 Time to Open8-12 weeksLaunch runway
Time to Open8-12 weeksLaunch runwayOpen an Online Medical Consultation Business With First Visits in 8–16 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open8-12 weeksLaunch runway  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckLicense gateState rules
Key BottleneckLicense gateState rules First Revenue StepPaid consultsBooking live
First Revenue StepPaid consultsBooking live


You’re building a care service before the first patient books, so launch readiness matters more than a logo or app polish This guide covers the 8–16 week US setup path: Health Insurance Portability and Accountability Act (HIPAA) readiness, licensed clinicians, secure visits, intake, billing, first bookings, and Month 1 model checks across a 60-month plan
Time to Open8-12 weeksLaunch runwayLaunch Sequence6 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepPaid consultsBooking liveLaunch timeline
Short web summary of the launch timeline; the XLSX export holds the detailed Gantt chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12Week 13Week 14Week 15Week 16
Compliance
- Entity filing
- State scope review
- HIPAA policies
- Malpractice coverage
- Licensure checks
Technology
- Platform shortlist
- Secure video setup
- Intake forms build
- Scheduling rules
- Documentation templates
Providers
- Physician outreach
- Contract drafts
- Credential checks
- On-call roster
- Backup bench
Clinical Ops
- Care scope map
- Triage protocols
- Test consults
- Support scripts
- Follow-up rules
Payments
- Payment gateway setup
- Refund policy
- Payer enrollment
- Reconciliation workflow
- Billing test run
Marketing
- Booking pages
- Lead capture setup
- Launch content
- Pilot campaign
- Go-live decision
Want to test the launch plan before go-live?
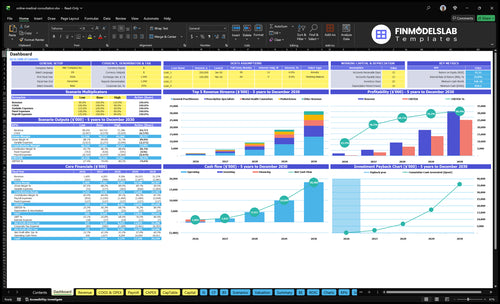
If you’re pre-launch, the Online Medical Consultation Financial Model Template uses dashboard and model tabs to show revenue, costs, cash needs, assumptions, and break-even logic, so you can test 8–16 week launch timing and runway before go-live. Year 1 uses 10 general practitioners, 5 mental health counselors, 8 prescription specialists, 3 pediatricians, and 2 dermatologists; at $49 to $99 per visit, the case lands near 1,932 consultations and $133,760 monthly revenue. Open the model.
Launch model highlights
- Staffing schedule by line
- Cash runway tracking
- Breakeven sensitivity charts
How do you get first telemedicine patients?
To get your first patients for Online Medical Consultation, start with one patient segment or condition, build local and condition-specific booking pages, and only test paid search after booking works; if you need a cost frame, see What Is The Estimated Cost To Open And Launch Your Online Medical Consultation Business? First revenue matters more than broad brand work, because Year 1 capacity needs about 1,932 completed consultations/month, so the first win is reliable paid bookings, not national awareness. Ask employers, clinics, pharmacies, and wellness providers for referral pilots, then track visitor-to-booking, booking-to-completed-visit, no-show, refund, and follow-up rates.
Start with one segment
- Pick one condition first.
- Build local booking pages.
- Make mobile booking fast.
- Test paid search later.
Measure paid demand
- Track visitor-to-booking rate.
- Track completed-visit rate.
- Track no-show rate closely.
- Track referral pilot results.
How long does it take to launch a telemedicine business?
Online Medical Consultation usually takes 8–16 weeks to launch, and Month 1 should start only after the patient journey works end to end. Faster launches use limited states, self-pay visits, simpler services, and available clinicians; slower launches get held up by multi-state licensure, payer billing, credentialing, protocol review, and platform setup. If clinician onboarding takes 14+ days per clinician, launch risk rises.
