 Owner income$381K
Owner income$381KHow Much Mobile Mammography Owners Make: $569K Year 1 EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$381K  Net margin28%
Net margin28% Revenue for target pay$1.37M
Revenue for target pay$1.37M Business difficultyHard
Business difficultyHard


A mobile mammography business owner can show about $569K of first-year EBITDA in this researched planning case, before owner pay, personal taxes, debt service, and reserves That comes from $149M in revenue, 535 completed screenings per month, and an 86% contribution margin after listed reading fees, supplies, fuel, maintenance, commissions, and referral fees By the mature year, the model reaches $1019M in revenue and $663M in EBITDA These are planning assumptions, not guaranteed distributions or reimbursement advice
Owner income$381KNet margin28%Revenue for target pay$1.37MBusiness difficultyHardWant to test your mobile mammography owner income?
Owner income calculator
Estimate monthly owner take-home and the target-pay gap from revenue, margin, staffing, overhead, reserves, and a pay target.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, owner distribution advice, or a final reimbursement determination.
Want to see the Mobile Mammography forecast?
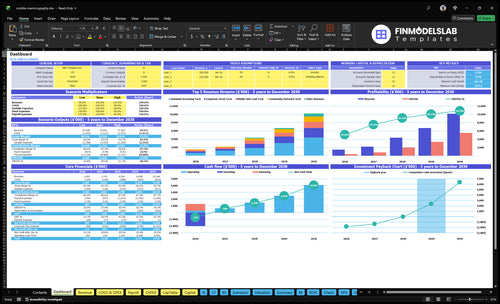
The Mobile Mammography Financial Model Template dashboard shows $149M first-year revenue, $1,019M mature-year revenue, $569K first-year EBITDA, and $663M mature-year EBITDA—open it to test scenarios.
Owner-income model highlights
- Screening, pricing, capacity tabs
- Staffing and overhead inputs
- Revenue, margin, payroll charts
- Fixed costs and break-even
- Scenario and income outputs
Is a mobile mammography business profitable with one van?
Mobile Mammography can be profitable with one van, but only if screenings consistently cover clinical labor, vehicle cost, reads, insurance, licensing, and downtime. The first-year plan shows $569K EBITDA on $149M revenue, which is only about 0.4% margin, so utilization has to stay very high. One van is the hard part: as volume rises, staffing, financing exposure, compliance work, and scheduling complexity rise too.
One van math
- $149M revenue in year one
- $569K EBITDA
- Margin is about 0.4%
- Profit depends on full schedules
What one van must cover
- Clinical labor and reads
- Vehicle cost and downtime
- Insurance and licensing
- 2 techs, 1 outreach tech, 1 event tech, 1 lead tech, 2 drivers, 1 ops manager
How much revenue can one mobile mammography van make?
One Mobile Mammography van can show about $7.458M in annual revenue if the launch plan’s 2 driver FTEs equal 2 operating units; see What Is The Most Critical Measure Of Success For Mobile Mammography? for the core success metric. That’s revenue, not owner take-home, because payroll, overhead, variable costs, debt service, reserves, and downtime still come out after sales.
Revenue math
- $14.9M total first-year revenue
- 2 driver-staffed operating units
- $7.458M revenue per unit
- 535 completed screenings per month
Owner reality
- $2,323.40 average revenue per screening
- 14% listed variable costs
- $578K payroll before owner income
- $1.356M fixed overhead before debt
What costs reduce mobile mammography owner income?
For Mobile Mammography, the biggest income cuts come from payroll, radiologist reading fees, fuel, and maintenance. See How Much Does It Cost To Open, Start, Launch Your Mobile Mammography Business? for the setup side, but on the profit line the first-year payroll is $578K, fixed overhead is $1,356K, and listed variable costs equal 14% of revenue. On $149M in revenue, each extra 1% of cost cuts EBITDA by about $149K.
Main cost drains
- Payroll: $578K in year one
- Fixed overhead: $1,356K
- Variable costs: 14% of revenue
- EBITDA hit: 1% cost = $149K
Other profit leaks
- Radiologist reads: 5% of revenue
- Fuel and maintenance: 4% of revenue
- Commissions, insurance, permits: add fixed drag
- Malpractice, licensing, software, marketing, services: stack fast
Want the six mobile mammography income drivers?
1
535/moScreening Volume
More completed screenings lift billing fastest, because every open slot that gets filled turns fixed mobile capacity into revenue.
2
$23.2KPayer Mix
Better reimbursement mix raises average monthly revenue, so the same route can produce more cash without adding visits.
3
86%Route Fill
Fewer no-shows and tighter routing protect contribution margin, which is where owner income starts to show up.
4
$578KStaffing Efficiency
Payroll is a major cost, so smoother scheduling and fewer idle hours flow straight to EBITDA and take-home pay.
