 Time to Open7 monthsLaunch runway
Time to Open7 monthsLaunch runwayHow To Open A Neurological Rehabilitation Center In 6 To 12 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open7 monthsLaunch runway  Launch Sequence8 stagesCompliance first
Launch Sequence8 stagesCompliance first Key BottleneckStaffing gapPayer setup
Key BottleneckStaffing gapPayer setup First Revenue StepInitial evalsReferral sources
First Revenue StepInitial evalsReferral sources


Key Takeaways
- Start with a narrow service menu and licensed coverage.
- Document compliance before opening to avoid payer delays.
- Match rooms and equipment to the first services.
- Build referral contacts before launch to fill schedules.
Time to Open7 monthsLaunch runwayLaunch Sequence8 stagesCompliance firstKey BottleneckStaffing gapPayer setupFirst Revenue StepInitial evalsReferral sourcesLaunch timeline
Short web summary of the launch plan; the XLSX export contains the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11
Compliance & licensing
- Scope service model
- Draft policies
- Submit licenses
- Site compliance review
Facility & equipment
- Finalize floor plan
- Order treatment tables
- Install IT systems
- Receive rehab devices
Staffing & training
- Recruit therapists
- Hire core team
- Train care pathways
- Run mock sessions
Payer credentialing
- Build payer list
- Submit credentialing forms
- Follow up approvals
- Activate billing setup
Referral marketing
- Map referral sources
- Meet physicians
- Launch patient outreach
- Open intake funnel
Opening operations
- Set staffing roster
- Build launch budget
- Test scheduling flow
- Opening week support
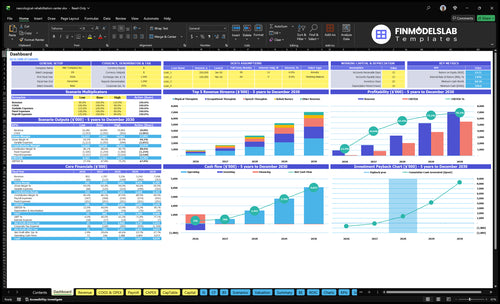
Why test the Neurological Rehabilitation model before opening?
Open the Neurological Rehabilitation Financial Model Template; the dashboard and assumptions tabs show revenue, costs, cash needs, launch timing, payer mix, patient ramp, cash runway, and break-even. Year 1 staffing is 3 physical therapists, 2 occupational therapists, 1 speech therapist, 1 neuropsychologist, and 1 rehab nurse, with monthly revenue near $70,980; verify reimbursement and payer timing.
Financial model highlights
- Revenue ramp chart
- Staffing load chart
- Capacity and runway
- Verify payer timing
What do you need to open a neurological rehabilitation center?
To open a Neurological Rehabilitation center, choose an outpatient or facility-based model, define a billable therapy scope, hire licensed clinicians, and set up compliant space, documentation, EMR, billing, insurance, and referral channels; for success tracking, start with What Is The Most Critical Metric To Measure The Success Of Neurological Rehabilitation?. The readiness signal is simple: a staffed, documented, billable, referable clinic that can deliver 9 core service areas.
Core setup
- Choose outpatient or facility-based care
- Define 9 therapy service lines
- Hire licensed PT, OT, and speech clinicians
- Prepare treatment rooms and therapy equipment
Compliance stack
- Verify state healthcare rules
- Meet payer documentation requirements
- Check professional licensing board rules
- Set up EMR, billing, and insurance
How long does it take to open a neurological rehabilitation center?
For Neurological Rehabilitation, a practical opening window is 6 to 12 months, and the pace depends on lease, buildout, equipment delivery, therapist hiring, state requirements, Medicare or commercial payer credentialing, EMR setup, and referral pipeline work. Don’t wait for construction to finish; start credentialing, hiring, vendor setup, and physician outreach early so your first evaluations can begin as soon as payers are ready.
