 Owner income$237k / $1.24M / $2.58M
Owner income$237k / $1.24M / $2.58MHow Much Does A Mobile Health Clinic Owner Make? $278K-$27M Model

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$237k / $1.24M / $2.58M  Net margin31% / 67% / 80%
Net margin31% / 67% / 80% Revenue for target pay$753k / $1.85M / $3.24M
Revenue for target pay$753k / $1.85M / $3.24M Business difficultyHard
Business difficultyHard


Key Takeaways
- Completed visits drive the $753k Year 1 top line.
- Break-even is about 864 treatments per month.
- Payer mix and service mix change cash collected.
- Fixed overhead and staffing drive monthly cash needs.
Owner income$237k / $1.24M / $2.58MNet margin31% / 67% / 80%Revenue for target pay$753k / $1.85M / $3.24MBusiness difficultyHardWant to test your own owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only; not guaranteed salary, tax advice, or owner distribution advice.
Want the model behind the math for Mobile Health Clinic?
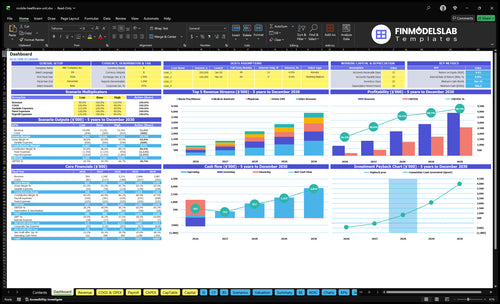
The Mobile Health Clinic Financial Model Template shows the dashboard, revenue assumptions, staffing schedules, fixed cost tabs, vehicle expenses, direct cost percentages, scenario outputs, charts, tables, owner-income projections, and break-even views. It also shows Year 1 revenue of $9,036k, Year 3 revenue of $221M, Year 5 revenue of $389M, plus operating profit before reserves of $278k, $132M, and $272M. Open the model if you want the math.
Owner-income model highlights
- Owner take-home projections
- Revenue and margin views
- Scenario and break-even tabs
What mobile health clinic operating costs reduce owner income?
Mobile Health Clinic owner income is lower than gross margin because 9% of revenue goes to direct medical costs and another 6% goes to route and billing costs. For the startup side, see What Is The Estimated Cost To Open, Start, And Launch Your Mobile Health Clinic Business? Fixed monthly overhead also includes $8k in vehicle lease or loan payments, $3k in vehicle insurance, $12k in professional liability insurance, and $1k for the electronic health record base subscription, plus $265k/year in admin wages. Reserves, taxes, reinvestment, and unsupplied clinician compensation cut distributions further.
Core cost drag
- 9% of revenue is direct medical cost.
- 6% goes to route and billing costs.
- $8k vehicle payments hit every month.
- $3k insurance adds fixed pressure.
Cash flow pressure
- $12k professional liability is fixed.
- $1k EHR base subscription runs monthly.
- $265k/year admin wages reduce take-home pay.
- Unsupplied clinician compensation cuts distributions.
How much can a mobile health clinic owner make?
A Mobile Health Clinic owner’s income should track operating profit from collected revenue, not billed charges or a fixed salary promise; see What Strategies Are You Using To Measure The Success Of Mobile Health Clinic? for the KPI view. In the supplied base case, operating profit is $278k on $9.036M revenue in Year 1, $132M on $221M in Year 3, and $272M on $389M in Year 5.
Owner earnings logic
- Track cash collected, not billed charges
- Year 1 margin: 3.1%
- Year 3 margin: 59.7%
- Year 5 margin: 69.9%
What cuts take-home
- Clinician wages can absorb cash
- Taxes and reserves reduce draws
- Billing delays slow payouts
- No contract revenue is included
How does owner-operated versus staffed mobile clinic income change?
If the owner is a licensed clinician and state rules allow it, a Mobile Health Clinic can keep more margin under an owner-operated model because labor and supervision are thinner. A staffed model can scale faster, but it adds paid providers, admin support, and tighter scheduling control, so more of the top line gets spent before profit. Here’s the quick math: monthly revenue rises from $753k in Year 1 to $3.239M in Year 5, a gain of $2.486M or about 4.3x.
Owner-led margin
- Keep more margin if licensed.
- Lower provider payroll load.
- Less admin and supervision cost.
- State rules must allow it.
Staffed scale pressure
- Year 1: 1 physician, 2 nurse practitioners.
- Year 5: 3 physicians, 6 nurse practitioners.
- More revenue means more management load.
- Vehicle use and compliance get tighter.
Want the six drivers that move owner income?
1
864/moPatient Volume
More completed visits get you over the 864-a-month break-even point and lift take-home the fastest.
2
$753K-$3.24MPayer Mix
Better payer contracts raise cash collected per visit, so the same patient flow turns into more monthly revenue.
3
308%-699%Service Mix
A better mix of physician, NP, MA, and lab visits lifts revenue per encounter and supports the margin range.
