 Owner income$120k-$1.79M
Owner income$120k-$1.79MHow Much Can An Occupational Therapy Clinic Owner Make On $790K Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$120k-$1.79M  Net margin-21% to 42%
Net margin-21% to 42% Revenue for target pay$791k
Revenue for target pay$791k Business difficultyHard
Business difficultyHard


An occupational therapy clinic owner can make little or no distributable profit in the first year if payroll and overhead are built ahead of volume Using the researched assumptions, first-year revenue is about $790,770, but known operating costs produce about a $166,800 operating loss after a $120,000 Clinic Director salary By Year 3, revenue reaches about $210 million and operating profit is about $493,000 before taxes, debt, and reserves Owner income depends on clinic size, payer mix, utilization, cancellations, staffing model, and whether the owner treats patients or fills the Clinic Director role
Owner income$120k-$1.79MNet margin-21% to 42%Revenue for target pay$791kBusiness difficultyHardWant to estimate your OT clinic owner income
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
How do you check owner income in an Occupational Therapy Clinic forecast?
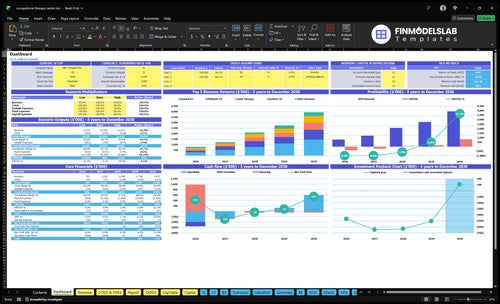
This dashboard shows revenue, visits, margins, cash flow, and owner pay assumptions; open the Occupational Therapy Clinic Financial Model Template.
Owner-income model highlights
- Owner pay stays flexible
- Revenue, visits, margins
- Tests staffing and break-even
What profit margin can an occupational therapy clinic reach
In this model, an Occupational Therapy Clinic can swing from -211% operating profit margin in Year 1 to 235% in Year 3 and 424% in Year 5, driven by treatment pricing and what the clinic actually collects; for startup cost context, see How Much Does It Cost To Open An Occupational Therapy Clinic?. The key point is simple: one reimbursement rate is not national, because payer mix changes the result fast.
Pricing shifts margin
- $145 to $200 per treatment in Year 1
- $165 to $220 per treatment in Year 5
- Higher rates lift collected revenue fast
- Margin can turn sharply with volume
Payer mix matters
- Medicare and Medicaid pay differently
- Commercial insurance changes collections
- Private pay and school contracts vary
- Authorizations, denials, and no-shows hit revenue
How much revenue does an OT clinic need for owner salary
The Occupational Therapy Clinic needs about $988,000 in annual revenue to cover payroll, fixed overhead, and a $120,000 Clinic Director salary. Here’s the quick math: $835,000 of fixed costs plus known payroll, divided by an 84.5% contribution margin, gets you there. At $159 average revenue per completed visit, that means about 6,200 visits a year, or 517 visits a month.
Revenue math
- $988,000 target revenue
- $835,000 fixed cost base
- 84.5% contribution margin
- $159 per completed visit
Visit volume gap
- 6,200 visits per year needed
- 517 visits per month needed
- 414 visits per month planned
- 103 visits short each month
Does hiring therapists increase an occupational therapy clinic owner’s income
Hiring therapists raises income only if referral volume and utilization keep paid clinician time full. In an Occupational Therapy Clinic, the model grows from 6 therapist FTE in Year 1 to 18 therapist FTE in Year 5, so the cash risk is highest early when utilization sits at 50% to 65%. By Year 5, 70% to 85% utilization can support better margins, and an owner-as-clinician may protect cash sooner while an owner-as-manager needs tighter scheduling, supervision, and billing.