Faster launch path
- Start with 1–2 states
- Use self-pay pricing
- Offer simple consults first
- Use ready clinicians
Common delay points
- Multi-state licensure scope
- Payer billing setup
- Protocol approval delays
- Onboarding over 14 days
What are the biggest telemedicine launch mistakes?
The biggest launch mistakes are skipping compliance, marketing in states where providers are not licensed, and turning on too many service lines at once. For Online Medical Consultation, the day-one failures are usually failed consent capture, missed payments, incomplete documentation, and weak patient handoffs. Start with one niche, then phase the 5 planned service lines only after the first workflow is stable.
Launch risks
- Check licensure before ads.
- Define clinical scope clearly.
- Write prescription boundaries.
- Keep provider coverage steady.
Day-one workflow
- Test intake forms end to end.
- Test video before go-live.
- Test scheduling and payments.
- Set referral and support handoffs.
Confirm what must be ready before accepting patients
Launch readiness checklist
Use this go-live approval checklist before opening the online medical consultation service.
Compliance
- Entity formedCritical
Formation keeps contracts, billing, and liability clean before patient traffic starts.
- State licensure mappedCritical
Licensure must match every state you will treat.
- HIPAA notice approvedCritical
Patients need the notice before any visit or data capture.
- Malpractice coverage activeCritical
Coverage should be active before the first consultation.
Care workflow
- Telehealth consent capturedCritical
Consent needs to be captured before intake or video starts.
- Clinical protocols approvedCritical
Protocols reduce provider drift and missed escalations.
- Intake workflow testedHigh
Intake must work without manual rescue.
- Follow-up escalation definedHigh
Escalation rules protect patients when symptoms worsen.
Platform
- Video, phone, chat testedCritical
All three channels must work for live visits.
- Scheduling and reminders liveHigh
Reminders cut no-shows and support same-day flow.
- EHR charting readyCritical
Charting has to sync with the visit record.
- Privacy controls checkedCritical
Privacy controls protect PHI and limit access.
Providers
- Clinician onboarding completeCritical
Every doctor needs clean onboarding before go-live.
- Credentialing files verifiedCritical
Credentialing avoids blocked visits and billing issues.
- Coverage schedule approvedHigh
Coverage gaps break same-day patient promises.
- Backup coverage assignedHigh
Backups keep service live when a clinician drops.
Launch
- Launch pricing approvedHigh
Price points must match the $49-$99 launch plan.
- Booking flow liveCritical
Booking has to work from the first click.
- Payment flow testedCritical
Payment must clear before the visit is confirmed.
- Patient support scripts readyHigh
Scripts keep support fast when issues pop up.
Cash
- Fixed cost budget lockedCritical
At $10,600 monthly fixed cost, cash needs to absorb slow ramp.
- Cash runway reviewedCritical
Minimum cash is $829k in Month 2.
- Capacity model reconciledHigh
Capacity should match provider counts, visit load, and launch demand.
- Go-live signoff completedCritical
Final signoff means every launch gate is green.
Which six launch drivers matter most?
1Compliance Gate
8-16 wksLaunch slips if licenses, consent, and prescribing rules are not mapped before marketing starts.
2HIPAA Stack
Test visitA secure booking-to-care flow cuts failed visits and reduces manual admin before go-live.
3Clinician Capacity
28 cliniciansYear 1 staffing needs 28 clinicians, or booked slots will fill before demand stabilizes.
4Clinical Workflow
1,932/moClean intake, routing, and follow-up keep the 1,932 monthly modeled consultations from turning messy.
5Billing Setup
$49-$99Simple paid-at-booking billing supports the $49-$99 visit range and speeds first revenue.
6Patient Engine
$10.6K/moMarketing must convert fast; a 170% variable load and $10.6K fixed costs leave little room for wasted traffic.
Compliance and Licensure Readiness
Licensure and Compliance Readiness
Open-on-time depends on having a state-by-state launch matrix before marketing starts. If a provider is not licensed in the patient’s state, or the service scope is unclear, you cannot safely route that visit on day one, and the team ends up reworking bookings instead of treating patients.