Main timing drivers
- Lease can set the pace
- Buildout often takes months
- Equipment delivery can slip timing
- Licensed therapists are hard to hire
Protect first revenue
- Start credentialing before construction ends
- Set up EMR early
- Line up referrals with physicians
- Open with initial evaluations first
How do you get patients for a neurological rehabilitation center?
Patients usually come from a referral network, not generic ads, so start building it before opening. For What Is The Estimated Cost To Open And Launch Your Neurological Rehabilitation Business?, the first-patient path should be simple: referral intake, benefits check, evaluation scheduling, care plan, and follow-up reporting.
Start with referrers
- Neurologists send the right cases.
- Hospitals need fast discharge options.
- Discharge planners control next steps.
- Primary care physicians need clear handoffs.
Make referral easy
- Share service scope and access steps.
- Show payer readiness and documentation rules.
- Report outcomes back after each evaluation.
- Include orthopedic, spine, and case managers.
Also work workers’ compensation contacts, senior care networks, and stroke or brain injury support groups, because they see patients early and can steer them fast. With 3 therapy types—physical, occupational, and speech—you need every referrer to know exactly what happens next.
First visit flow
- Intake the referral the same day.
- Verify benefits before the visit.
- Schedule the evaluation quickly.
- Send the care plan and updates.
What builds trust
- Use plain, timely communication.
- Keep documentation standards tight.
- Lead with outcomes, not ads.
- Answer payer questions before launch.
Confirm what must be ready before a neuro rehab clinic accepts patients
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Registration
- Entity registration completeCritical
The clinic needs a legal entity before permits, contracts, and payer setup.
- State clinic permit approvedCritical
State healthcare approval can block opening if it's missing.
- Scope rules reviewedHigh
Each role must stay within state scope before patient care starts.
Credentialing
- Therapist licenses verifiedCritical
Physical, occupational, speech, neuropsychology, and nursing licenses must be current.
- Malpractice coverage boundCritical
Coverage should be live before any patient session.
- Clinical director assignedHigh
One accountable clinician must own care quality and escalation.
Facility
- Treatment rooms readyHigh
Rooms must support therapy work without day-one bottlenecks.
- Accessibility path clearedCritical
Patients need safe access for mobility limits and equipment.
- Emergency procedures postedCritical
Staff need clear steps for falls, seizures, and urgent events.
Systems
- Electronic records configuredCritical
Records must support notes, plans, and audit trails from day one.
- Consent forms approvedCritical
Consent must be ready before the first evaluation or treatment.
- Incident workflow testedHigh
Reporting steps should work when a patient event happens.
- Billing setup testedHigh
Clean claims help cash flow start on time.
Staffing
- Opening roster filledCritical
The clinic needs enough coverage for the opening-week load.
- Orientation completedHigh
Staff must know documentation, handoff, and escalation rules.
- Year one capacity setMedium
Plan around 50% to 60% early capacity across clinical lines.
Launch plan
- Referral outreach activeHigh
Inbound referrals must start before the first patient day.
- Opening-week schedule builtHigh
The first week needs balanced visits, evals, and admin time.
- Cash runway confirmedCritical
Minimum cash of $330k is needed at Month 7.
- Go-live signoff issuedCritical
Final signoff should confirm care, systems, staffing, and cash.
Want to check the six launch drivers before opening?
1Service Scope
Start narrowA narrower service menu keeps hiring, documentation, and equipment aligned at opening.
2Licensing Readiness
Compliance gateDocumented policies and trained staff keep licensing, HIPAA, and payer acceptance on track.
3Facility Setup
Soft-open readyMatching rooms and equipment to the service menu speeds soft opening and avoids trapped cash.
4Therapist Staffing
8 cliniciansEight Year 1 clinicians set day-one capacity and protect referral credibility.
5Billing Setup
Payer readyPayer-ready workflows cut denials and reduce cash strain during the first ramp-up.
