 Owner income-$1.0M to $4.1M
Owner income-$1.0M to $4.1MHow Much Does an Orthopedic Clinic Owner Make From $27M Revenue?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income-$1.0M to $4.1M  Net margin-37% to 27%
Net margin-37% to 27% Revenue for target pay$3.5M
Revenue for target pay$3.5M Business difficultyHard
Business difficultyHard


Key Takeaways
- Filled schedules drive revenue more than headline volume.
- Payer mix changes collected cash per visit.
- Fixed overhead falls from 113% to 21% by Year 5.
- Billing fees and denials control cash flow.
Owner income-$1.0M to $4.1MNet margin-37% to 27%Revenue for target pay$3.5MBusiness difficultyHardWant to test your own clinic income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. It excludes personal taxes, legal structure, guaranteed salaries, and one-time startup costs unless you add them.
Want to check owner income in the Orthopedic Clinic model?
The Orthopedic Clinic Financial Model Template shows revenue, margin, costs, reserves, and owner take-home assumptions—open the model.
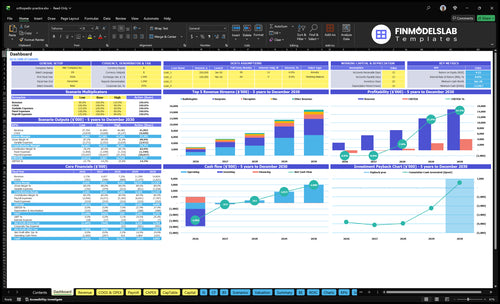
Owner-income model highlights
- Dashboard shows owner pay
- Year 1-5 revenue charts
- Scenario testing by payer mix
- Staffing and cost tabs
- Fixed overhead and inputs
Which orthopedic clinic costs cut owner take-home most?
The costs that cut owner take-home most are the fixed bills before distributions: $15k lease and $15k maintenance are the biggest drain, and if you’re mapping startup costs, How Much Does It Cost To Open An Orthopedic Clinic? shows how fast they stack up. Add $5k malpractice, $2k utilities, and $1k EHR, and visible fixed costs hit at least $38k a month before variable spend. Variable costs run at 18% of revenue, and one visible surgeon salary is $350k a year, so every cost dollar paid before distributions lowers owner take-home unless it raises collections or capacity.
Big fixed costs
- $15k monthly lease
- $15k monthly maintenance
- $5k monthly malpractice
- $2k monthly utilities
Labor and variable spend
- $1k monthly EHR software
- Variable costs are 18% of revenue
- One surgeon salary is $350k yearly
- Payroll data is incomplete here
How do orthopedic clinics make money?
Orthopedic clinics make money by billing completed visits, procedures, imaging, therapy, and nurse-led services; in this Orthopedic Clinic model, radiology is the largest listed Year 1 revenue stream, so What Is The Most Important Metric To Measure The Success Of Your Orthopedic Clinic? should tie revenue back to capacity, utilization, and payer mix. One data issue matters: $115M radiology conflicts with the stated 42% share, so validate that figure before using it for funding or staffing decisions.
Main Revenue
- Surgeon treatments: $864k
- Physician assistants: $216k
- Radiology: $115M listed
- Therapists: $324k
What Controls Profit
- Nurse-led services: $180k
- Payer contracts set allowed rates
- Ownership rules limit ancillaries
- Compliance controls procedure capture
How does clinic scale change orthopedic owner income?
For an Orthopedic Clinic, scaling from 15 clinical staff in Year 1 to 34 in Year 5 can lift owner income potential because modeled revenue rises from $274M to $1,482M as capacity moves from 60% to 80%. The fixed overhead stays at $3,096k a year, so it falls from 113% of revenue in Year 1 to 21% in Year 5; that’s the upside, but scale also brings more payroll risk, utilization pressure, management load, compliance needs, and working-capital needs.
Income upside
- 15 to 34 staff growth
- $274M to $1,482M revenue
- 60% to 80% capacity
- Fixed overhead stays at $3,096k
Scale risks
- Payroll risk rises with more staff
- Utilization gets harder to hold
- Management load increases fast
- Compliance and cash needs grow
What drives orthopedic clinic owner income?
1
$274M-$1.48BProvider Volume
More surgeon, PA, radiology, and therapy work lifts revenue fast, so this is the biggest driver of owner cash.
2
18%Payer Mix
Better contract rates and fewer denials protect the cash left after the 18% variable cost load.
3
$150-$4KService Mix
A richer mix of surgery, imaging, and rehab raises revenue per visit, while low-value care drags margin.
4
60%-80%Staffing Efficiency
Moving capacity from 60% to 80% spreads wages across more billable work and improves EBITDA.
5
$25.8K/moFixed Overhead
The clinic carries about $25.8K in fixed overhead each month, so idle rooms still burn cash.
