 Owner income$13K
Owner income$13KMedication Synchronization Pharmacy Owner Income: $156K/Month Model

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$13K  Net margin81%
Net margin81% Revenue for target pay$192K
Revenue for target pay$192K Business difficultyHard
Business difficultyHard


A medication synchronization pharmacy service owner can make meaningful income only after refill volume covers labor, software, facility, packaging, fulfillment, and reserve needs In the researched Year 1 assumptions, 242 weekly visitors, 12% conversion, 85% repeat customers, 4 units per order, and a $39 weighted unit price produce about $264M in revenue After 11% supplies cost, 6% fulfillment cost, $936K fixed overhead, and $220K payroll, operating cash flow is about $188M before taxes, debt, reserves, and owner draw That is a planning case, not guaranteed owner pay
Owner income$13KNet margin81%Revenue for target pay$192KBusiness difficultyHardWant to test your med sync owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on revenue, margins, payroll, taxes, debt, and reinvestment.
Want to check owner income in the model?
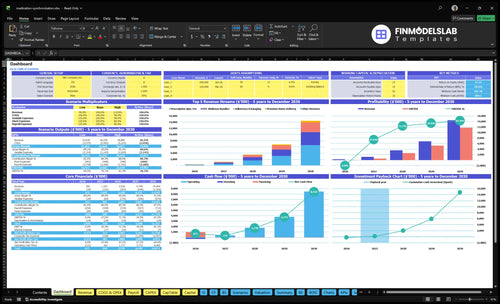
The Medication Synchronization Pharmacy Service Financial Model Template shows dashboard, assumptions, revenue, costs, reserves, and owner take-home. Open it.
Owner-income model highlights
- Owner draw capacity
- Revenue and gross margin
- Payroll ramps $220K to $549K
- Capex starts at $177K
How many medication synchronization patients are needed to pay the owner?
There isn’t one fixed patient count, but the Medication Synchronization Pharmacy Service model points to about 1,284 repeat customers as the scale needed to cover owner pay after $78K in monthly fixed overhead and about $183K in monthly payroll. The prompt also puts repeat-customer revenue at about $171 a month, and that break-even count can move fast if units per order drop below 4, repeat rate falls under 85%, or the owner keeps cash for inventory and capex.
What the owner must cover
- $78K monthly fixed overhead
- $183K average monthly payroll
- 1,284 repeat customers in Year 1
- $171 monthly revenue per repeat customer
What changes the count fast
- 4 units per order is the floor
- 85% repeat rate matters a lot
- Inventory and capex reserves reduce cash
- Lower fill profit raises patient needs
Can a medication synchronization service scale without the owner?
Yes—the Medication Synchronization Pharmacy Service can scale without the owner only if technician-led workflows, pharmacy management system controls, and pharmacist oversight keep errors, exceptions, and churn in check. In Year 1, staffing is 1 lead pharmacist, 1 technician, 0.5 delivery coordinator, and 0.5 admin FTE; by Year 5, it rises to 2 pharmacists, 4 technicians, 1.5 delivery coordinators, and 1 admin FTE, while payroll climbs from $220K to $549K. The owner’s job shifts from refill firefighting to enrollment, payer review, quality control, cash reserves, and retention.
What must hold
- Technicians handle daily sync work
- System controls catch exceptions fast
- Pharmacists review risky refills
- Churn stays under control
Where the owner moves
- Enroll more patients
- Review payer rules and claims
- Check quality and errors
- Protect cash reserves for payroll
Is a medication synchronization pharmacy service profitable?
Yes, a Medication Synchronization Pharmacy Service can be profitable, but only when refill capture, repeat use, and workflow speed beat labor, supplies, fulfillment, rent, software, and payer adjustments; track the right drivers with What Are The 5 KPIs For Medication Synchronization Pharmacy Service Business?. In the Year 1 researched case, revenue is about $264M, with $290K supplies, $158K fulfillment, $936K fixed overhead, and $220K payroll, leaving about $188M operating cash flow before taxes and reserves.