6Referral Pipeline
Pre-open leadsNamed referral contacts speed evaluations before opening month and fill the first schedule.
Clinical Service Scope
Clinical Scope First
Your service menu decides whether you can open on time. If you start with too many services, every one needs licensed staff, space, equipment, documentation, payer setup, and a clear referral message before day one.
A narrower scope is safer. If PT, OT, and speech therapy are ready, but cognitive rehab or gait training is not, launch the ready services first and add the rest after volume proves the need.
Scope Check Before Open
Build a line-by-line readiness list for each service: staff license, room, equipment, note template, billing code setup, and referral language. If one item is missing, that service is not launch-ready.
Use the staffing plan as the gate. The Year 1 mix of 3 physical therapists, 2 occupational therapists, 1 speech therapist, 1 neuropsychologist, and 1 rehab nurse should match the scope you can actually support on day one.
- Start with the services you can staff.
- Match equipment to the menu.
- Set payer setup before scheduling.
- Keep referral promises tight.
1
Licensing And Compliance Readiness
Licensing & Compliance Readiness
Compliance decides whether a neurological rehab center can open on time and accept patients on day one. Before the first evaluation, verify state healthcare rules, therapist licensure, business insurance, HIPAA compliance, patient consent, documentation standards, incident procedures, and any Medicare or payer participation rules. If one approval is missing, the center can’t safely or legally start care.
The readiness signal is simple: written policies, trained staff, and proof the facility meets safety and privacy rules. HIPAA means protecting patient health information. In rehab, weak documentation or a broken consent flow can delay billing, trigger rework, and slow first cash from treatment visits.
Verify Before You Schedule
Start with state licensure boards, payers, and the facility checklist, then lock down insurance, forms, and incident procedures before booking patients. One clean rule: no patient should be scheduled until the center can legally document, bill, and protect records.
- Confirm each clinician license status
- Test consent and intake forms
- Train staff on HIPAA and incidents
- Check payer participation and billing rules
- Document safety steps before inspections
If any payer or license item is missing, launch shifts from operations to compliance cleanup, and that can push first revenue back. Keep one file with approvals, policies, and contact names so the team can answer inspectors, payers, and referral partners fast.
2
Facility And Equipment Setup
Facility and Equipment Setup
A neurological rehab center opens on time only when the rooms, therapy gym, accessibility, EMR workstations, and storage match the first service menu. The goal is a safe path from intake to treatment to checkout; if that path is broken, day-one care slows and the soft opening gets messy.
Plan for the items you will actually use at launch: balance and gait equipment, mats, parallel bars, assessment tools, assistive devices, and infection-control supplies. Buying advanced gear before demand is proven can trap cash and crowd the floor, while missing basics can delay patient starts.
Map the room flow first
Map each step before ordering gear: check-in, evaluation, treatment, charting, and discharge. Confirm the space supports accessibility and staff movement, then test the layout with one real patient path so you can catch bottlenecks before opening. If the flow works, the soft opening is smoother and the team can serve patients from day one.
3
Therapist Staffing Plan
Therapist Staffing Plan
Open on time only if the core team is hired, licensed, and trained before the first referral lands. This year-one plan calls for 3 physical therapists, 2 occupational therapists, 1 speech therapist, 1 neuropsychologist, and 1 rehab nurse, so staffing is the main capacity gate on day one.
The real readiness signal is licensed coverage, neuro experience, documentation standards, and coverage scheduling. If those are weak, the clinic may open with a full payroll but less real treatment capacity, which raises cash pressure before referrals build. One missed role can slow evaluations, delay care plans, and weaken referral trust.
Staff Before You Scale Visits
Start with the staffing map, then layer in support roles: clinical director, rehabilitation aides, intake coordinator, billing support, and part-time specialists only as scope requires. Confirm every clinician is licensed for the state, can document to standard, and has coverage blocks that match patient demand.
