 Time to Open8-16 weeksLaunch runway
Time to Open8-16 weeksLaunch runwayHow To Open A Neurofeedback Therapy Practice In 8–16 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open8-16 weeksLaunch runway  Launch Sequence6 stagesScope first
Launch Sequence6 stagesScope first Key BottleneckTraining gapProvider readiness
Key BottleneckTraining gapProvider readiness First Revenue StepPaid intakeAssessment ready
First Revenue StepPaid intakeAssessment ready


Key Takeaways
- Scope and credentials must be clear before booking clients.
- Equipment, software, and room setup need testing first.
- Intake, consent, and HIPAA controls reduce care risk.
- Capacity math points to $68,340 monthly revenue at modeled capacity.
Time to Open8-16 weeksLaunch runwayLaunch Sequence6 stagesScope firstKey BottleneckTraining gapProvider readinessFirst Revenue StepPaid intakeAssessment readyLaunch timeline
This web view shows the short launch timeline, and the XLSX export carries the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Scope / compliance
- Service scope defined
- Privacy workflows drafted
- Consent forms approved
- Intake forms approved
- Compliance signoff
Equipment / software
- Vendor quotes gathered
- Equipment ordered
- Software configured
- Brain map test
- Backup tools ready
Space / setup
- Space plan set
- Clinic buildout starts
- Soundproofing done
- Waiting area set
Staffing / training
- Core team hired
- Training plan built
- Session drills run
- Documentation training
- Readiness check
Marketing / referrals
- Referral list built
- Outreach materials ready
- Intro meetings book
- Launch offers sent
First-client ops
- Scheduling live
- Payments tested
- First clients booked
- Go-live review
Want to test the launch plan before signing leases?
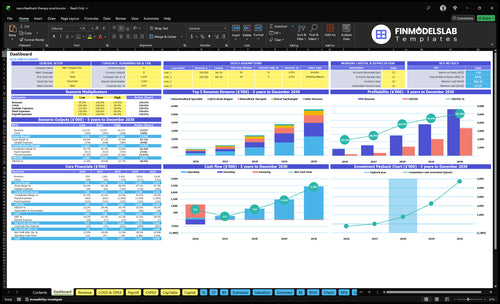
Before you sign a lease, this Neurofeedback Therapy Financial Model Template shows dashboard, launch timing, revenue ramp, staffing, runway, and breakeven—open it now.
Financial model highlights
- $68,340 monthly at capacity
- 9% variable and direct costs
- $42,307 breakeven revenue
How do you get first neurofeedback clients?
Get first clients for Neurofeedback Therapy by building trust before opening week, then turning referrals into paid intake or qEEG assessments at $350 and follow-on $160 sessions; if you’re planning launch costs too, see How Much Does It Cost To Open And Launch Your Neurofeedback Therapy Business?. Start with therapists, physicians, schools, parent groups, attention-related communities, anxiety-focused networks, performance clients, and existing wellness partners. The first real signal is not ads; it’s booked referral meetings, a clear intake script, and a clean assessment-to-plan handoff.
Trust channels first
- Meet therapists and physicians early
- Ask schools and parent groups
- Use attention and anxiety networks
- Keep promises ethical and clear
Convert the lead
- Offer consultation calls first
- Screen for clear suitability criteria
- Sell $350 intake or qEEG
- Move fit clients to $160 sessions
How long does it take to start a neurofeedback practice?
If licensure and space are already in place, a Neurofeedback Therapy practice can often open in 8–16 weeks. The usual delays are equipment procurement, software onboarding, provider training, office setup, HIPAA workflows, consent review, and referral marketing lead time. First confirm scope and protocols, then install and test equipment, then book assessments and run dry runs before the first client. New licensure, buildout, or payer contracting can push launch past that window.