Early-stage risk
- 6 therapist FTE in Year 1
- 50% to 65% utilization
- Payroll risk stays high
- Owner-as-clinician can protect cash
Scale-up margin
- 18 therapist FTE by Year 5
- 70% to 85% utilization
- Margins improve when schedules fill
- Owner-as-manager needs tighter systems
Want the six main OT clinic income drivers
1
4.96KCompleted Visits
Year 1 is about 4,962 visits, and every extra completed visit adds revenue before overhead, taxes, and reserves.
2
50%-65%Clinician Utilization
Moving from 50% to 65% utilization turns paid therapist time into more billable care without the same jump in fixed cost.
3
$159Reimbursement Mix
The mix of service lines drives average Year 1 revenue per visit, which is about $159, so better mix lifts take-home on the same schedule.
4
$80KClinical Labor Cost
Therapist pay starts at $80K per FTE, so staffing choices have a direct hit on EBITDA.
5
$135KFixed Overhead
Fixed overhead runs about $135K a year, so rent, admin, and software control decide how fast the clinic reaches owner income.
6
15.5%Collections
Missed visits and slower collections squeeze cash, while Year 1 variable and COGS still run 15.5% of revenue.
Occupational Therapy Clinic Core Six Income Drivers
Completed Visit Volume
Completed Billable Visits
Completed billable visits are the visits that actually get paid, so they’re the first step that turns therapist time into cash. In this model, Year 1 reaches about 4,962 completed visits, Year 3 about 12,516, and Year 5 about 22,056. Scheduled visits do not count if patients cancel, authorizations lag, or claims fail.
Owner pay starts after those visits cover therapist payroll, billing fees, rent, and admin. Here’s the quick math: completed visits × collected rate per visit = revenue. If completions rise without a matching jump in overhead, more of each extra dollar can flow to profit and the owner draw.
Fill Open Therapist Time First
Track scheduled visits, completed visits, cancellation rate, authorization lag, and denial rate every week. The goal is simple: keep paid therapist time full before adding more payroll. If a therapist has open slots, fill those first; that usually raises revenue faster than hiring, while rent and admin costs stay flatter.
Use a dashboard that shows scheduled-to-completed conversion by therapist and payer. A clinic can look busy and still miss cash if visits fall through. When completions slip, cash flow tightens fast, because fixed costs still run even when the calendar was full.
- Count only paid visits.
- Watch cancellations weekly.
- Track payer delays fast.
1
Reimbursement And Payer Mix
Reimbursement and Payer Mix
Average collected reimbursement is the main revenue lever here. In Year 1, treatment prices range from $145 for geriatric OT to $200 for ergonomics, and the model shows about $159 per completed visit. By Year 5, that rises to $165 to $220, with modeled revenue near $179 per visit. If collections slip or the mix skews to lower-paying work, owner distributions shrink fast.
This driver includes state rates, payer contracts, setting, authorization rules, and collection performance. Here’s the quick math: completed visits × collected rate = revenue. At Year 1 volume of 4,962 visits and $159 per visit, revenue is about $788,958. That same volume at a weaker mix would leave less gross margin for payroll, billing, and owner pay.
Track net rate by visit
Measure net collected reimbursement by service line, payer, and therapist. Compare billed charge, allowed amount, collected amount, and denial rate each month. If ergonomics is near $200 while geriatric OT is near $145, the visit mix matters as much as volume. One clean rule: protect the visits that lift average net revenue per completed session.
Use a simple dashboard: payer mix, authorization lag, denial rate, and collection speed. Test whether better scheduling, cleaner documentation, or tighter verification shifts collected reimbursement toward the modeled path from $159 in Year 1 to $168 in Year 3 and $179 in Year 5. If the mix drifts lower, owner pay gets squeezed even when the schedule stays full.
- Track net revenue per completed visit.
- Separate rates by payer and service.
- Review denials and authorizations weekly.
- Watch collection speed by claim age.
