider use pushes output higher and spreads staff cost across more billable care.
4
$120-$290Service Mix
A richer mix of higher-priced visits raises revenue per slot and improves margin.
5
$22K+$675K-$1.23MOverhead
Keeping fixed rent, systems, and wage load in check protects EBITDA as the team grows.
6
Policy gapReserve Policy
No reserve rule is set, so retained cash, debt service, and owner draws need a clear policy.
Integrative Medicine Clinic Core Six Income Drivers
Patient Volume And Appointment Capacity
Patient Volume and Appointment Capacity
More completed visits are the main top-line lever here. Monthly patient visits rise from 583 in Year 1 to 3,161 in Year 5, and revenue moves with it from $1,039k to $6,264k per month. The key is simple: this only helps if the clinic completes and collects the visit, not just books it.
The owner’s income improves when visit growth outpaces added staffing and overhead. Empty provider time, cancellations, and weak follow-up can leave cash on the table, even with a full calendar. So the real metric is collected visits per month, because that is what turns capacity into cash for payroll, taxes, and profit draws.
Track Completed Visits, Not Bookings
Forecast from completed visits × collected revenue per visit. If collections hold, more visits should lift profit; if they slip, the schedule can grow while owner pay stalls. Track provider slots, show rate, rebook rate, and month-end collections together so capacity, cash, and staffing stay in sync.
Use a tight follow-up loop: confirm visits 48 hours ahead, rebook before checkout, and review no-shows every week. That protects cash flow and keeps providers busy. A one-line test: if open slots stay empty for two weeks, the issue is usually recall, retention, or schedule design, not demand alone.
- Completed visits per provider
- Cancel and no-show rate
- Collected visits by month
- Fill rate on open slots
1
Average Collected Revenue Per Visit
Average Collected Revenue Per Visit
This is the cash the clinic actually collects per visit, not the fee on the chart. It rises from about $178 in Year 1 to $198 in Year 5, so even small collection gains feed owner pay faster than higher listed charges that never get paid.
Track visit count, listed price, cash collected, discounts, and payer mix. Year 1 price ranges run $120-$250 and Year 5 ranges run $140-$290, but if realized collections stay flat, the gap is leakage. One clean rule: higher realized collections = higher take-home income.
How to raise collected revenue
Set a weekly scorecard that separates billed charges from cash collected. Here’s the quick math: a $20 lift per visit adds $2,000 for every 100 visits before overhead. That matters because collection discipline, package design, cash-pay pricing, and payer mix decide what the owner can actually draw.
- Track cash by service line.
- Audit discounts and write-offs.
- Prepay packages when possible.
- Review payer mix monthly.
2
Provider Mix And Utilization
Provider Mix And Utilization
Provider mix is the split between medical doctors, acupuncturists, nutritionists, and other clinicians. Utilization means booked time divided by available time. In this model, provider count rises from 7 in Year 1 to 26 in Year 5, while utilization moves from 50% to 65% in Year 1 to 85% to 88% in Year 5. More staff raises capacity, but only booked visits create margin.
The owner’s income improves when those added hours turn into collected visits faster than wages rise. The wage schedule climbs from $675k to $1.231M per year for listed roles, including payroll taxes, benefits, contractor fees, and supervision where needed. If hiring runs ahead of demand, labor costs hit cash flow before revenue catches up, and profit available for owner pay shrinks.
Track Booked Hours Before You Hire
Measure booked hours, available hours, and completed visits by role each month. The useful check is simple: if a clinician’s schedule stays below the target utilization band, that seat is costing money. One clean rule: do not add a full-time provider until current providers are close to the upper end of their range and follow-up demand is already in the pipeline.
Build staffing from demand, not hope. Test whether each role lifts collected visits enough to cover its share of the $675k to $1.231M wage load plus overhead. If a service line can’t hold 85%+ utilization, keep it part-time, contract-based, or shared across roles so owner income stays tied to margin, not headcount.
3
Service Mix And Program Margin
Service Mix Drives Margin
The mix of medical visits, therapies, counseling, nutrition, programs, and products changes both collected revenue and owner pay. In this model, visit prices run from $120 to $290, with Medical Doctor visits at the top end and acupuncture at the low end. The quick math is simple: more time in higher-priced services raises gross margin per slot, while a calendar filled with low-priced or low-capacity visits can cap profit.
What matters is not just volume, but the revenue per chair hour and per provider hour. The model shows gross margin after supplies and labs improving from 89.5% to 91.5%, so small mix shifts can move take-home income fast. One low-margin visit type, repeated all month, can crowd out better-paying work and leave the owner with less cash after payroll and overhead.
Track Revenue Per Service Type
Build a monthly mix report by service line: completed visits, collected dollars, supply cost, lab cost, and provider time. Use collected revenue per visit, not posted fees, and split it by medical visits, therapies, counseling, nutrition, programs, and products. That shows which services earn enough after direct costs to support owner draw.
