 Owner income$991k-$2.19M
Owner income$991k-$2.19MHow Much Can A Liver Cleanse Detox Program Owner Make At 296 Starts/Month

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$991k-$2.19M  Net margin42%-71%
Net margin42%-71% Revenue for target pay$2.37M
Revenue for target pay$2.37M Business difficultyHard
Business difficultyHard


You’re modeling owner income, not detox health results In the first-year planning case, 296 monthly treatment starts create $58,300 in monthly revenue, 79% contribution margin, and about $99,100 operating profit before personal tax, capex, debt service, and reserves This is not tax advice, a personal guarantee analysis, a clinical efficacy claim, or individual legal or medical compliance advice
Owner income$991k-$2.19MNet margin42%-71%Revenue for target pay$2.37MBusiness difficultyHardWant to test your detox program owner income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. It excludes medical outcomes, personal taxes, and guaranteed distributions.
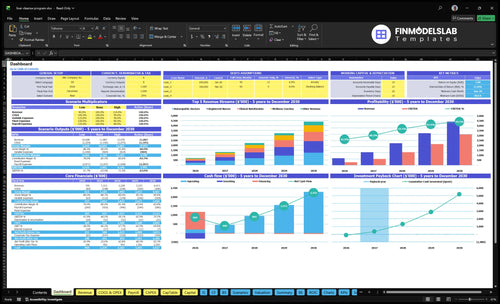
Want to see the owner-income forecast?
This screenshot shows revenue, gross margin, operating profit, cash flow, and owner pay; open the Liver Cleanse Detox Program Financial Model Template.
Owner-income model highlights
- Owner pay before tax
- Break-even starts shown
- Year 1 to 5 cases
Can a liver cleanse detox program owner make more by scaling?
Yes, the Liver Cleanse Detox Program owner can make more by scaling, but only if each added client still leaves margin after labor, compliance, and marketing. The model grows from 8 providers in Year 1 to 28 in Year 5, with monthly starts rising from 296 to 1,708 and revenue from $6996k to $441M. Owner-led delivery can help early margins, but hiring practitioners lowers per-client profit and adds risk in screening, protocol oversight, scheduling, cancellations, documentation, insurance, and compliance.
Scale helps income
- 8 providers to 28
- Starts rise to 1,708 monthly
- Revenue reaches $441M
- Added capacity must stay profitable
Margin risks to watch
- Owner-led delivery caps volume
- Hired staff cuts per-client margin
- Screening and oversight add cost
- Compliance and cancellations hurt throughput
What costs reduce liver cleanse detox program owner income?
Owner income in a Liver Cleanse Detox Program gets squeezed first by direct costs: 8% medical supplements and cleansing agents, 4% organic consumables and lab kits, 6% digital marketing and referral fees, and 3% credit card and booking fees, which leaves about 79% contribution before fixed costs. For KPI context, see What Are The 5 Core KPIs For Liver Cleanse Detox Program Business? Fixed overhead adds $19,050 a month, led by $12,500 lease, $1,800 liability insurance, $2,200 utilities and sterilization, and $850 compliant software, while $225k Year 1 payroll, reserves, capex, debt service, and practitioner wages can cut distributable cash further.
Direct cost drain
- 8% supplements and cleansing agents
- 4% consumables and lab kits
- 6% marketing and referral fees
- 3% card and booking fees
Fixed overhead load
- $19,050 monthly fixed overhead
- $12,500 clinic lease
- $1,800 liability insurance
- $2,200 utilities and sterilization
How many clients does a liver cleanse detox program need to pay the owner?
No single client count works for every Liver Cleanse Detox Program; it depends on price, margin, fixed costs, and the owner’s pay target. Using the provided economics from How To Write A Business Plan For Liver Cleanse Detox Program?, $197 average revenue and 79% contribution margin create about $155.63 per client, so $37,800 in monthly fixed costs needs about 243 monthly starts to cover overhead and the listed $120,000 annual Clinic Director salary.
Break-even clients
- $197 average revenue per start
- 79% contribution margin
- $155.63 contribution per client
- 243 monthly starts at $37,800 fixed costs
Owner pay check
- 296 planned monthly starts
- About $58,312 monthly revenue
- About $46,066 monthly contribution
- Practitioner wages not separately provided
Want the six income drivers that matter most?
1
296/moMonthly Starts
More starts lift revenue first, and every extra client helps spread fixed cost across a bigger base.
2
$197Package Price
A higher average revenue per start pushes take-home up fast because the same visit mix turns into more sales.
3
$225KLabor Cost
Year 1 payroll is about $225K, so staffing efficiency shows up directly in EBITDA and owner draw.
4
400/moDelivery Capacity
If the team can deliver 400 treatments a month, growth can scale without a matching jump in overhead.
5
$19KOverhead Discipline
Fixed overhead of about $19,050 a month sets the cash floor, and reserve discipline decides how much can be withdrawn safely.