Profit drivers
- Capture monthly refills reliably
- Increase repeat prescription volume
- Batch work into fewer touchpoints
- Keep delivery exceptions low
Margin risks
- Watch PBM and DIR fees
- Control prior authorization delays
- Track low reimbursement claims
- Reserve cash for payer adjustments
Want the six main income drivers?
1
45-150/dayPatient flow
More synced patients drive the whole model, since each added visit can become repeat fills and higher monthly revenue.
2
85%-94%Repeat rate
Holding more first-time buyers turns one fill into a longer cash stream, with lifetime rising from 24 to 40 months.
3
83%-87%Fill margin
Direct costs ease as supplies fall from 11% to 9% and fulfillment from 6% to 4%, and payer mix plus PBM/DIR fees can move take-home fast.
4
$39-$46.5Unit price
The weighted ticket rises as packaging, OTC bundles, and delivery make up more of each order.
5
4-6/ordBasket size
More products per order lift revenue per patient without the same jump in visit count.
6
$220K-$549KPayroll load
Staffing must stay tight as payroll climbs with scale, or more of the gross profit gets used up.
Medication Synchronization Pharmacy Service Core Six Income Drivers
Enrolled synchronized patients
Enrolled synchronized patients
Enrollment is the base of recurring revenue, but retained active patients matter more than signups. In Year 1, 12,584 annual visitors at 12% conversion implies about 1,510 enrollments, and an 85% repeat assumption yields about 1,284 repeat customers. More active patients help cover the $78K monthly fixed overhead and payroll.
By Year 5, 775 weekly visitors, 25% conversion, and a 94% repeat rate point to a much stronger base. Churn raises outreach cost, slows refill continuity, and weakens owner draw. One clean rule: retention pays the bills.
Track repeat patients first
Measure enrolled patients, repeat rate, and monthly refill activity together. The inputs you need are visitor count, conversion rate, active retention, and the cost to re-engage patients who miss refills. If conversion rises but repeat slips, the base looks bigger while cash flow gets weaker.
- Count active patients monthly.
- Watch repeat rate by cohort.
- Separate new from retained revenue.
- Price outreach against churn cost.
Use the enrollment base to forecast whether recurring volume will cover payroll, packaging, and outreach. If retained patients fall, owner income drops fast because fixed costs do not move down at the same speed.
1
Prescriptions per patient per cycle
Refills per Patient Cycle
This driver is the number of prescriptions filled each sync cycle for one patient. In this model, it starts at 4 units per order in Year 1 and rises to 6 by Year 5, with 1 order per month per repeat customer. More chronic scripts lift revenue per enrollment, but they also add refill calls, timing fixes, and exception handling.
Here’s the quick math: more units per cycle usually means more sales, but not always more profit. The owner’s take-home rises only if added refill volume beats the extra labor, inventory planning, and payer mix drag. Patients with more prescriptions can be sticky, yet they need tighter coordination, so missed refills or slow follow-up can turn revenue into margin leakage.
Track Cycle Count, Not Just Headcount
Measure prescriptions per patient per cycle, not just enrolled patients. Track scripts per order, refill exceptions, and minutes spent per sync, then compare that against gross profit per order. If a patient’s cycle grows from 4 to 6 units but coordination time rises faster, owner draw can shrink even when revenue looks better.
Use a simple patient file for payer mix, refill date drift, and average margin by patient type. Patients with heavier chronic loads can drive more recurring revenue, but they also need more calls, prior auth work, and inventory checks. Tighten those workflows first, because cleaner cycles protect cash flow and keep labor from eating the extra refill revenue.