5
$569KPipeline
A fuller booked pipeline keeps the calendar busy and supports the EBITDA path, before reserves and debt service.
6
$1.36MVehicle Cost
Vehicle and equipment overhead can eat profit fast, so keeping this base in line matters for break-even and cash.
Mobile Mammography Core Six Income Drivers
Completed Screening Volume
Completed Screening Volume
Completed, billable screenings drive revenue here, not scheduled visits. The first-year model assumes 535 screenings per month, with $23,234 average revenue and $19,981 contribution per screening. So when completions slip, the owner loses cash flow fast, and fixed payroll, insurance, licensing, and office overhead get spread over fewer bills.
Track completions, not bookings
Measure scheduled, completed, and billed screenings separately, then watch completions by standard, outreach, corporate event, and lead tech capacity. The model says each lost completed exam cuts monthly contribution by about $200, so the fastest fix is tighter reminders, better site partners, and filling cancelled slots with another billable exam.
- 535 monthly completions target
- $19,981 contribution per screening
- $200 loss per missed exam
1
Reimbursement And Payer Mix
Reimbursement and Payer Mix
This driver is the average cash collected per completed mammogram. In year 1, service prices run $180 to $250; in the mature model they rise to $200 to $350 with premium service active. The mix across employer, community, self-pay, grant, Medicaid, Medicare, and commercial claims decides whether each screening supports owner pay or gets eaten by fixed payroll, fleet, and insurance.
At 535 completed screenings per month, moving every exam from $180 to $250 changes monthly revenue by about $37,450. So the owner’s take-home income depends on both price and payer mix, not just volume. More commercial and employer revenue usually lifts margin; more Medicaid or Medicare can slow collections and tighten cash.
Track the mix, not just volume
Measure completed screenings by payer class every month, plus denial rate and days to collect. Split results into employer, community, self-pay, grant, Medicaid, Medicare, and commercial so you can see which sites pay fast and which ones add admin work. One clean rule: price and collections have to beat labor before owner pay grows.
- Track realized revenue per exam.
- Watch cash timing by payer.
- Test higher-paying site mixes.
- Cut denials and rebills fast.
If collections lag, a full schedule still can’t fund the draw. Keep the mix balanced so higher-paying employer and commercial days help cover lower-reimbursement public-payer days, and update forecasts whenever the payer mix shifts.
2
Route Utilization And No-Shows
Route Utilization and No-Shows
Route density is the share of a vehicle day that turns into completed, billable screenings. In this model, capacity rises from 50% to 70% in outreach, 60% to 85% in standard screening, and 70% to 90% in corporate events over the model period. More completed exams on the same route lift revenue, spread fixed vehicle and staff costs, and raise owner take-home income.
No-show rate is an editable input, so missed visits can cut cash fast even when the schedule looks full. Here’s the quick math: if a site partner or reminder workflow fills seats better, the business keeps more of each route day without adding another vehicle. That matters because empty slots still carry labor, fuel, and dispatch time.
Improve Route Fill Rate
Track booked, arrived, and completed screenings by site type. Split results for outreach, standard screening, and corporate events so you can see where utilization is weakest and where reminders work best.
Push the basics first: stronger site partners, tighter schedules, and reminder workflows. If one site type stays closer to 85% to 90% completion, route revenue improves before payroll or fleet size has to rise.
- Measure booked-to-completed by site.
- Track no-shows by reminder method.
- Prioritize high-fill partner locations.
- Delay new vehicles until routes fill.
3
Staffing Efficiency
Labor Load
Staffing is the biggest visible cost here, and owner labor is not free. The first-year model shows $578K of payroll across technologists, drivers, and operations management. If completed screenings do not rise with headcount, labor eats the margin that would otherwise become owner pay and free cash.
In the mature year, payroll reaches $217M as staffing expands to 8 standard techs, 4 outreach techs, 4 event techs, 2 premium techs, 3 lead techs, and 9 drivers. That mix protects scale and coverage, but it also lowers distributable cash if paid management grows faster than billable screenings.
Track Cost Per Screening
Measure payroll per completed screening, not just total payroll. This driver includes technologist time, driver coverage, and operations management, so the key inputs are headcount, loaded pay, and completed exams. If staffing rises before volume does, each screening must absorb more labor cost and owner income drops.
- Track hours per completed screening.
- Watch overtime and idle route time.
- Separate owner ops hours from paid labor.
- Test staffing against booked screening volume.
Use the staffing plan to protect cash, not just coverage. A paid lead or manager can help scale routes, but only if that role raises completed screenings enough to cover the added wage. If it doesn’t, the business looks bigger while the owner takes home less.
