 Owner income$85.4k
Owner income$85.4kHow Much Non-Invasive Body Sculpting Clinic Owners Make at $1478K/Month

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$85.4k  Net margin62.1%
Net margin62.1% Revenue for target pay$1.65M
Revenue for target pay$1.65M Business difficultyHard
Business difficultyHard


You’re trying to separate clinic revenue from real owner take-home This five-year US clinic model uses $147,800/month in first-year treatment revenue and $1,047,480/month in mature-year treatment revenue, then layers in COGS, marketing, merchant fees, fixed overhead, visible admin payroll, reserves, and owner role assumptions
Owner income$85.4kNet margin62.1%Revenue for target pay$1.65MBusiness difficultyHardWant to test your own clinic numbers?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only, not guaranteed salary, tax advice, or owner distribution advice. It excludes taxes, personal debt, buildout overruns, and lender underwriting.
Want to see the full income model for a Non-Invasive Body Sculpting Clinic?
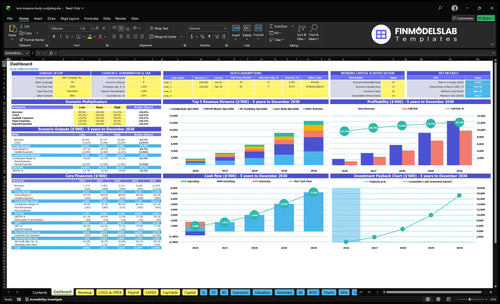
The Non-Invasive Body Sculpting Clinic Financial Model Template shows revenue, margin, cash flow, and owner pay, plus first-year $147,800/month and mature-year $1,047,480/month views. Open the model for the assumptions and scenarios.
Owner-income model highlights
- Owner pay and distributions
- Revenue, margin, cash flow
- Assumptions and scenario tabs
What body sculpting clinic profit margin should owners expect?
Owners should treat profit margin as a range, not a promise. In a Non-Invasive Body Sculpting Clinic, the first-year model can look strong on paper, but How To Write A Business Plan To Launch Non-Invasive Body Sculpting Clinic? matters because costs like 85% consumables, 40% device maintenance and per-use licensing, 60% digital marketing, and 30% merchant fees can move fast.
Cost stack
- 85% consumables hit every treatment
- 40% device maintenance and licensing
- 60% digital marketing can drain cash
- 30% merchant fees cut receipts
Margin risk
- $20,050 fixed overhead still needs coverage
- $10,583 visible admin payroll is built in
- Modeled first-year margin is about 578%
- Low utilization can cut owner income fast
How much revenue does a body sculpting clinic need to pay the owner?
If the owner wants to take home $20,000 a month, the Non-Invasive Body Sculpting Clinic needs about $64,500 in monthly revenue before provider pay, equipment payments, reserves, and taxes. Here’s the quick math: fixed overhead is $20,050 a month, visible admin payroll is $10,583, and known variable costs run at 21.5% of revenue, so only 78.5% is left to cover owner pay and the other missing cost lines.
Core cost stack
- $20,050 fixed overhead monthly
- $10,583 admin payroll monthly
- 21.5% of revenue is variable cost
- 78.5% remains before missing lines
Revenue target math
- $20,000 owner pay target
- $30,633 known fixed monthly cost base
- About $64,500 needed monthly revenue
- Before provider pay, equipment, reserves, taxes
How much can a body sculpting clinic owner make?
A Non-Invasive Body Sculpting Clinic owner can show about $85,400/month in pre-tax owner take-home potential in year one under this model, not salary; for setup context, see How To Launch Noninvasive Body Sculpting Clinic Business?. Mature-year revenue reaches $1,047,480/month, but staffing, quality control, debt, and cash reserves can shrink actual take-home fast.
Year-one math
- $147,800/month first-year revenue
- 12.5% COGS assumed
- 9.0% marketing and merchant fees
- $30,633 fixed overhead plus admin payroll
Owner reality
- Provider pay comes out next
- Equipment financing can cut cash flow
- Reserve policy changes owner distributions
- Utilization and pricing drive income
Want the six main income drivers?
1
520/moAppointment Load
At 520 treatments a month, the clinic can spread fixed costs across enough visits to turn volume into cash.
2
$400-$900Package Price
That price spread across the core offers is the fastest way to lift revenue without adding more visits.
3
6%-4%Lead Cost
Marketing runs at 6% of revenue in year 1 and falls to 4%, so conversion quality directly protects margin.
4
6-20 FTEProvider Labor
The team grows from 6 to 20 FTE across the plan, so payroll discipline matters as much as bookings.
5
$20.1K/moOverhead Floor
Rent, oversight, software, and disposal create a monthly floor the clinic must cover before owner cash builds.
6
$755KEquipment Cost
The device suite and fit-out need $755K upfront, so funding terms affect payback more than top-line growth.
Non-Invasive Body Sculpting Clinic Core Six Income Drivers
Appointment Volume and Device Utilization
Appointment Volume and Device Use
Utilization means how much of your bookable device and room time turns into paid sessions. Because rent and equipment are fixed once the clinic opens, every empty slot lowers income twice: you lose revenue and still pay the same overhead. The model shows $147,800/month in first-year revenue from paid booked sessions, with utilization running from 300% for laser body treatments to 500% for nurse practitioner-led treatments.
