 Time to Open8-16 weeksOpening prep
Time to Open8-16 weeksOpening prepHow to Start a Neuromuscular Training Program in 8 to 16 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open8-16 weeksOpening prep  Launch Sequence8 stagesProtocols first
Launch Sequence8 stagesProtocols first Key BottleneckReferral gateCredentialing path
Key BottleneckReferral gateCredentialing path First Revenue StepPaid evalIntake live
First Revenue StepPaid evalIntake live


You’re launching a PT-led service line, so the first job is readiness: licensure, protocols, staff training, space, billing, and referrals This roadmap covers the 8 to 16 week launch path and uses planning assumptions like 8 Year 1 clinical providers, 686 monthly treatments, and a $110k monthly revenue run-rate at modeled utilization Costs, funding, and owner income are validation topics inside the assumptions, not the main promise here
Time to Open8-16 weeksOpening prepLaunch Sequence8 stagesProtocols firstKey BottleneckReferral gateCredentialing pathFirst Revenue StepPaid evalIntake liveLaunch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt Chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Compliance
- Scope review
- Policy draft
- Privacy setup
- Intake consent
Clinical Protocols
- Outcome measures
- Exercise scripts
- Progression rules
- Safety screen
Facility Setup
- Lease setup
- Room buildout
- Equipment install
- Tech testing
Staffing & Training
- Hire clinicians
- Onboard assistants
- Protocol drills
- Scheduling training
Billing & Referrals
- Payer enrollments
- Fee schedule
- Referral outreach
- Claims test
Marketing & Launch
- Website launch
- Outreach campaign
- Booking opens
- Soft launch
- Launch review
Want to test the launch plan before opening?
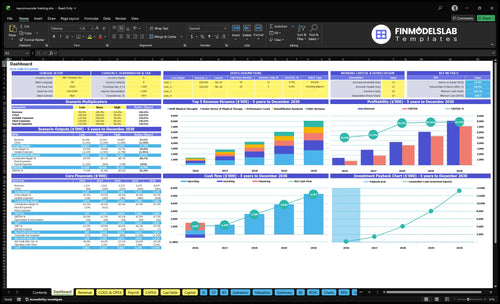
This screenshot shows revenue, costs, cash needs, assumptions, and break-even logic. Open the Neuromuscular Training Program Financial Model Template to test it.
Financial model highlights
- 8 clinical providers Year 1
- 686 monthly treatments
- $110,360 monthly revenue
- 185% variable and COGS
- $20,500 fixed overhead
- $15,833 admin payroll
- Runway and break-even checks
How do I get first patients for neuromuscular training?
For a Neuromuscular Training Program, first patients should come from clinically appropriate referrals and direct-access options where allowed; see How Increase Neuromuscular Training Program Profitability?. Focus on physician referrals, orthopedic groups, sports medicine, post-injury patients, fall-risk adults, athletes, and movement assessment offers. The first revenue step is booked initial evaluations or paid movement assessments, and Year 1 should set aside 8% of revenue for digital marketing and referral rewards.
Referral sources
- Target physician referrals first
- Build orthopedic group ties
- Use sports medicine partners
- Offer clear patient profiles
First paid step
- Book initial evaluations
- Sell movement assessments
- Track outcomes clearly
- Check follow-up conversion
What do I need to start a neuromuscular training program?
To start a Neuromuscular Training Program, you need licensed physical therapy operations, documented assessment protocols, compliant billing, and an 8-person launch team. Track capacity and utilization early with What Are The 5 KPI Metrics For Neuromuscular Training Program Business? because first revenue comes from evaluations and care plans, then fee-for-service treatment sessions.
Legal and admin
- Confirm PT licensure and scope rules
- Set supervision rules by staff role
- Carry liability coverage before intake
- Prepare consent forms and compliant claims
Clinic launch
- Build EHR templates for documentation
- Assess motor control, balance, gait
- Add resistance tools and movement space
- Staff: 2 DPTs, 2 PTs, 4 support roles
What launch mistakes should a neuromuscular training program avoid?