4
70%-90%Route Utilization
Tighter routes keep the vehicle busy, so each clinic day produces more billable visits and less dead time.
5
10-29 staffStaffing Model
Labor has to match demand, because too many clinicians can turn visit growth into wage drag instead of profit.
6
$18.8K/moFixed Overhead
Fixed overhead runs about $18.8K a month, so revenue must clear that floor before owner pay improves.
Mobile Health Clinic Core Six Income Drivers
Patient Volume And Clinic-Day Utilization
Completed Visit Volume
Completed visits are the cash event in a mobile clinic. Year 1 models 1,354 completed treatments per month and about $753k in revenue, while break-even is roughly 864 completed treatments per month before reserves. That gap is what funds overhead and owner draw. If completion falls below plan, collections drop fast and profit shrinks.
Capacity is not just booked demand. No-shows, travel time, setup time, and intake delays all cut clinic-day utilization. Here’s the quick math: at $5,561 average collections per completed treatment, every lost completed visit removes about that much Year 1 revenue. Track booked visits, completed visits, cancellations, and collections per visit by route.
Track Clinic-Day Fill Rate
Measure booked, completed, and canceled visits by day and stop. Compare completed visits to scheduled capacity so you can see where travel, setup, or intake is wasting time. One weak route can pull the month below the 864-visit break-even line, even when demand looks full.
Use the dashboard to test reminders, tighter scheduling windows, and repeat sites. If completion rate improves, owner cash improves without adding another vehicle. If it slips, the clinic can still look busy and lose money because the lost $5,561 per completed visit never reaches collections.
1
Payer Mix And Contract Revenue
Payer Mix
Payer mix is the split between Medicaid, private insurance, grants, employer payments, and any contract work. In the model, revenue is counted as service collections only, not billed charges, and Year 1 average collected revenue is $5,561 per completed treatment. If payer mix shifts toward slower or lower-paying sources, cash flow and owner take-home can fall even when visit volume holds.
Contracts can smooth volume, but only if payment terms are clear. The key risk is timing: billed charges are not cash, and Medicaid, private insurance, grants, and employer pay often collect on different schedules. So the owner needs to forecast collections by payer, not just visits.
Track Collections by Payer
Measure completed treatments, collected revenue per visit, and days to cash by payer type. That tells you whether a higher-volume month will actually support payroll, fuel, rent, and owner pay. One clean number matters: $5,561 average collected revenue per completed treatment in Year 1.
Build separate lines for Medicaid, private insurance, grants, employer contracts, and any community work. Test contract terms before you add them, and track what portion is collected at service date versus later. If a payer mix looks strong on paper but cash lands late, profit may not cover the month’s fixed costs.
- Track cash by payer, not billed charges
- Separate contract revenue from service collections
- Watch collection timing by payer
2
Service Mix And Revenue Per Encounter
Service Mix and Revenue per Encounter
Service mix is the share of physician, nurse practitioner, medical assistant, phlebotomist, and Driver EMT encounters. In Year 1, prices run from $30 to $150; by Year 5, they rise to $35 to $170. The spread is $120 per encounter in Year 1 and $135 in Year 5, so mix alone can move collections before volume changes.
More higher-acuity or employer-facing visits can lift revenue per encounter and help cover fixed overhead, but the tradeoff is real: supplies, kits, billing work, and clinical rules also rise. If the mix shifts toward physician and nurse practitioner work faster than direct costs rise, more cash is left for profit and owner pay. If not, the extra revenue can disappear into variable cost.
Track Mix by Visit Type
Here’s the quick math: track encounters by type, collected price per visit, and direct cost per visit. Don’t manage this at the monthly total only. A better mix is one that raises average revenue per encounter without pushing labor, supplies, and admin time up faster than collections.
- Split visits by service type
- Compare price to direct cost
- Watch collections per encounter
- Test higher-acuity route days
What this estimate hides: a richer mix can slow throughput if visits take longer or need more coordination. If that happens, revenue per encounter may rise while total owner cash falls. The key is to test mix changes against completed visits, not just posted prices.
3
Route Planning And Operating-Day Efficiency
Dense Routes, Higher Route Yield
Route density is the gap between a full day and a long drive day. When stops are close together and repeat sites return on schedule, the clinic can complete more treatments without adding a vehicle, and each lost visit can cost about $5,561 in Year 1 collections. Dense routing also supports better owner pay because the same labor and vehicle time produces more cash.
Here’s the quick math: the model puts fuel and vehicle maintenance at 4% of revenue in Year 1, then 35% by Year 5. If routes spread out, staff hours rise while completed visits fall, so margin gets squeezed from both sides. One clean line: more dead miles means less take-home income.
Measure Stops, Time, and Cash per Route
Track the inputs that show whether a route is paying for itself: revenue per route, completed treatments per stop, drive time, setup time, and cancellations by location. Compare booked visits to completed visits, because no-shows and slow intake hide the true cost of a route until payroll and fuel hit cash flow.
- Rank sites by completed treatments per stop.
- Reuse high-repeat locations first.