2
Therapist Productivity And Utilization
Therapist Utilization
Utilization is the share of paid clinician time that turns into billable visits. At 50%, half of the therapist salary sits on nonbillable work, so the $80,000 cost is harder to cover; by 70% to 85%, much more of that pay is funded by revenue and gross margin improves.
Here’s the quick math: this driver depends on paid hours, billable hours, documentation, admin work, supervision, and care coordination. Do not assume every scheduled hour is revenue. If utilization stays low, fixed salary and overhead stay in place while collected visits lag, which cuts the owner’s take-home pay.
Track Billable Hours First
Measure utilization by therapist each week as billable hours ÷ paid hours. Compare service lines too: Year 1 ranges from 50% for ergonomics to 65% for general occupational therapy, so a new line should not be forecast like a mature one.
- Paid hours by therapist
- Billable hours by therapist
- Cancellations and no-shows
- Documentation and admin time
- Authorization and care coordination lag
Fill open slots before adding payroll. Better scheduling pushes utilization toward the 70% to 85% Year 5 range, spreads the same salary over more visits, and lifts cash available for owner draw.
3
Clinical Labor Cost
Clinical Labor Cost
Therapist payroll is the biggest known cost here. The model uses $80,000 per Occupational Therapist FTE, rising from 6 FTE in Year 1 to 18 FTE in Year 5, so base clinical labor runs from about $480,000 to $1.44 million a year before payroll taxes, benefits, assistants, or contractors.
This cost hits owner income through gross margin and cash flow. If hiring gets ahead of billed visits, profit can look fine on paper while cash stays tight. Keep clinical labor separate from owner pay and admin overhead so you can see whether added staff are paying for themselves.
Track FTE Before You Hire
Measure clinical labor per completed visit, not just headcount. Here’s the quick math: 6 FTE × $80,000 = $480,000 in Year 1 and 18 FTE × $80,000 = $1.44 million in Year 5. If payroll rises faster than completed visits, owner take-home gets squeezed fast.
Track these inputs monthly: therapist FTE, assistants, contractors, payroll taxes, benefits, supervision load, and billable visits. A simple rule helps: don’t add full-time clinicians until schedule fill, authorization flow, and collections can cover the next payroll cycle. Hiring early can turn growth into cash pressure.
- Track FTE by clinician type.
- Separate owner pay from clinic payroll.
- Compare payroll to completed visits.
- Test staffing before adding headcount.
4
No-Shows, Denials, And Collections
No-Shows and Collection Leakage
No-shows, denials, and slow collections cut top-line cash before the owner sees profit. In Year 1, the clinic has $135,000 of fixed overhead, so every missed visit hurts because rent, salaries, software, and insurance still run. At an average of $159 per completed visit, 100 l ost visits is about $15,900 in missed revenue, before billing fees.
This driver includes eligibility checks, authorization tracking, denial follow-up, reminder workflows, and patient balance collection. Billing service fees are 40% of revenue in Year 1 and 35% in Year 5, so weak clean-claim and collection rates squeeze owner pay fast. If onboarding or payer approvals slow cash, the clinic may need reserve cash to cover payroll and overhead.
Tighten Claims, Reminders, And Balances
Track missed-visit rate, denial rate, days to collect, and patient balance recovery each month. Here’s the quick math: the more visits that fail to bill or collect, the less cash is left after the $135,000 fixed overhead and the 40% Year 1 billing fee. One clean one-liner: cash flow is won or lost before the statement closes.
- Check eligibility before every start.
- Track authorizations by payer.
- Follow up denials weekly.
- Send reminders before each visit.
- Collect balances at service and after.
What this hides: if payer approvals slow, revenue can lag even when schedules look full. Build a reserve so payroll and rent stay covered while claims work through the system. If collections improve, more of each billed dollar stays available for owner draw.