6
6%Marketing Efficiency
Keeping marketing and referral spend near 6% protects the spread that turns revenue into distributable cash.
Liver Cleanse Detox Program Core Six Income Drivers
Package Pricing And Mix
Package Pricing And Mix
Owner pay rises when the package mix pushes average revenue per client up, but only if added delivery cost stays controlled. Year 1 pricing runs from $85 to $450, with a $197 weighted average; by Year 5, it rises to $105 to $510, with a $215 weighted average. At 296 monthly starts, every $10 increase in average revenue adds $2,960 a month before costs change.
This driver includes supervised protocols, nutrition visits, coaching, follow-ups, kits, and maintenance plans. The key inputs are start volume, package mix, and delivery cost per client. Revenue = starts × weighted average price. Premium pricing without matching supervision and compliance can raise churn and damage reputation, which cuts cash flow and owner take-home fast.
Price the mix, not the menu
Track average revenue per start, gross margin by package, and the labor time tied to each add-on. If a higher-price plan needs more follow-up, more kits, or more clinical review, build that cost into the price before you scale it. The goal is simple: more revenue per client without letting delivery cost rise faster than the extra cash.
Test price steps and package bundles against cancellations, complaints, and repeat bookings. If a premium offer needs tighter supervision, document the protocol and staff time first. That keeps the mix profitable and protects the brand while the clinic grows.
1
Monthly Client Starts
Monthly Client Starts
Monthly client starts is the main volume lever. With 296 planned starts in Year 1, 914 in Year 3, and 1,708 in Year 5, revenue scales fast once fixed costs are covered. Break-even is about 243 starts per month using Year 1 average revenue and contribution margin, so volume below that pushes owner pay down fast.
Here’s the catch: starts only help income if leads convert into paid visits without straining clinical screening, scheduling, and follow-up. High cancellation rates or slow onboarding can turn a strong lead pipeline into weak cash flow. Above break-even, cash still has to cover reserves, payroll, debt service, and capex before any owner distribution.
Track starts, not leads
Measure booked starts, show rate, cancellation rate, and days to onboarding. The key formula is paid starts ÷ qualified leads. If volume rises but screening or follow-up slows, the clinic looks busy while take-home falls. A clean start process is what turns demand into margin.
Test capacity before pushing volume. Compare starts per practitioner, then watch whether added starts increase revenue faster than payroll and admin time. If owner draws are getting squeezed, cap starts at the level where service quality stays tight and contribution stays above 243 monthly starts with room for reserves.
2
Delivery Model Capacity
Delivery Capacity
Delivery model capacity decides how many treatments you can sell and actually fulfill. One-on-one supervision supports higher prices, but it caps throughput. The disclosed source capacity is 40 monthly treatments per naturopathic doctor, 80 per registered nurse, 60 per clinical nutritionist, 100 per wellness coach, and 120 per phlebotomist before utilization.
At 40% to 60% utilization in early stages, a naturopathic doctor supports about 16 to 24 treatments a month. By Year 5, 80% to 85% utilization lifts that to about 32 to 34. If volume rises faster than screening, documentation, and protocol oversight, safety review slows and owner income falls through weaker retention and more rework.
Keep Quality Tight
Track capacity by role, not just total starts. Watch monthly treatments per provider, utilization, no-shows, onboarding time, and protocol exceptions. Here’s the quick rule: more visits only help income when each step from screening to follow-up stays controlled. If one role becomes the bottleneck, cash flow stalls even when demand is strong.
- Set weekly caps by practitioner.
- Document screening before scheduling.
- Test group or hybrid visits first.
- Review safety exceptions every week.
- Keep follow-up templates tight.
Group or hybrid delivery can lift revenue per month, but only if oversight stays tight. If the team holds 80% to 85% utilization with clean records and consistent protocols, margin and owner draw improve. If not, chasing volume adds labor strain, client complaints, and slower collections.
3
Practitioner Labor Cost
Practitioner Labor Cost
Practitioner labor is the cost of the people delivering the service, and it decides whether booked starts turn into owner take-home pay. In this model, provider headcount is included, but provider wages are not listed as direct COGS, so a mature forecast has to add them or margin will look too strong.
That matters because volume grows from 296 monthly starts to 1,708 by Year 5. Early owner delivery can help cash flow, but unpaid owner time is not free. Each added practitioner has to clear revenue per appointment, utilization, supervision needs, and margin after payroll before it earns its keep.
Test Labor Against Cash Margin
Track labor by role and by start. Use the capacity guide: 40 monthly treatments per naturopathic doctor, 80 per registered nurse, 60 per clinical nutritionist, 100 per wellness coach, and 120 per phlebotomist before utilization. Utilization moves from 40%–60% early to 80%–85% by Year 5, so staffing too early can crush cash flow.
Non-provider payroll already rises from $225k in Year 1 to $450k in Year 5, so add practitioner wages before you call profit real. The quick check is simple: if a provider cannot cover wage, supervision, and shared overhead at current starts, delay the hire or push more of the owner’s own time into the early schedule.