Start first
- Confirm scope and protocols
- Install and test equipment
- Train the provider
- Book assessments
Common delays
- Equipment procurement takes time
- HIPAA workflows need setup
- Referral marketing has lead time
- Buildout or payer work can extend launch
Do you need a license to offer neurofeedback?
You may need a professional license to offer Neurofeedback Therapy, but the answer is state-specific across 50 U.S. states: it depends on scope of practice, supervision, diagnosis, treatment claims, and payer rules; see What Is The Main Indicator Of Success For Neurofeedback Therapy? before selling therapy-like services.
License check
- Review state scope rules
- Confirm diagnosis claim limits
- Set written supervision terms
- Check payer documentation expectations
Launch proof
- Get counsel or board confirmation
- Treat BCIA as certification, not license
- Review malpractice coverage before intake
- Use consent language before session one
Confirm what must be complete before paid neurofeedback sessions
Launch readiness checklist
Use this go-live approval checklist before opening a neurofeedback therapy clinic.
Compliance
- State scope review completeCritical
Scope must match local rules before any client is booked.
- Supervision rules documentedCritical
Supervision must be clear for every clinician before care starts.
- Malpractice policy boundCritical
Coverage needs to be active before the first session.
- HIPAA workflows testedHigh
Privacy steps must work before intake or charting.
- Informed consent approvedCritical
Consent must explain risks, limits, and expected outcomes.
Clinical flow
- Intake forms finalizedHigh
Intake data must be consistent for triage and charting.
- qEEG workflow signed offHigh
qEEG steps need to be repeatable before assessments start.
- Treatment protocols approvedCritical
Protocols keep session plans aligned across providers.
- Referral list preparedHigh
Referral partners support clients who need higher care.
Facility
- Private rooms installedCritical
Rooms need privacy before live sessions begin.
- Neurofeedback systems testedCritical
Systems must run cleanly before any paid treatment.
- Soundproofing confirmedMedium
Sound control protects session quality and client focus.
- Supplies stockedHigh
Stockouts can delay the first week.
Systems
- EHR access verifiedCritical
Clinicians need secure charting before the first visit.
- Booking and payment flow worksCritical
Booking and payment must work together to avoid lost revenue.
- Charting templates loadedHigh
Templates save time and keep notes consistent.
- Software licenses activeCritical
License gaps can stop care or billing.
Team
- Lead practitioner namedCritical
One clinical owner must be named before go-live.
- Provider training completedCritical
Staff need hands-on practice with tools and scripts.
- Coverage plan matchedHigh
Coverage should match Year 1 demand by role.
- Escalation paths clearHigh
Escalation rules reduce risk when a client worsens.
Economics
- First-year capacity checkedCritical
Year 1 should fit 50% to 70% capacity by role.
- Pricing matches modelCritical
Prices should cover $350 qEEG and $160 sessions.
- Cash runway covers setupCritical
Cash must cover the $674k minimum need in Month 5.
- Referral meetings bookedHigh
Booked referral talks are the first revenue channel.
- Go-live signoff completeCritical
Final signoff confirms compliance, systems, and client flow.
Want the six drivers that decide opening readiness?
1Clinical Scope
License gateClear scope and credentials first; it lowers referral objections and keeps bookings inside state rules.
2Equipment Setup
Setup readySystems must be installed and tested first, or onboarding slips and first assessments get canceled.
3Intake System
Intake flowA fixed intake flow keeps screening, consent, and session notes consistent and safer from day one.
4HIPAA Ops
HIPAA readySecure records and private workflows keep sensitive data safe and reduce admin failures at opening.
5Referral Flow
$350 / $160Paid qEEG at $350 and sessions at $160 need pre-open demand, or the schedule stays thin.
6Capacity Check
50-70% capModeled Year 1 capacity supports about $68K monthly revenue, but $8.5K overhead and $30K wages need close watch.