This driver also covers telehealth consent, privacy policy, malpractice coverage, prescribing rules, and clinical documentation. The real risk is simple: selling access before compliant coverage exists. That creates launch delays, patient frustration, and messy onboarding for clinicians who are not cleared for the right states or services.
Build the launch matrix first
Verify the legal entity, care scope, provider license status, consent language, privacy workflow, malpractice policy, and prescription boundaries before any public launch. One clean rule: if it is not in the matrix, it is not live.
Assign each state to a named clinician and service line, then test a mock intake against that setup. That shows who can treat which patients, what can be prescribed, and where the visit must be routed. It also makes provider onboarding cleaner because the rules are written before the first appointment is booked.
- Match licenses to patient states.
- Approve consent and privacy flow.
- Confirm malpractice coverage dates.
- Set prescribing limits by state.
- Document visit templates and records.
1
HIPAA-Ready Technology Stack
Secure Stack Before Go-Live
A telemedicine launch stalls fast if the platform can’t handle secure video, chat, or phone plus intake, scheduling, notifications, payments, support, and visit notes. The real test is simple: a test patient can book, pay, consent, join, get care, receive follow-up, and leave a complete record without staff workarounds.
This depends on signed vendor agreements and configured access controls. The electronic health record (EHR), the system used to store patient charts and visit notes, must be ready before first revenue. If setup is weak, you get failed visits, manual admin work, and messy records on day one.
Test the Full Patient Loop
Build the launch plan around one live-style walkthrough, not separate software checks. Confirm the booking page, payment flow, consent, video link, documentation, and follow-up message all work in one chain. That is the clean readiness signal, and it tells you if the stack can actually support care.
Use a short go-live checklist and assign one owner for each step. Verify vendor contracts, role-based access, and staff permissions before launch. One broken handoff can delay opening, while a clean end-to-end test lowers support tickets and keeps clinicians focused on care instead of fixing admin issues.
- Confirm vendor agreements first.
- Set access by role.
- Test one complete patient journey.
- Check EHR note saving.
- Verify follow-up and receipts.
2
Clinician Recruitment and Scheduling Capacity
Clinician Coverage and Slot Readiness
Opening depends on licensed clinicians being live in the schedule before the first patient books. The Year 1 plan shows 10 general practitioners at 450% modeled capacity, 5 mental health counselors at 400%, 8 prescription specialists at 500%, 3 pediatricians at 400%, and 2 dermatologists at 350%. If the license, scope, and hours are not loaded by specialty, the launch slips.
The risk is simple: demand can arrive faster than staffed appointment slots. Published availability with backup coverage is the real readiness signal, because abandoned bookings rise when patients see open slots that can’t actually be filled. Set escalation rules and compensation structure before go-live so day-one care is smooth, not a scramble to rebook.
Publish Coverage Before You Market
Build a live coverage map first: which clinician can treat which state, visit type, and age group, plus who backs them up if a slot drops out. Test one full day of booking against real staffed hours. No backup plan means the calendar looks open, but patients still hit a wall.
- Verify licenses by state.
- Assign specialty scope.
- Set backup coverage hours.
- Document escalation rules.
- Lock pay terms before recruiting.
3
Clinical Workflow and Patient Experience
Patient flow readiness
Opening on time depends on a clean mock visit that proves intake, eligibility screening, consent, visit routing, documentation, e-prescribing boundaries, follow-up, referrals, refunds, and support handoffs all work before go-live. If any step is fuzzy, clinicians lose time, patients get bounced, and first-day visits slip into manual work. A bad intake flow burns the first slot before the chart is even open.
The key dependency is approved protocols plus trained support staff. A pediatric visit must route to a pediatrician, and a prescription renewal must go to a prescription specialist; otherwise, you risk unsafe care or a wasted clinician slot. If routing rules are unclear, you usually pay for it with refunds, escalations, and slower revenue.