4
Marketing Efficiency
Marketing Efficiency
If marketing brings in leads that never start, owner pay gets squeezed fast. The key metric is CAC = marketing spend ÷ new paid clients. In Year 1, marketing and referral fees are 6% of revenue, falling to 4% by Year 5; the source model places Year 1 at about $42k a year.
Use booked starts, not lead counts, because paid demand can look strong while unqualified leads fail screening or cancel before day one. The real test is whether each new client still covers marketing plus delivery. If CAC rises above contribution profit per client, revenue can grow and cash still tighten.
Track CAC by booked start
Judge referral partners, local relationships, content, and paid leads by paid starts, not inquiries. Track CAC by channel, screening pass rate, and cancel-before-start rate so you can see which source actually creates take-home income. Here’s the quick math: if CAC goes up and conversion stays flat, owner profit falls even when lead volume looks good.
- Measure CAC by channel.
- Count booked starts only.
- Watch screening fallout.
- Compare CAC to contribution profit.
5
Overhead And Reserves
Overhead And Reserves
Fixed overhead is $19,050 per month, made up of $12,500 lease, $1,800 liability insurance, $2,200 utilities and sterilization, $850 compliant software, $600 supplies, and $1,100 maintenance. That cash leaves the clinic before the owner takes anything home, so it cuts distributable income even when the operation looks profitable on paper.
Year 1 payroll adds $18,750 per month, so the business has $37,800 in monthly fixed cash outflow before owner pay and before any reserve build. Reserves must be set aside first, not treated as leftover profit. Underfunded reserves turn profit into cash stress fast.
Fund Cash Buffer First
Track overhead by line item and hold a reserve target before any owner withdrawal. Use the monthly fixed-cost run rate of $19,050, plus $18,750 payroll, to test how many months of cash the clinic can survive if starts slow or collections slip. No reserve, no draw.
Build the reserve around the cash uses that hit hard and early: $150,000 clinic buildout, $45,000 diagnostic equipment, and $25,000 furniture. Watch lease timing, insurance renewals, and maintenance spend. A simple control is cash on hand versus fixed burn, then pay the owner only after that floor is met.
- Track monthly fixed cash burn
- Separate reserve cash from profit
- Review lease and payroll timing
- Delay owner draws until buffer exists
6
Compare lean, base, and high owner-income scenarios
Owner income scenarios
Owner income rises as treatment volume, staffing, and fixed payroll scale. These cases show how much profit may be available under low, base, and high operating paths.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | Lower earnings path built on Year 1 revenue and EBITDA, with the owner paid only if they fill the Clinic Director role. | Modeled mid case built on Year 3 performance and a fuller clinic rhythm. | Stronger earnings path built on Year 5 scale and the highest modeled output. |
| Typical setup | Year 1 is about $700k revenue and $293k EBITDA, but practitioner wages are still missing and must be added. | Year 3 reaches about $2.228M revenue and $1.317M EBITDA, with larger staffing and the same caveat on missing practitioner wages. | Year 5 reaches about $4.413M revenue and $3.113M EBITDA, with heavier staffing and the same caveat on missing practitioner wages. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $293k - $413kConservative range | $1.317M - $1.437MModeled range | $3.113M - $3.233MUpside range |
| Best fit | Use this to stress test the first operating year and the impact of missing practitioner wages. | Use this as the main planning case for lender, investor, or owner discussions. | Use this to test upside if the clinic fills capacity and keeps fixed costs under control. |
Planning note: These ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Liver Cleanse Detox Program Porter's Five Forces Analysis
- Liver Cleanse Detox Program BCG Matrix
- Liver Cleanse Detox Program Business Model Canvas
- What Are The 5 Core KPIs For Liver Cleanse Detox Program Business?
- Liver Cleanse Detox Program Business Plan Template in Pre-Written Word
- How Increase Liver Cleanse Detox Program Profitability?
- What Are Operating Costs For Liver Cleanse Detox Program?
- Liver Cleanse Detox Program Startup Costs: $803K Funding Plan
- Liver Cleanse Detox Program Financial Model Template in Excel
- How To Open A Supervised Liver Cleanse Program In 8–14 Weeks
- How To Write A Business Plan For Liver Cleanse Detox Program?
- Liver Cleanse Detox Program Marketing Mix
- Liver Cleanse Detox Program Marketing Plan
- Liver Cleanse Detox Program Business Proposal
- Liver Cleanse Detox Program PESTEL Analysis
- Liver Cleanse Detox Program Pitch Deck Example Editable PPTX
- Liver Cleanse Detox Program Business SWOT Analysis
- Liver Cleanse Detox Program Value Proposition Canvas
Frequently Asked Questions
In the first-year planning case, operating profit is about $99,100 after listed payroll and fixed overhead If the owner also fills the $120,000 Clinic Director role, pre-tax owner economics could reach about $219,100 before reserves, capex, debt service, and personal tax Add practitioner wages before treating that as take-home