2
Gross profit per synchronized prescription
Gross profit per sync
Gross profit per synchronized prescription is the cash left after the $39 weighted unit price is offset by acquisition and supply cost, before overhead. With 4 units per order, order revenue is about $156; at 11% supplies cost, gross profit is about $138.84 per order before fulfillment and operating costs. That’s the margin that funds payroll, delivery, and owner pay.
Here’s the quick math: $156 × 89% = $138.84. If payer adjustments, labor, packaging, or delivery rise, gross profit falls fast even when sales look strong. The owner’s take-home depends on this spread staying wide enough after claim cuts and service costs, not just on prescription volume.
Track the realized spread
Measure realized price per unit, supplies cost %, and fulfillment cost per order. This driver only helps owner income if the gap stays intact after payment rules, packaging, and delivery. A small drop in realized price can wipe out the margin needed to cover fixed overhead and profit draw.
- Track revenue per synced order.
- Watch supply cost above 11%.
- Test delivery and labor by order.
- Flag payer cuts before month end.
If you want cleaner profit, protect the mix that supports the $39 unit price and keep exception handling tight. One owner hour saved on refill work can matter more than a few extra orders if those orders come with thin reimbursement or heavy delivery time.
3
Payer mix and PBM fees
Payer Mix and PBM Haircut
Payer mix decides how much of a synchronized prescription’s billed value becomes realized profit. Medicare Part D, commercial plans, and cash patients do not pay the same, and PBM (pharmacy benefit manager) and DIR (direct and indirect remuneration) fees can cut the take-home amount after the sale. Since the source model does not give a fee percentage, use an editable haircut in the forecast.
Test owner income after post-sale fees, not just claim revenue. Reimbursement timing, reversals, clawbacks, and performance-based adjustments can slow cash and reduce the profit available for payroll, rent, and owner draw. Two pharmacies with the same top line can end up with very different take-home pay.
Model the Net, Not the Claim
Build the model with payer shares, an editable PBM/DIR haircut, and a cash lag. Here’s the quick math: if the claim posts today but fees or clawbacks hit later, owner income falls even when sales look strong. Track net collections by payer so you know which mix actually funds payroll and owner pay.
- Split Medicare Part D, commercial, cash.
- Apply a fee haircut by payer.
- Track days to cash.
- Review clawbacks monthly.
4
Labor and workflow efficiency
Medication Sync Labor Cost
Labor is a direct owner-income lever because med sync turns each refill cycle into paid work: outreach, prior authorizations, packaging, delivery, and pharmacist review all take hours. In the model, payroll is $220K in Year 1 and rises to $549K by Year 5, so small workflow waste quickly shows up as lower profit and a smaller owner draw.
Batching refills can lower cost per cycle, but only if exceptions stay low. If every synchronized patient still needs manual calls or extra pharmacist review, labor grows faster than revenue. Here’s the quick check: track time per patient and per cycle, then compare it to monthly refill volume an d fixed payroll, because owner pay comes from what is left after labor.
Track Time, Not Just Refills
Measure the work that actually eats the day: technician time per patient, pharmacist review time per cycle, delivery hours, and owner involvement per week. If any of those rise faster than synchronized refill volume, margin gets squeezed even when sales look steady.
- Time outreach by patient.
- Log exception handling minutes.
- Separate delivery from fill time.
- Review owner hours weekly.
Use those logs to staff the right role for the right task. Batch routine refills, push simple work to technicians, and reserve pharmacist time for clinical checks and exceptions. That keeps payroll tied to volume, protects cash flow, and makes the business more likely to throw off real owner income instead of just busywork.
5
Retention, incentives, and ancillary revenue
Retention and Ancillary Revenue
Medication sync only pays off if patients stay active. In the model, repeat rate rises from 85% in Year 1 to 94% in Year 5, and customer life extends from 24 to 40 months. That means more monthly refill cycles, steadier cash, and less spend to replace lost patients. One clean line: retention is the revenue base, not new signups.