6
5%Billing Speed
Billing services take 5% of revenue, and faster claims work keeps more cash in house.
Orthopedic Clinic Core Six Income Drivers
Provider Productivity And Patient Throughput
Provider Productivity
Income here comes from how well the clinic turns provider time into billable care. In this model, capacity rises from 60% in Year 1 to 80% in Year 5, with monthly treatments rising from 15 to 19 per surgeon, 25 to 29 per physician assistant, 200 to 240 per radiologist, 100 to 120 per therapist, and 50 to 58 per nurse.
The risk is simple: more visits do not always mean more owner income. If referrals slow, no-shows rise, staffing slips, or collections lag, the clinic can fill slots but miss cash. This driver moves revenue, labor cost, and cash flow at the same time, so profit depends on turning each open slot into a paid visit.
Keep Schedules Full
Track filled schedule rate, referral flow, no-show rate, and treatments per provider by role each month. Use booked, kept, and billed visits together, not just appointment volume. That shows whether growth is real demand or just empty capacity on the calendar.
Push volume only when reimbursement, staffing, and collections can absorb it. If a provider adds visits but billing lags or payroll rises faster than cash, owner pay gets squeezed. The clean test is whether each extra treatment improves net cash after labor and billing costs, not just top-line revenue.
1
Payer Mix And Reimbursement Quality
Payer Mix Quality
Payer mix is the share of visits and procedures paid by commercial insurance, Medicare, Medicaid, workers’ compensation, and cash pay. In this clinic, prices range from $100 nurse services to $4,800 surgeon treatments by Year 5, so payor shifts change cash collected fast. A 1% collection swing equals about $274k in Year 1 revenue and $1,482k in Year 5 revenue.
What this hides is the gap between billed work and cash in hand. Deductibles, denials, and contract terms can cut owner pay even when visit volume is steady. If collections slip, fixed costs still get paid first, so the owner feels the hit in lower profit and tighter cash flow.
Track Net Collections
Watch net collection rate first: cash collected after contractual write-offs and denials. Then split it by payer, service type, and provider so you can see where revenue leaks start. The key inputs are visit counts, procedure mix, allowed rates, deductibles collected, denial rate, and days to cash.
- Track cash by payer each month.
- Flag denials before aging starts.
- Compare allowed rates by contract.
- Measure patient balance collection speed.
If cash collection improves by just 1%, the owner keeps far more income without adding visits. If payer mix shifts toward lower-paying contracts or uncollected balances rise, the clinic can look busy and still pay out less.
2
Procedure And Ancillary Service Mix
Procedure and Ancillary Mix
Service mix changes both revenue and margin because each service line pays and costs differently. In the Year 1 model, revenue includes $864k surgeon treatments, $324k therapy, $216k physician assistant services, and $180k nurse services, while imaging is about 42% of total revenue. If the mix shifts toward lower-paid or higher-cost work, owner take-home falls even when visit counts stay flat.
Track Margin by Service Line
Measure revenue, labor, supplies, denials, and collections by injections, casting, imaging, therapy, DME, and surgery-related cases. Here’s the quick math: a better mix lifts gross margin, but a worse mix can add staffing and compliance cost faster than cash comes in. Before you count on the revenue, review payer contracts and compliance rules so the captured margin matches the billed work.
3
Staffing Efficiency And Provider Leverage
Provider Leverage
Provider leverage is how many visits, procedures, and collections each clinician supports before payroll starts outrunning revenue. Here, staffing grows from 2 surgeons, 4 physician assistants, 1 radiologist, 3 therapists, and 5 nurses in Year 1 to 6 surgeons, 8 physician assistants, 3 radiologists, 7 therapists, and 10 nurses in Year 5, while a surgeon’s visible salary is $350k a year. If schedules are thin, this fixed labor load cuts operating margin and owner pay fast.
The risk is blunt cuts. The full payroll is incomplete, so the real test is revenue and collections per provider, not headcount alone. If staffing drops below demand, visits fall, wait times rise, patient experience slips, and collections can weaken. For an orthopedic clinic, the win is matching labor to filled capacity, not just to planned capacity.
Track staff per booked visit
Measure booked visits, completed visits, and collections per clinician each month. Compare labor load as the team scales from Year 1 to Year 5, and flag any role whose added payroll does not lift throughput or cash collected.
Use a simple rule: if a hire does not improve filled schedules, patient flow, or collections, it is overhead, not leverage. Track surgeon time, PA support, radiology volume, therapy sessions, and nurse coverage together so cuts do not break care delivery.
Facility, Equipment, And Fixed Overhead
Facility and Fixed Overhead
Fixed overhead is the monthly cost stack that shows up before owner pay: lease, malpractice insurance, utilities, maintenance, and EHR software. Here that is $258k per month or $3,096k per year, including a $180k lease, $60k malpractice, $24k utilities, $18k maintenance, and $12k software. With low volume, these costs can wipe out income fast.