- Cut routes with heavy idle time.
- Test tighter stop spacing monthly.
If a location needs extra setup or creates more cancellations, price it differently or drop it. The goal is simple: keep the day dense enough that each staffed hour turns into paid care, not empty windshield time.
4
Staffing Model And Clinical Labor Cost
Clinical Staffing Cost
Staffing is the biggest swing factor in owner take-home. The model only shows admin wages, at $265k in Year 1 rising to $460k by Year 5. It does not g ive wage rates for physicians, nurse practitioners, medical assistants, phlebotomists, or Driver EMTs, so labor margin depends on how many staffed visits you can actually complete.
Here’s the quick math: if clinical hours run ahead of completed visits, cash gets tied up fast. An owner-clinician setup can keep more cash in the business, while a hired-provider setup needs tight volume control to cover wage load, supervision, and state licensing rules.
Track wage load per completed visit
Measure admin wages, clinical hours, completed visits, and collections per visit together. If admin pay alone is $265k and climbs to $460k, fixed payroll pressure rises even before provider pay. That means owner draw only works when visit volume and schedule fill stay high.
Set a weekly staffing plan by service type and state. Track the ratio of staffed hours to completed treatments, and flag any shift where supervision rules or idle time push labor cost up faster than collections. Volume discipline is the control point.
5
Vehicle, Insurance, Compliance, And Fixed Overhead
Fixed Overhead Hurdle
Fixed overhead is the monthly cash bill you must cover before the owner can take home pay. Here, listed recurring costs total $1,875k per month across vehicle insurance, lease or loan payments, software base fees, rent, utilities, marketing, legal and compliance, and professional liability insurance.
This is the break-even floor. If completed visits or collections slip, the same overhead stays in place, so cash gets tight fast. Use fixed overhead ÷ contribution per completed treatment to see how many visits the clinic needs each month just to stand still.
Measure The Monthly Burn
Track each fixed line separately so the owner can see what is driving the cash hurdle. The clean inputs are insurance, debt service, software, rent, utilities, marketing, legal, compliance, and professional liability. The $465k startup build only matters here if it turns into loan or lease payments.
- Track fixed cost by month.
- Separate fixed and variable spend.
- Compare overhead to collections.
- Keep reserves for delays and repairs.
Reserves are not overhead, but they protect owner income when repairs, equipment replacement, compliance work, or billing delays hit cash. If reserves are thin, even a good month can still leave the owner short on pay.
6
Compare low, base, and high mobile clinic income scenarios
Owner income scenarios
Owner income moves fast as visit volume, staffing, and overhead scale. The year 1, year 3, and year 5 cases show how that operating mix changes EBITDA.
| Scenario | Low CaseDownside case | Base CaseBase case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the lower-income path built on year 1 assumptions. | This is the modeled middle path using year 3 assumptions. | This is the stronger earnings path built on year 5 assumptions. |
| Typical setup | The clinic runs one physician, two nurse practitioners, and smaller support staff, with about $99k in monthly revenue and year 1 EBITDA near $237k. | The clinic scales to two physicians, four nurse practitioners, and higher monthly volume, with year 3 EBITDA near $1.243M. | The clinic reaches three physicians, six nurse practitioners, and the highest modeled volume, with year 5 EBITDA near $2.578M. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | About $237kIncome floor | About $1.24MCore plan | About $2.58MUpside run |
| Best fit | Use this to test a slower start or weaker utilization in the first operating year. | Use this as the main planning case for a steady expansion plan and normal utilization. | Use this to test what happens if the clinic keeps adding capacity without a big cost step-up. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or owner distributions.
Related Products
- Mobile Health Clinic Porter's Five Forces Analysis
- Mobile Health Clinic BCG Matrix
- Mobile Health Clinic Business Model Canvas
- 7 Essential Financial KPIs for Your Mobile Health Clinic
- Mobile Health Clinic Business Plan Template in Pre-Written Word
- 7 Proven Strategies to Boost Mobile Health Clinic Profit Margins
- How to Calculate Running Costs for a Mobile Health Clinic
- Mobile Health Clinic Startup Costs: Plan $580K CAPEX Plus Cash Reserve
- Mobile Health Clinic Financial Model Template in Excel
- How to Open a Mobile Health Clinic in 6 to 12 Months
- How to Write a Mobile Health Clinic Business Plan: 7 Actionable Steps
- Mobile Health Clinic Marketing Mix
- Mobile Health Clinic Marketing Plan
- Mobile Health Clinic Business Proposal
- Mobile Health Clinic PESTEL Analysis
- Mobile Health Clinic Pitch Deck Example Editable PPTX
- Mobile Health Clinic Business SWOT Analysis
- Mobile Health Clinic Value Proposition Canvas
Frequently Asked Questions
The supplied model shows $278k of Year 1 operating profit on $9036k revenue, before taxes, reserves, and any clinician pay not listed By Year 5, modeled operating profit reaches $272M on $389M revenue Actual take-home depends on payer collections, staffing, route use, debt service, and reserve policy