The biggest launch mistakes for a Neuromuscular Training Program are readiness gaps: vague positioning, weak referral flow, undertrained staff, and billing confusion. Open too early, and the Year 1 target of 686 monthly treatments gets hard to hit, while denial and churn risk climb. Fix the basics first: standardize evaluation templates, treatment pathways, safety screens, and follow-up cadence.
Launch risks
- Skip vague program positioning.
- Do not open without referrals.
- Avoid undertrained staff at launch.
- Do not mix billing workflows.
Launch fixes
- Standardize evaluation templates.
- Build clear treatment pathways.
- Use safety screens every time.
- Set follow-up cadence before opening.
Confirm what must be ready before accepting patients
Launch readiness checklist
Use this go-live approval checklist before opening to confirm the clinic is ready for patients, billing, and daily operations.
Compliance
- State licensure verifiedCritical
No patient care should start until each clinician can practice in the launch state.
- Scope of practice setCritical
This keeps therapists, coaches, and assistants inside allowed duties from day one.
- Liability policy boundCritical
Professional liability coverage should be active before any evaluation or treatment.
Protocols
- Consent forms approvedHigh
Patients need clear consent before testing, treatment, and sensor-based tracking start.
- Evaluation templates readyHigh
Standard eval forms keep visits consistent and make outcomes easier to compare.
- Safety screens definedCritical
A clear screen helps staff catch red flags before movement work begins.
- Outcome measures selectedMedium
Tracked outcomes prove whether the program improves coordination and movement patterns.
Facility
- Treatment space finishedCritical
The clinic needs safe room flow, privacy, and enough space for guided movement.
- Motion systems installedHigh
The 3D motion capture, force plates, and EMG gear must work before first visits.
- Biofeedback gear testedHigh
Biofeedback must read cleanly so therapists can coach movement with confidence.
Staffing
- Therapist mix staffedCritical
Year 1 needs 2 senior therapists, 2 staff therapists, 1 specialist, 1 coach, and 2 assistants.
- Role coverage assignedHigh
Every patient touchpoint needs a clear owner so handoffs do not break care.
- Protocol training completedHigh
Staff must know evaluation, treatment flow, and escalation steps before launch.
Intake
- Referral sources activeHigh
The clinic needs a live source of patients before the first operating month.
- Scheduling rules setHigh
Rules for visit length, capacity, and no-shows protect the 686 monthly treatment plan.
- Billing workflow testedCritical
Claims, card payments, and patient balances must clear before revenue can count.
- EHR workflows loadedHigh
The EHR should match intake, notes, billing, and patient follow-up steps.
Cash
- Revenue model stress-testedCritical
Test the 686 monthly treatments and $110,360 modeled monthly revenue before opening.
- Cost load acceptedCritical
Year 1 variable and COGS load is 185%, so margin pressure needs a clear plan.
- Overhead and payroll coveredCritical
$20,500 fixed overhead and $15,833 admin payroll must be covered before clinician pay.
- Go-live signoff completedCritical
Do not open until compliance, staffing, billing, and cash checks are all green.
Which launch drivers matter most before go-live?
1Clinical Protocol
Day 1Aligned intake, screening, and discharge steps keep evaluations consistent and reduce day-one safety and documentation misses.
2Licensed Staffing
8 staffYear 1 team of 8 supports 686 monthly treatments if licensure and competencies are in place.
3Referral Network
Pre-launchReferral scripts and intake paths must be live before opening to avoid a slow first-patient ramp.
4Facility Setup
$20.5K/moOpen floor space and core tools are enough; missing basics delay safe movement work and patient flow.
5Billing Workflow
3%+3%EHR templates, coding, and payment rules must work before visits or claims and cash collection slip.
6Patient Ramp
8% revMarketing should convert into booked evaluations first, so early volume grows without breaking operations.
Clinical Protocol Readiness
Clinical Protocol Readiness
This business opens on time only if every clinician can run the same intake, movement screen, balance and gait assessment, care plan, and discharge criteria. That protocol set is the credibility base; without it, you risk inconsistent safety screens, uneven treatment plans, and weak referral trust on day one.