Set a target mix before opening the schedule. If higher-priced doctor visits are scarce, or low-price services take too much clinician time, margin slips even when the calendar looks full. Watch revenue per provider hour, then adjust pricing, staffing, and block scheduling so the highest-value services get the best slots.
4
Fixed Overhead And Administrative Costs
Fixed Overhead Pressure
$221k in fixed monthly overhead includes $125k rent, $35k insurance, $22k EHR and IT, $18k utilities, $12k maintenance, and $900 office supplies. These costs hit the owner before one more visit is collected, so income can stay tight even when patient volume grows.
In Year 1, fixed costs equal 213% of revenue, then drop to 35% by Year 5. The risk is paying for underused space and admin staff too early; listed wages add $563k to $1.026M per month, so slow demand can wipe out owner draw fast.
Control Overhead Before Hiring
Track fixed cost per collected visit, space use, admin headcount, a nd wage run rate. If visits lag, delay lease expansion and nonessential hires. The key test is simple: does each added room, admin role, or software line improve collected revenue enough to pay for itself?
Use a monthly budget that separates fixed overhead from variable clinic costs, then compare it with collected revenue, not booked visits. If the overhead ratio stays near 213%, owner pay is being funded by growth hope, not cash. Cut waste first, then add capacity.
- Monitor rent, payroll, and IT monthly.
- Freeze hiring until demand justifies it.
- Measure collected visits per room.
- Watch admin labor before adding space.
5
Reserves, Debt, And Distribution Policy
Pay Yourself From Leftover Cash
Available cash is not the same as taxable income or guaranteed owner pay. This model gives no fixed reserve or debt-service assumption, so distributions should happen only after payroll, tax reserves, equipment needs, marketing, debt payments, and working capital are covered. In Year 1, profit is only $384k before those uses.
Here’s the quick math: a clinic can look profitable and still run short if cash leaves too early. By Year 5, profit reaches $47M before owner-level deductions, so the main risk shifts to over-distributing cash the clinic still needs to operate. One clean rule: business first, owner second.
Use a Draw Waterfall
Track a monthly cash waterfall: collected revenue, payroll, tax reserve, debt service, equipment, marketing, and working capital. Only the leftover cash should fund owner draws. That keeps pay tied to real cash, not booked profit.
Set a written trigger for distributions, like no draw until the reserve target is funded and the next debt payment is covered. Recheck it after hiring, slow collections, or new equipment buys. If collections dip, owner pay should flex down before payroll or vendor bills do.
- Monthly collected cash
- Payroll and taxes
- Debt payment due dates
- Equipment and marketing spend
- Working capital target
6
Compare low, base, and high owner-income scenarios
Owner income scenario table
Owner income moves with visit volume, pricing, and fixed overhead. The high case only works if utilization stays strong and staffing economics stay tight.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | This is the lower earnings path built on Year 1 operating assumptions. | This is the modeled mid-case built on Year 3 operating assumptions. | This is the stronger earnings path built on Year 5 operating assumptions. |
| Typical setup | Year 1 revenue is $1.247M, gross margin is 89.5%, and fixed salaries, rent, and insurance absorb most of the clinic's cash flow. | Year 3 revenue is $4.054M, gross margin is 90.5%, and the clinic runs with more doctors, therapists, and support staff at higher utilization. | Year 5 revenue is $7.517M, gross margin is 91.5%, and the model assumes strong capacity use across all provider types. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $384kLow Case | $2.1MBase Case | $4.7MHigh Case |
| Best fit | Use this to stress test a slower start with tight cash use and heavier overhead pressure. | Use this as the core operating plan for a clinic that is past launch and scaling into steadier demand. | Use this to test upside if utilization stays high and provider pay stays lean relative to volume. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Integrative Medicine Clinic Porter's Five Forces Analysis
- Integrative Medicine Clinic BCG Matrix
- Integrative Medicine Clinic Business Model Canvas
- What Five KPI Metrics Should Integrative Medicine Clinic Track?
- Integrative Medicine Clinic Business Plan Template in Pre-Written Word
- How Increase Profits For Integrative Medicine Clinic?
- What Are Operating Costs For Integrative Medicine Clinic?
- Integrative Medicine Clinic Startup Costs: $628K Funding Need
- Integrative Medicine Clinic Financial Model Template in Excel
- How to Open an Integrative Medicine Clinic in 4 to 9 Months
- How To Write A Business Plan For Integrative Medicine Clinic?
- Integrative Medicine Clinic Marketing Mix
- Integrative Medicine Clinic Marketing Plan
- Integrative Medicine Clinic Business Proposal
- Integrative Medicine Clinic PESTEL Analysis
- Integrative Medicine Clinic Pitch Deck Example Editable PPTX
- Integrative Medicine Clinic Business SWOT Analysis
- Integrative Medicine Clinic Value Proposition Canvas
Frequently Asked Questions
In the researched model, clinic profit ranges from $384k in Year 1 to $47M in Year 5 before personal taxes, reserves, debt service, and distributions If the owner also works as the Medical Director, the model includes a separate $240k annual salary That role requires proper licensing