Mock every service line
Before launch, map the visit in order: intake, screening, consent, routing, note, prescription decision, follow-up, referral, refund path, and support handoff. Then test each path with a real person on the support side, not just a screen review. The goal is simple: no handoff should depend on guesswork.
- Test pediatric routing first.
- Test prescription renewals separately.
- Write refund triggers in plain language.
- Train support on escalation rules.
- Confirm documentation closes every visit.
One broken intake step can waste a clinician visit and create a patient complaint the same day. Fixing that before opening is cheaper than refunding it after the fact.
4
Payment, Billing, and Revenue Collection
Payment Setup
For day-one launch, the fastest path is self-pay before or at booking. That keeps cash moving, avoids claims setup, and lets the first paid visit happen without waiting on credentialing or partner files. Simple collect first, complex billing later.
At $49–$99 per visit, modeled payment processing at 10% of revenue is about $4.90–$9.90 per visit. Memberships add recurring billing and cancellation rules; employer-paid care needs contracts and eligibility files; payer billing can slow launch through credentialing and claims setup.
Test Cash Flow
Before opening, run one paid test visit end to end: booking, charge, receipt, refund, and reconciliation. The readiness signal is simple — a patient pays, the visit completes, and the books match. Cash at booking keeps day one clean.
- Set one visit price first.
- Document refund and cancellation rules.
- Confirm processor and payout timing.
- Test reconciliation against the ledger.
If any one of those steps fails, opening on time gets risky because staff can’t tell whether a visit really paid, refunded, or settled. That creates messy support work and weak first-week cash flow.
5
Patient Acquisition and First-Booking Engine
First-Booking Engine
A telehealth launch does not really open until a patient can find the booking page, pay, get a reminder, and complete a visit. With 35% of revenue modeled for marketing and acquisition in Year 1, the funnel has to convert fast or you burn cash before you know what works.
Start with one niche, then target high-intent searches and referral channels. If you only buy traffic and do not turn it into scheduled paid consultations, the business has empty clinician time, weak first revenue, and no clear signal on which patients actually book and show up.
Test the Funnel Before Spend
Verify the full path before opening: traffic source, booking page, payment, reminder, and follow-up tracking. The readiness signal is a test patient who books, pays, receives the reminder, and completes the consult with the record captured end to end.
Assign one owner to conversion tracking and one to traffic. Measure booked rate and completed-visit rate from day one. If paid traffic starts before those numbers are visible, you will not know whether the issue is search intent, page design, pricing, or reminders.
- Pick one niche first.
- Use high-intent search terms.
- Test booking and payment.
- Track completed consultations.
- Delay spend until conversion is clear.
6
Related Products
- Online Medical Consultation Porter's Five Forces Analysis
- Online Medical Consultation BCG Matrix
- Online Medical Consultation Business Model Canvas
- 7 Critical KPIs for Online Medical Consultation
- Online Medical Consultation Business Plan Template in Pre-Written Word
- How to Boost Online Medical Consultation Profitability in 7 Steps
- How Much Does It Cost To Run An Online Medical Consultation Platform?
- Online Medical Consultation Startup Costs: $227K CAPEX Plus Cash Runway
- Online Medical Consultation Financial Model Template in Excel
- How Much Online Medical Consultation Owners Make At 1,932 Visits/Month
- How to Write an Online Medical Consultation Business Plan
- Online Medical Consultation Marketing Mix
- Online Medical Consultation Marketing Plan
- Online Medical Consultation Business Proposal
- Online Medical Consultation PESTEL Analysis
- Online Medical Consultation Pitch Deck Example Editable PPTX
- Online Medical Consultation Business SWOT Analysis
- Online Medical Consultation Value Proposition Canvas
Frequently Asked Questions
Yes, but clinical care must be delivered by properly licensed providers in the patient’s state Your launch plan still needs HIPAA-ready systems, malpractice coverage, consent, documentation, and prescribing rules In the researched Year 1 case, the operating model uses 28 clinicians across 5 service lines, so the founder role is more about compliant operations than practicing medicine