5
Fixed Overhead Control
Fixed Overhead Control
Fixed overhead is the monthly bill you pay even when visits are light. Here it totals $11,250 per month—$7,500 rent, $1,000 utilities, $750 liability insurance, $800 software, $400 supplies and maintenance, $200 licensing, and $600 IT support. That is $135,000 per year before the owner takes anything home.
This cost sets the downside risk: if completed visits or collections slip, profit and cash fall fast because these bills still run. The owner only pays themselves after gross profit and labor cover this base. One clean rule: keep fixed overhead low enough that the business can survive a slow month without borrowing.
Track the fixed-cost floor
Build the budget from the actual monthly lines, then compare them to collected revenue each month. Use rent, utilities, insurance, software, supplies and maintenance, licensing, and IT support as the core inputs, and watch the ratio of fixed overhead to collected visits and gross margin. If overhead climbs faster than visits, owner draw gets squeezed.
- Track fixed costs at $11,250 monthly.
- Review any increase before signing.
- Use shared admin tools as volume rises.
- Delay hires until visits support them.
Scalable admin systems matter because they spread the same $135,000 annual base across more completed visits. What this hides: if onboarding or billing slows collections, even small fixed costs can drain cash. Set a monthly ceiling for overhead and test it against current visit volume before adding more space or software.
6
Compare low, base, and high OT clinic owner income scenarios
Owner income scenarios
Owner income moves with visits, utilization, pricing, and payroll. The low, base, and high cases show how this clinic can shift from loss to strong profit as capacity fills.
| Scenario | Low CaseDownside case | Base CaseCore case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the lower-earnings path where the clinic runs below full capacity and owner income stays under pressure. | This is the modeled middle path where steady volume and staffing lift owner income into the main plan. | This is the stronger-earnings path where higher visit volume and fuller capacity push owner income up fast. |
| Typical setup | Year 1 models about 4,962 visits, $790,770 revenue, 50% to 65% utilization, about $700,000 payroll, and about $135,000 fixed overhead, with operating profit near negative $166,800 before owner pay. | Year 3 models about 12,516 visits, $2,099,010 revenue, 60% to 75% utilization, and about $493,000 operating profit before owner pay. | Year 5 models about 22,056 visits, $3,937,320 revenue, 70% to 85% utilization, and about $167 million operating profit before owner pay. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $-166.8kLoss risk | $493kCore plan | $167MUpside run |
| Best fit | Use this to stress-test a slow ramp, weaker throughput, and heavier payroll load. | Use this as the main planning case for a clinic that settles into steady demand and tighter staffing. | Use this to test the upside if the clinic fills capacity and keeps volume growth strong. |
Planning note: These scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Occupational Therapy Clinic Porter's Five Forces Analysis
- Occupational Therapy Clinic BCG Matrix
- Occupational Therapy Clinic Business Model Canvas
- 7 Critical KPIs to Track for Your Occupational Therapy Clinic
- Occupational Therapy Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Occupational Therapy Clinic Profitability
- How Much Does It Cost To Run An Occupational Therapy Clinic Monthly?
- Occupational Therapy Clinic Startup Costs: $165K CAPEX Before Cash Reserve
- Occupational Therapy Clinic Financial Model Template in Excel
- How To Open An Occupational Therapy Clinic In 4-9 Months
- How to Write an Occupational Therapy Clinic Business Plan
- Occupational Therapy Clinic Marketing Mix
- Occupational Therapy Clinic Marketing Plan
- Occupational Therapy Clinic Business Proposal
- Occupational Therapy Clinic PESTEL Analysis
- Occupational Therapy Clinic Pitch Deck Example Editable PPTX
- Occupational Therapy Clinic Business SWOT Analysis
- Occupational Therapy Clinic Value Proposition Canvas
Frequently Asked Questions
In this model, first-year distributions are not supported because operating profit is about negative $166,800 after known costs If the owner fills the $120,000 Clinic Director role, that salary is separate from profit By Year 3, operating profit reaches about $493,000 before taxes, debt, and reserves