Clinical Scope And Credentials
Clinical Scope and Credentials
No scope, no launch. Neurofeedback is a clinical service, so the first gate is making sure each provider’s license, supervision, and allowed tasks match state law before the first client books. BCIA certification can support credibility and training, but it does not replace legal scope or let a provider offer services their license does not allow.
If the team books clients before scope is clear, the clinic can run into referral objections, consent edits, and day-one delays. The risk is simple: a provider may look qualified, but still be unable to deliver the exact service claimed, which raises compliance exposure and can stall opening from the start.
Verify scope before the schedule opens
Lock the rules first. Do a written compliance review, then line up malpractice coverage, role definitions, referral language, consent forms, and documentation standards so they all match the same scope. That keeps the launch clean and avoids rework after intake starts.
Check these inputs before opening week:
- License and supervision rules
- Allowed service claims
- Malpractice coverage terms
- Consent language and chart templates
- Referral-out wording for edge cases
1
Equipment And Software Readiness
Equipment And Software Ready
This is a go/no-go item. Do not open the schedule until equipment setup, software onboarding, qEEG workflow testing, and room calibration are complete. If systems are paid for but still onboarding, you can lose launch weeks and still carry fixed costs, which pushes the first assessment date back.
The main dependency is provider training plus secure documentation. If the team cannot run a full session, save records, and use the backup process without help, day-one care slows down. That usually shows up as canceled first assessments, longer visits, and a rough first client experience.
Test Before Booking
Lock the order: vendor selection, ordering, installation, training, then live testing. Readiness means the workflow works without help. Here’s the quick math: $8,500 fixed overhead plus $30,000 listed wages equals $38,500 a month before any treatment revenue, so a launch slip gets expensive fast.
- Run one full client session.
- Test qEEG notes and storage.
- Calibrate each treatment room.
- Print backup steps and contacts.
- Practice provider handoffs twice.
Do not book paid assessments until the team can repeat the process cleanly. If setup slips, delay the calendar and finish the last checks first. That protects day-one capacity and keeps the clinic from paying for idle systems while clients wait.
2
Protocol And Intake System
Intake and Care Protocol
This is the gate that keeps the clinic from opening with guesswork. Screening, suitability, assessment, goals, treatment planning, session notes, progress reviews, and referral-out rules need to be set before the first booking. If the team starts without a clear intake path, providers will make different calls on who is a fit, what gets documented, and when to stop or refer out.
Informed consent has to be in plain English. It should explain limits, risks, expectations, privacy, and alternatives so clients know what neurofeedback can and cannot do. That lowers day-one confusion, supports safer operations, and keeps the first client experience consistent across providers.
Build the Intake Packet First
Lock the full workflow before opening: one intake form set, one qEEG rule set, one session note template, and one review cadence. qEEG means a brainwave mapping step used to guide fit and planning. Put referral-out triggers in writing so staff know when a client needs a different provider or a different level of care.
- Screen before scheduling treatment.
- Test consent language with staff.
- Use one note template.
- Review progress on schedule.
- Document handoffs every time.
Run the whole path before launch day: screen, consent, assess, plan, document, review, and hand off. If staff have to debate client fit or rewrite notes in week one, you slow openings, weaken handoffs, and create uneven care delivery. One clean workflow now is cheaper than fixing intake mistakes after clients are already on the schedule.
3
HIPAA-Ready Clinic Operations
HIPAA-Ready Clinic Ops
This gate decides whether the clinic can open cleanly and serve clients on day one. Before the schedule opens, private rooms, secure records, scheduling, payments, and client messaging all need to work under HIPAA, the federal Health Insurance Portability and Accountability Act privacy and security rules for protected health information. If intake data is collected before access controls are set, launch slips and the first visit feels messy.
The operating stack includes the electronic health record, user permissions, payment flow, cancellation policy, incident process, insurance handling, and staff scripts. Clean setup cuts admin errors and protects the first client experience. Weak setup can force manual work, expose sensitive data, and delay opening week while policies and systems get fixed.