Here’s the quick math: moving from 300% toward mature-year 650% to 800% utilization changes owner take-home far more than small price tweaks. What this estimate hides is no-shows, long room turnover, and weak scheduling. If paid bookings slip, fixed lease, medical director, and admin costs stay in place, so profit and owner draw drop fast.
Fill Paid Slots First
Track booked sessions per device hour, show rate, turnover minutes, and paid treatments per provider per month. Use those numbers to see whether the calendar, not demand, is the bottleneck. One clean rule: fill the schedule before you discount packages.
- Measure paid sessions, not inquiries.
- Watch no-shows and late cancels.
- Cut room turnover with tighter blocks.
- Use waitlists to backfill openings.
Recheck the schedule weekly against the $147,800/month target and the 300% to 500% first-year utilization band. If no-shows rise or turnover runs long, tighten deposits and slot rules before you add more devices or staff.
1
Average Package Price
Average Package Price
Average package price is the blended amount per sold treatment package: revenue divided by packages sold. The listed first-year prices run from $400 for radiofrequency sculpting to $900 for nurse practitioner-led treatments; if one of each sold equally, the simple average is $630. Higher pricing lifts revenue dollar-for-dollar before percentage costs, so it flows straight into owner income.
The catch is conversion. A $900 package only helps if the consult closes; if the clinic discounts to fill the schedule, revenue per slot falls and cash for payroll, financing, reserves, and owner distributions shrinks. With fixed overhead already at $20,050/month, price cuts need real volume lift to pay off.
Track Selling Price by Service
Track average selling price by service, not just total revenue. Break out closes for cryolipolysis ($750), high-intensity focused electromagnetic muscle treatments ($500), radiofrequency sculpting ($400), laser body treatments ($600), and nurse practitioner-led treatments ($900). That shows which offer supports margin and which one only fills gaps.
Test price changes against consult conversion and refund rate before you roll them out. If a lower price fills the calendar but lowers cash, it can hurt owner pay even when utilization looks strong. Raise price only when booked consults, show rates, and close rates hold, so each slot still clears overhead and leaves distributable cash.
2
Marketing Cost and Lead Conversion
Lead Cost and Close Rate
Paid demand can make a clinic look busy while owner pay stays thin. In this model, digital marketing and lead acquisition are 60% of first-year revenue and still 40% in a mature year, while merchant fees stay at 30%. That means cash gets tight fast if booked consults, show rate, and close rate are weak.
More leads do not fix income if the team discounts hard or refunds rise. The key inputs are cost per booked consult, show rate, close rate, package size, and refund risk. High traffic with poor follow-up can fill the calendar and still leave little cash for payroll, debt, or owner draw.
Track Conversion, Not Lead Count
Track each step from lead to booked consult to sale. If 60% of revenue goes to marketing, every bad lead hurts twice: it costs cash up front and lowers the chance of a paid treatment. Better show rate and close rate lift take-home income more than buying more traffic.
Use a weekly scorecard: cost per booked consult, show rate, close rate (the share that buys), average package size, and refund rate. If follow-up takes too long, conversion drops and the marketing bill stays the same. In a mature year, the 40% marketing load helps, but only if discounting stays controlled.
- Lead-to-book rate
- Consult show rate
- Close rate
- Average package size
- Refund rate
3
Staffing Costs and Provider Productivity
Staffing Costs and Provider Productivity
This driver covers the people who turn bookings into completed treatments. Admin payroll starts with a $85,000 clinic operations manager and one $42,000 receptionist, or about $10,583/month combined, before clinical payroll. Because clinical roles rise from 6 in year one to 20 in mature year, labor can grow faster than revenue if schedule fill stays weak.
Provider pay rates are not provided, so final owner take-home cannot be completed from the data. The key measure is paid treatments per provider per month. If headcount rises but paid treatments per provider do not, labor pressure hits gross margin, cash flow, and the owner’s draw long before demand looks full.
Track Paid Treatments Per Provider
Track paid treatments per provider per month, show rate, and booked hours by role. Tie hiring to actual throughput, not planned capacity. One clean rule: do not add a provider unless the new monthly labor cost is supported by repeatable paid volume, not just consult leads.
- Watch paid treatments per provider.
- Track no-shows by provider.
- Forecast payroll before hiring.
If utilization slips, extend hours, tighten scheduling, and cut idle room time before adding headcount. That keeps payroll from outrunning collections and protects the cash left for taxes, reserves, and owner pay.
4
Equipment Financing and Maintenance
Device Cash Cost
This driver covers device lease or loan payments, maintenance, and per-use licensing, meaning fees tied to each treatment. It hits owner income directly because these costs are paid before profit gets to the owner. With maintenance and licensing modeled at 40% of first-year revenue and 32% in mature year, a clinic at $147,800/month revenue gives up about $59,120/month before financing.