- Verify active licenses before scheduling
- Test coverage for therapy and neuro visits
- Train documentation before first patient
- Hold part-time roles until demand proves out
Here’s the quick risk check: if the schedule is built around hiring dates instead of patient flow, payroll starts before referrals do. That can still be a valid launch plan, but only if cash is set aside for a controlled ramp-up and the intake team can fill the calendar fast.
4
Payer Credentialing And Billing Setup
Payer Readiness
Payer credentialing and billing setup decides whether Ascend NeuroCare can get paid from day one. For a neurological rehab clinic, that means Medicare, Medicaid where relevant, commercial payer contracts, prior authorization, coding, documentation, claim submission, and denial workflows must be ready before the first patient is booked.
The readiness signal is simple: evaluations can be scheduled, verified, documented, billed, and followed up. The bottleneck is opening the doors before contracts or billing rules are live, which can turn early visits into delayed cash, denied claims, and avoidable write-offs.
Set Billing Before You Book
Build the payer matrix first: who you will accept, what needs prior auth, which codes apply, and what documentation each payer wants. Then test the full path with a sample visit so intake, clinical notes, charge capture, claim submission, and denial follow-up all work together.
- Confirm payer contracts and enrollment status.
- Map prior auth rules by service.
- Standardize coding and note templates.
- Train staff on claim holds and denials.
If this setup is weak, launch revenue slips even when demand is there, and cash strain shows up fast during the early ramp-up.
5
Referral Pipeline Development
Referral Pipeline
Referral pipeline is what turns clinical readiness into first patients. For a neurological rehab center, it should be built before opening with neurologists, hospitals, discharge planners, primary care offices, case managers, senior living communities, spine practices, and stroke or brain injury support groups. Waiting until opening month to sell is the bottleneck that can leave chairs empty.
Readiness means you already have named referral contacts, a clear intake workflow, payer access notes, and a simple follow-up report. That setup helps move stroke, TBI, spinal cord injury, and other neurological patients into evaluations faster, so day one is not a cold start.
Build Referrals Before Open
Start outreach while the clinic is still getting ready. A practical launch list is 7 source types: neurologists, hospitals, discharge planners, primary care offices, case managers, senior living communities, and spine practices. Add support organizations for stroke and brain injury.
- Track named contacts and direct lines.
- Document intake steps and payer notes.
- Set a weekly follow-up cadence.
- Test the handoff from referral to evaluation.
If the intake path is slow or unclear, the first revenue cycle slows too, and clinical staff may open with too few patients to use their time well.
6
Related Products
- Neurological Rehabilitation Porter's Five Forces Analysis
- Neurological Rehabilitation BCG Matrix
- Neurological Rehabilitation Business Model Canvas
- 7 Essential Financial KPIs for Neurological Rehabilitation
- Neurological Rehabilitation Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Neurological Rehabilitation Profitability
- Running Costs for Neurological Rehabilitation: A CFO's Monthly Guide
- Neurological Rehabilitation Startup Costs: $827K–$969K Opening Plan
- Neurological Rehabilitation Financial Model Template in Excel
- Neurological Rehabilitation Owner Income: $156K Before Reserves
- How to Write a Neurological Rehabilitation Business Plan
- Neurological Rehabilitation Marketing Mix
- Neurological Rehabilitation Marketing Plan
- Neurological Rehabilitation Business Proposal
- Neurological Rehabilitation PESTEL Analysis
- Neurological Rehabilitation Pitch Deck Example Editable PPTX
- Neurological Rehabilitation Business SWOT Analysis
- Neurological Rehabilitation Value Proposition Canvas
Frequently Asked Questions
Start by choosing the clinical scope and matching it to licensed staff, space, equipment, payer setup, and referral sources The researched Year 1 model assumes 3 physical therapists, 2 occupational therapists, 1 speech therapist, 1 neuropsychologist, and 1 rehab nurse At stated capacity, modeled monthly revenue is about $70,980 before fixed overhead