Lock the workflow before booking
Build and test the full path before the calendar opens: intake form, record storage, client messages, payment collection, and cancellation rules. Assign who can see what, who answers issues, and what the incident process looks like. If any step is still manual, document it and test it in a mock visit first.
- Set EHR access controls.
- Test payment and refund steps.
- Approve privacy and cancellation scripts.
- Train staff on incident reporting.
4
Referral And Client Acquisition
Referral Pipeline Before Open
Referral marketing has to start before the clinic opens, or you can end up with a finished clinic and empty assessment slots. The referral list here spans 8 groups: therapists, physicians, schools, parents, attention-related communities, anxiety-focused networks, performance clients, and wellness partners.
Use education, not hype. A referral one-pager, consultation calls, intake criteria, and a follow-up process help turn trust into the first paid qEEG assessments on day one, without unsupported medical claims.
Set the referral machine before opening
Build outreach while the clinic is still being finished. Keep the message tight: who you serve, what a first visit looks like, and when a referral should be sent.
- Lead with ethical education sessions.
- Use one referral one-pager.
- Define intake fit and referral-out rules.
- Assign follow-up within 24 to 48 hours.
- Track first qEEG inquiries by source.
5
Capacity And Financial-Model Validation
Capacity Check
This launch driver decides whether the clinic can open with enough booked volume to pay its bills from day one. The Year 1 model assumes 2 neurofeedback specialists at 120 monthly treatments each and 65% capacity, plus 1 qEEG mapper at 80 monthly assessments and 70% capacity, with biofeedback, psychology, and lead practitioner time at 50% to 60%. That mix points to about $68,340 in monthly revenue at modeled capacity.
The risk is simple: if bookings trail the model, fixed costs still hit on schedule. Year 1 direct and variable costs total 9%, fixed overhead is $8,500 a month, and listed wages are $30,000. The breakeven planning check is about $42,307 in monthly revenue before unlisted costs, so a slow ramp can turn into cash pressure fast.
Test the Ramp
Before opening, build the schedule from real weekly capacity, not best-case utilization. Lock the first 8 to 12 weeks of staffing, room time, software access, and intake flow, then compare that plan with likely bookings. If the clinic cannot reach modeled load quickly, trim hours or delay hiring; otherwise payroll can outpace revenue in the first month.
- Confirm booked hours by role.
- Test qEEG and session flow.
- Track no-shows and rebook speed.
- Set a cash buffer for slow weeks.
- Verify backup coverage for absences.
6
Related Products
- Neurofeedback Therapy Porter's Five Forces Analysis
- Neurofeedback Therapy BCG Matrix
- Neurofeedback Therapy Business Model Canvas
- 7 Critical KPIs for Neurofeedback Therapy Clinics
- Neurofeedback Therapy Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Neurofeedback Therapy Profitability
- Running Costs for Neurofeedback Therapy: A Monthly Financial Breakdown
- Neurofeedback Therapy Startup Costs: $360K+ Before Launch
- Neurofeedback Therapy Financial Model Template in Excel
- How Much Does a Neurofeedback Therapy Practice Owner Make? $284k Model
- How to Write a Business Plan for Neurofeedback Therapy
- Neurofeedback Therapy Marketing Mix
- Neurofeedback Therapy Marketing Plan
- Neurofeedback Therapy Business Proposal
- Neurofeedback Therapy PESTEL Analysis
- Neurofeedback Therapy Pitch Deck Example Editable PPTX
- Neurofeedback Therapy Business SWOT Analysis
- Neurofeedback Therapy Value Proposition Canvas
Frequently Asked Questions
Start by confirming state scope of practice, supervision rules, and provider credentials Then set up equipment, HIPAA-ready records, consent forms, scheduling, and referral channels A practical launch often takes 8–16 weeks if space and licensure are ready In the model, Year 1 planning uses $350 qEEG assessments, $160 neurofeedback sessions, and 50% to 70% role capacity