The bottleneck is usually not the therapy itself, but the setup around it: EHR templates, consent forms, staff training, and referral partner education. If those pieces are missing, the clinic can still open the doors, but it won’t operate as one system, and documentation gaps can slow billing, delay follow-up, and raise compliance risk.
Standardize the first visit
Before launch, test one standard path end to end: intake, movement screen, balance and gait assessment, care plan, and discharge rules. Make sure each clinician documents the same way in the EHR, uses the same consent language, and applies the same patient-fit criteria. That is what keeps the first patient from becoming a process exception.
Use a short referral script and a clear fit/no-fit guide so outside partners know who should come in. A launch slip here is expensive: fixed overhead in the plan is $20,500 per month, so every week of delay keeps about $4,800 of fixed cost in play while day-one operations stay messy. The goal is simple: one protocol, one charting standard, one opening sequence.
- Train every clinician on the same intake.
- Standardize safety screens and progressions.
- Document discharge criteria in advance.
- Test EHR templates before first visit.
- Brief referral partners on patient fit.
1
Licensed Staffing and Competencies
Licensed Staff and Safe Capacity
Opening hinges on having the right licensed team on payroll and schedulable on day one. The Year 1 model uses 2 Senior Doctors of Physical Therapy, 2 Staff Physical Therapists, 1 Neuromuscular Specialist, 1 Performance Coach, and 2 Rehabilitation Assistants. At modeled utilization, that supports 686 treatments per month, so staffing is not just a hiring issue; it sets how many patients can be booked safely.
The readiness signal is documented competency in motor control, balance, gait, coordination, injury risk, and functional movement. If licensure, supervision, scheduling, or continuing education lag, the clinic can open late or take on too much before staff can handle complex cases safely. That creates compliance risk, weaker patient experience, and early bottlenecks in the schedule.
Lock Competency Before You Open
Before launch, verify each clinician’s license, supervision chain, and schedule coverage. Then document who can assess, who can progress care, and who can handle higher-complexity cases. Here’s the quick math: 686 monthly treatments only works if the team can safely support that volume, not just fill slots.
- Confirm every license and supervision rule.
- Document movement-screen competency.
- Train staff on continuity and handoffs.
- Test scheduling against complex-case demand.
The biggest risk is booking faster than the team can safely treat. If demand rises before staff training is done, the clinic may need to slow intake, push evals, or delay case starts. That protects safety and keeps day-one operations realistic instead of overpromising capacity.
2
Referral Network Activation
Referral Network Activation
If physicians, orthopedics, sports medicine, post-injury channels, fall-risk groups, and athlete networks don’t know who to send and when to send them, you can open with trained staff and still have no patient flow. The launch risk is not clinical skill; it’s slow referrals, which delays first evaluations and pushes back day-one revenue.
Here’s the quick math on readiness: the partner must understand what the evaluation includes, what outcomes are tracked, and the exact intake path. A short referral script plus a feedback loop is the signal that the network is live, not just “planned,” so the ramp is steadier from the first month.
Build the referral script first
Before launch month, give each target partner a one-page script that says who is a fit, when to refer, and what happens after referral. Keep it simple enough for front-desk staff and clinicians to use on the spot. If the intake path is unclear, referrals stall even when demand is real.
Verify three things before opening: a named contact for referrals, a same-week scheduling path, and a feedback note after evaluation. That loop helps partners trust the process and makes it easier to book first visits fast, instead of opening with a trained team and an empty schedule.
- Define the patient fit.
- Share a short referral script.
- Document the intake steps.
- Confirm feedback goes back.
3
Facility and Equipment Setup
Safe Treatment Space Setup
For this neuromuscular PT clinic, the room layout is a launch gate, not décor. Day one needs open floor space, balance tools, resistance equipment, a gait and movement assessment area, a documentation station, and smooth patient flow so therapists can test, treat, and chart without crowding the session.
The planning case carries $20,500 in monthly fixed overhead: $12,500 lease, $1,200 utilities and internet, $2,500 liability insurance, $800 EHR, $1,500 maintenance, and $2,000 continuing education. Unsafe layout or missing basics is the main bottleneck because it can delay opening and slow first-day care.