The key inputs are utilization, visit volume, and collected revenue per treatment. As volume rises, fixed overhead drops from 113% of revenue in Year 1 to 21% in Year 5, so the clinic’s owner income depends on filling the facility enough to spread these costs. If utilization slips, cash flow tightens and owner draw gets pushed out.
Track Overhead Against Collected Revenue
Measure fixed overhead as a share of monthly collections, not just as a dollar total. Watch lease, insurance, utilities, maintenance, and software every month, then compare that run rate with treatment volume and collection pace. If the ratio stays near the 113% Year 1 level, the clinic is still funding overhead before it earns owner pay.
Manage this driver by keeping rooms, equipment, and provider time busy enough to spread the fixed base. One cl ean rule: if volume growth stalls, overhead does not shrink with it. Build the forecast around monthly utilization and collections, then test whether each added treatment actually lowers fixed overhead per dollar of revenue.
5
Billing, Collections, Denials, And Cash Flow
Revenue-Cycle Cash Control
This driver controls how much billed orthopedic work turns into cash. In this model, billing services run at 5% of revenue, or about $1,368k in Year 1 and $7,412k in Year 5, so slow claims, denials, or unpaid patient balances can cut owner draw even when volume is strong.
The cash risk is timing and collectability, not just price. Coding accuracy, prior authorizations, denial follow-up, patient balances, collection lag, and billing fees all affect how fast money reaches the bank. If collections slip, profit on paper can look fine while cash for payroll, rent, and owner pay gets tight.
Speed Up Claim-to-Cash
Track clean-claim rate, denial rate, prior auth turnaround, patient balance aging, and days from service to cash. Keep the billing team on a weekly denial list and a set follow-up cadence, because every delayed appeal or patient bill delays cash for the business owner.
Use the 5% billing cost line as a control point, not a guess. If billing fees stay fixed while denials fall, more revenue drops to cash and less gets trapped in receivables. If collection lag rises, raise reserves before taking distributions.
6
Compare lean, base, and high orthopedic clinic income cases
Owner income scenarios
Income swings hard with clinic scale because staff, capacity, and fixed overhead move together. These cases show the planning range before payroll details are fully set.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | This is the lower earnings path if the clinic stays near Year 1 scale and collections are still uneven. | This is the modeled middle path if the clinic reaches Year 3 scale and runs close to plan. | This is the stronger earnings path if the clinic reaches Year 5 scale and holds higher utilization. |
| Typical setup | Year 1 scale: 15 clinical staff, 60% capacity, $274M revenue, 18% variable costs, and about $3.096M fixed overhead before debt, reserves, taxes, or owner pay; payroll data is incomplete. | Year 3 scale: 24 clinical staff, 70% capacity, $733M revenue, and about $570M pre-payroll cash before debt, reserves, taxes, and owner pay; payroll data is incomplete. | Year 5 scale: 34 clinical staff, 80% capacity, $1.482B revenue, and about $1.185B pre-payroll cash before debt, reserves, taxes, and owner pay; payroll data is incomplete. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $193M pre-payroll cashLow Case | about $570M pre-payroll cashBase Case | about $1.185B pre-payroll cashHigh Case |
| Best fit | Use this to stress-test the clinic if volume or collections come in below plan. | Use this as the planning case for lender, investor, and board work. | Use this to test upside if referrals stay strong and the clinic keeps scaling smoothly. |
Planning note: Scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Orthopedic Clinic Porter's Five Forces Analysis
- Orthopedic Clinic BCG Matrix
- Orthopedic Clinic Business Model Canvas
- 7 Critical KPIs to Measure for Orthopedic Clinic Success
- Orthopedic Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Orthopedic Clinic Profitability
- How To Calculate Monthly Running Costs for an Orthopedic Clinic
- Orthopedic Clinic Startup Costs: Plan For $215M+ In CAPEX
- Orthopedic Clinic Financial Model Template in Excel
- How To Open An Orthopedic Clinic In The US In 6 To 12 Months
- How to Write an Orthopedic Clinic Business Plan: 7 Actionable Steps
- Orthopedic Clinic Marketing Mix
- Orthopedic Clinic Marketing Plan
- Orthopedic Clinic Business Proposal
- Orthopedic Clinic PESTEL Analysis
- Orthopedic Clinic Pitch Deck Example Editable PPTX
- Orthopedic Clinic Business SWOT Analysis
- Orthopedic Clinic Value Proposition Canvas
Frequently Asked Questions
Owner take-home depends on what remains after payroll, debt, reserves, and reinvestment The model shows $274M in Year 1 revenue, $1482M in Year 5 revenue, 18% variable costs, and $3096k annual fixed overhead before payroll That creates planning capacity, not guaranteed personal income