Downtime, warranty gaps, service contracts, and upgrade cycles can make gross margin look better than cash. If a device sits idle or needs repairs, the owner still pays payroll, rent, and overhead. Since equipment lease or loan payments are not provided, they must be entered before owner pay is trusted. The real test is cash left after device costs, not paper profit.
Track Uptime and Device Fees
Build a device-level cash sheet. Track treatments per device, uptime, maintenance, per-use licensin g, service contract cost, and lease or loan payment. Per-use licensing is a fee charged each time the device is used. Here’s the quick math: if uptime falls, the same fixed payment gets spread over fewer treatments, so owner draw drops fast.
- Track treatments per device.
- Log downtime by hour.
- Enter lease or loan payments.
- Review service contract terms.
- Price for upgrade cycles.
Test pricing and scheduling against cash, not just gross margin. If licensing or repair spend rises, adjust package price, tighten utilization, or hold more cash before distributions. Reserve funds for warranty gaps and replacements so one repair cycle does not wipe out monthly owner pay.
5
Fixed Overhead and Cash Reserves
Fixed Overhead and Cash Reserves
$20,050 a month in fixed overhead comes out before the owner gets paid: $12,000 lease, $3,500 medical director oversight, $1,200 utilities and internet, $1,800 insurance, $600 software, and $950 janitorial and medical waste disposal. That is $240,600 a year before any owner draw, so cash flow has to clear this floor first.
Reserves are not leftover cash. They cover refunds, repairs, slow lead flow, payroll timing, and device issues, and they protect owner income when booked treatments slip or collections lag. If cash sits tight, distributions should wait.
Hold Cash Before Owner Pay
Track fixed overhead as a monthly run rate, then compare it with cash collected, not just booked revenue. Keep a reserve bucket for refund risk, equipment downtime, and payroll gaps so owner pay does not depend on a strong week.
- Measure cash on hand weekly.
- Track refunds and repair calls.
- Review payroll dates and lease timing.
- Delay distributions until reserves are funded.
Here’s the quick math: every month, the clinic must cover $20,050 before profit starts. If lead flow slows or a device goes down, reserves keep the business paying bills without forcing the owner to take a cut in pay.
6
Compare low, base, and high owner-income assumptions
Owner income scenarios
Owner income shifts fast here because utilization, pricing, staffing mix, and financing load all move the margin. The low, base, and high cases show cash left before provider pay, reserves, and taxes.
| Scenario | Low CaseDownside case | Base CaseModel case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the lower earnings path if utilization stays soft and fixed costs absorb more of the margin. | This is the modeled path if volume, pricing, and staffing hold near plan. | This is the stronger earnings path if utilization, pricing, and financing stay favorable. |
| Typical setup | First-year model at $147,800 monthly revenue, 78.5% contribution margin before fixed costs, $20,050 fixed overhead, and $10,583 visible admin payroll, leaving about $85,400 monthly before provider pay, equipment, reserves, and taxes. | Year 3 revenue of $480,120 monthly, 80.9% contribution margin before fixed costs, and about $354,300 monthly before missing costs. | Mature-year revenue of $1,047,480 monthly, 83.3% contribution margin before fixed costs, and about $834,900 monthly before missing costs. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $85.4k/monthIncome floor | $354.3k/monthCore plan | $834.9k/monthUpside test |
| Best fit | Use this to stress test the clinic if bookings start slow or staffing costs run hot. | Use this as the main operating case for budgeting, hiring, and cash planning. | Use this to test the upper end of owner income when the clinic is full and costs stay tight. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Non-Invasive Body Sculpting Clinic Porter's Five Forces Analysis
- Non-Invasive Body Sculpting Clinic BCG Matrix
- Non-Invasive Body Sculpting Clinic Business Model Canvas
- What 5 KPIs Matter For Non-Invasive Body Sculpting Clinic Business?
- Non-Invasive Body Sculpting Clinic Business Plan Template in Pre-Written Word
- How Increase Profits Non-Invasive Body Sculpting Clinic?
- What Are Operating Costs For Non-Invasive Body Sculpting Clinic?
- Non-Invasive Body Sculpting Clinic Startup Costs: $740K+ CAPEX
- Non-Invasive Body Sculpting Clinic Financial Model Template in Excel
- How To Open A Body Sculpting Clinic In 3 To 6 Months
- How To Write A Business Plan To Launch Non-Invasive Body Sculpting Clinic?
- Non-Invasive Body Sculpting Clinic Marketing Mix
- Non-Invasive Body Sculpting Clinic Marketing Plan
- Non-Invasive Body Sculpting Clinic Business Proposal
- Non-Invasive Body Sculpting Clinic PESTEL Analysis
- Non-Invasive Body Sculpting Clinic Pitch Deck Example Editable PPTX
- Non-Invasive Body Sculpting Clinic Business SWOT Analysis
- Non-Invasive Body Sculpting Clinic Value Proposition Canvas
Frequently Asked Questions
The first-year model leaves about $85,400/month after COGS, marketing, merchant fees, fixed overhead, and visible admin payroll That is not the owner draw Provider pay, equipment financing, reserves, taxes, and reinvestment still come out before safe distributions