Check Flow Before Move-In
Map the patient path before you buy extra gear. Confirm where intake, movement screening, treatment, charting, and checkout happen, then test the setup with a full visit flow. What this estimate hides is any rework from a cramped room plan, and that can push back opening fast.
- Verify clear floor space first.
- Place charting near treatment zones.
- Store tools within reach.
- Test one full patient visit.
4
Billing and Documentation Workflow
Billing and Documentation Ready
Billing and documentation must be live before the first visit. For a neuromuscular PT program, that means the note template, coding guidance, payer rules, consent forms, cash-pay policy, payment collection process, and denial follow-up are all set. If patients arrive before those pieces work, the clinic can deliver care but still miss clean payment and compliance on day one.
This is also a cash need issue. Year 1 assumes 3% payment processing, 3% diagnostic technology licensing, and 45% clinical supplies and biofeedback sensors. So the opening budget has to cover front-end workflow setup, not just treatment space and staff.
Set the claim path first
Lock the billing rules before scheduling opens. Verify insurer credentialing status, define which visits are insurance or cash-pay, and test how each visit gets documented, coded, collected, and followed up. Insurance and cash-pay paths are launch dependencies, not a back-office afterthought.
Use a short readiness check: EHR templates, coding guidance, payer rules, and denial follow-up. If any one of those is missing, the clinic risks treating patients before the record supports payment and compliance. That can slow first revenue and create cleanup work the team cannot afford in week one.
- EHR templates ready
- Credentialing status confirmed
- Consent forms signed
- Payment collection tested
5
Patient Acquisition and First Evaluation Ramp
Evaluation Booking Ramp
Booked initial evaluations or paid movement assessments are the first revenue step, so this clinic needs a clear offer, referral intake path, and open schedule before launch. If marketing starts before staff, protocols, billing, and follow-up are ready, leads turn into missed calls, weak conversion, and launch delays.
Year 1 marketing and referral rewards are modeled at 8% of revenue. Keep early volume controlled so the team can convert evaluations into treatment plans, document cleanly, and support day-one operations without overloading the schedule.
Book Evaluations First
Set the assessment offer, referral script, and scheduling rules before any promotion goes live. Test intake, reminders, follow-up cadence, and the handoff from evaluation to treatment plan in the EHR so the first patient flow works on day one.
- Confirm call coverage before launch.
- Test no-show follow-up timing.
- Track evaluation-to-plan conversion.
- Hold spend until workflow works.
That keeps first demand aligned with real capacity, so the opening week builds cleanly instead of creating cash strain, missed appointments, and rushed documentation.
6
Related Products
- Neuromuscular Training Program Porter's Five Forces Analysis
- Neuromuscular Training Program BCG Matrix
- Neuromuscular Training Program Business Model Canvas
- What Are The 5 KPI Metrics For Neuromuscular Training Program Business?
- Neuromuscular Training Program Business Plan Template in Pre-Written Word
- How Increase Neuromuscular Training Program Profitability?
- How Increase Neuromuscular Training Program Profitability?
- Neuromuscular Training Program Startup Costs: $730k Funding Plan
- Neuromuscular Training Program Financial Model Template in Excel
- Neuromuscular Training Program Owner Income: $145K Plus Profit
- How To Write A Business Plan For Neuromuscular Training Program?
- Neuromuscular Training Program Marketing Mix
- Neuromuscular Training Program Marketing Plan
- Neuromuscular Training Program Business Proposal
- Neuromuscular Training Program PESTEL Analysis
- Neuromuscular Training Program Pitch Deck Example Editable PPTX
- Neuromuscular Training Program Business SWOT Analysis
- Neuromuscular Training Program Value Proposition Canvas
Frequently Asked Questions
Start by confirming licensure, scope, and documentation before marketing Then build assessment protocols, train staff, set up EHR and billing, prepare the treatment space, and secure referral partners The researched launch window is 8 to 16 weeks, with the base Year 1 plan using 8 clinical providers and 686 modeled monthly treatments