4
Vehicle, Equipment, Financing, And Maintenance
Vehicle Cost Load
When the vehicle and imaging rig sit idle, owner income drops fast. The model carries $3,000/month for fleet insurance and permits, plus fuel and maintenance at 4% of first-year revenue. Because capital cost is separate, break-even depends on how many billable screenings the vehicle can support, not just the purchase price.
In the mature year, maintenance falls to 35%, so a tighter fleet can improve cash flow. But debt service and replacement reserves are not in EBITDA, so a business can look profitable and still leave less cash for owner pay after loan bills and upkeep.
Track Cost Per Exam
Measure fleet cost per completed screening, not per vehicle day. Start with $3,000/month, then add fuel, maintenance, service contracts, downtime, and replacement reserves. Divide by completed exams to see if the rig is earning its keep. If volume stalls, this cost hits owner draws first.
- First-year revenue sets the 4% base.
- Completed screenings spread fixed fleet costs.
- Downtime days raise cost per exam.
- Loan payments cut free cash.
Test route miles, repair frequency, and idle days against the 4% fuel-and-maintenance assumption. Better uptime keeps cash inside the business; weak scheduling pushes spend up before the owner gets paid.
5
Partnership And Contract Pipeline
Contract Pipeline Quality
This driver is the share of screenings that come from repeat employers, clinics, health systems, insurers, and community sites. It matters because contracted sites lift completed screenings, not just leads. In the model, corporate event volume starts at 140 completed screenings per month and reaches 792 in the mature year; outreach starts at 75 and reaches 544. More booked sites spread fixed labor, vehicle, and admin cost over more billable exams.
The risk is simple: contracts reduce wasted marketing, but they are not guaranteed bookings. If the pipeline weakens, no-shows rise and the route sits idle, so cash collected drops before payroll and vehicle costs do. That hits owner pay fast because the same team and vehicle keep burning time while fewer visits turn into revenue.
Track Site Fill Rate
Measure each site by completed screenings, show rate, and route hours. The best contract is the one that turns a full day on the road into the most billable exams, not the one that just looks busy on paper.
- Track confirmed exams by partner.
- Rank sites by route density.
- Drop weak dates early.
Keep a 30- to 90-day pipeline with named contacts, dates, and expected counts. If a site will not fill enough slots, replace it fast so staff time, fuel, and overtime stay tied to paying volume and owner cash stays predictable.
6
Compare lean, scaled, and mature mobile mammography income cases
Owner income scenarios
Owner income moves with screening volume, staffing, and fleet overhead. Early launch is cash tight, but higher utilization and a better case mix lift earnings fast.
| Scenario | Low CaseLaunch load | Base CaseStaffing load | High CaseReserve need |
|---|---|---|---|
| Launch model | Low case assumes a Year 1 ramp with modest volume and EBITDA before owner pay, taxes, debt, and reserves. | Base case assumes a Year 3 operating rhythm with stronger volume and EBITDA before owner pay, taxes, debt, and reserves. | High case assumes a Year 5 mature run with stronger capacity use and EBITDA before owner pay, taxes, debt, and reserves. |
| Typical setup | One mobile unit, early staffing build, and a full fixed cost base make the first operating year the tightest period. | Two units, more tech FTEs, and steadier utilization support a larger revenue base, but payroll still does most of the work. | A fuller two-unit setup with premium service volume, more staff, and tighter scheduling pushes earnings higher. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | About $381kLaunch case | About $1.99MScaled case | About $5.53MMature case |
| Best fit | Use this to stress test the first-year launch and reserve need. | Use this for a steady-state plan after the first ramp period. | Use this to test upside if utilization stays high and reserves are funded. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Mobile Mammography Porter's Five Forces Analysis
- Mobile Mammography BCG Matrix
- Mobile Mammography Business Model Canvas
- 7 Critical KPIs for Mobile Mammography Operations
- Mobile Mammography Business Plan Template in Pre-Written Word
- How to Boost Mobile Mammography Profit Margins
- How to Run a Mobile Mammography Business: Monthly Costs and Cash Flow
- How Much It Costs To Start A Mobile Mammography Business: $172M
- Mobile Mammography Financial Model Template in Excel
- How To Open A Mobile Mammography Business With 5 Year 1 Techs
- How to Write a Mobile Mammography Business Plan (7 Steps)
- Mobile Mammography Marketing Mix
- Mobile Mammography Marketing Plan
- Mobile Mammography Business Proposal
- Mobile Mammography PESTEL Analysis
- Mobile Mammography Pitch Deck Example Editable PPTX
- Mobile Mammography Business SWOT Analysis
- Mobile Mammography Value Proposition Canvas
Frequently Asked Questions
In this planning case, first-year EBITDA is about $569K on $149M revenue That is before owner pay, personal taxes, debt service, and reserves The mature-year case reaches $663M EBITDA on $1019M revenue, but that assumes much higher staffing, volume, and utilization