Ancillary income can lift margin, but only when it is actually approved and billed. The mix includes adherence packaging at 30% to 40%, wellness bundles at 20%, and premium delivery at 10%. Adherence incentives, clinical service fees, packaging fees, and delivery revenue are payer-dependent, so treat them as variable income, not guaranteed profit.
Track Retained Patients and Attach Rate
Watch retained patients, monthly orders per patient, and the attach rate for packaging, wellness, and delivery. The key test is simple: if retention rises but fee capture falls, owner income can still drop. Measure net cash after payer rules, supply cost, labor, and delivery time, not just billed revenue. Here’s the quick math: more months active usually means more profit, if margin holds.
Set separate forecast lines for approved fees and denied fees. Track how many patients accept each add-on, what the payer allows, and how often staff must intervene to collect or rework claims. If onboarding or refill exceptions slow the team, the extra revenue can get eaten by labor. What this hides: high retention helps most when ancillary services are cleanly documented and reimbursed.
6
Compare lean, base, and high medication synchronization owner income scenarios
Owner income scenarios
Owner income changes fast here because weekday traffic, conversion, repeat fills, mix, and staffing all move together. The scenario spread shows when launch losses turn into stable cash flow.
| Scenario | Low CaseDownside case | Base CaseBase case | High CaseUpside case |
|---|---|---|---|
| Launch model | Launch earnings stay weak while traffic, conversion, and repeat volume are still building. | Modeled earnings stabilize once refill volume and repeat use are both established. | Stronger earnings show up when traffic, conversion, and repeat fills all scale faster. |
| Typical setup | Year 1 lands near $305k revenue and -$94k EBITDA, with 242 weekly visitors, 12% conversion, 85% repeat rate, and 4 units per order. | Year 3 reaches about $3.52M revenue and $2.53M EBITDA, with 463 weekly visitors, 18% conversion, 90% repeat rate, 5 units per order, and a $42.80 weighted unit price. | Year 5 reaches about $14.46M revenue and $11.78M EBITDA, with 775 weekly visitors, 25% conversion, 94% repeat rate, 6 units per order, and a $46.50 weighted unit price. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | -$94kLaunch loss | $2.5M - $5.2MStable cash | $11.8MScale upside |
| Best fit | Use this to test launch-month cash strain and hiring timing. | Use this as the middle case for reserve planning and owner draw timing. | Use this to test upside if weekday demand and repeat usage stay strong. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Medication Synchronization Pharmacy Service Porter's Five Forces Analysis
- Medication Synchronization Pharmacy Service BCG Matrix
- Medication Synchronization Pharmacy Service Business Model Canvas
- What Are The 5 KPIs For Medication Synchronization Pharmacy Service Business?
- Medication Synchronization Pharmacy Service Business Plan Template in Pre-Written Word
- How Increase Medication Synchronization Pharmacy Service Profitability?
- What Are Operating Costs For Medication Synchronization Pharmacy Service?
- Medication Synchronization Pharmacy Startup Costs: $664k Cash Need
- Medication Sync Financial Model Template in Excel
- How to Open a Med Sync Pharmacy Service in 6 to 12 Weeks
- How To Write A Business Plan For Medication Synchronization Pharmacy Service?
- Medication Synchronization Pharmacy Service Marketing Mix
- Medication Synchronization Pharmacy Service Marketing Plan
- Medication Synchronization Pharmacy Service Business Proposal
- Medication Synchronization Pharmacy Service PESTEL Analysis
- Medication Synchronization Pharmacy Service Pitch Deck Example Editable PPTX
- Medication Synchronization Pharmacy Service Business SWOT Analysis
- Medication Synchronization Pharmacy Service Value Proposition Canvas
Frequently Asked Questions
Known startup capex totals at least $177K from pharmacy buildout, automated dispensing, delivery vehicles, and IT setup That excludes any incomplete or unlisted equipment, working capital, inventory reserves, debt costs, and owner living costs Monthly fixed overhead is $78K before payroll, and Year 1 payroll is $220K