 Owner income$120k-$186k
Owner income$120k-$186kHow Much Does An Outpatient Clinic Owner Make On $897K Revenue?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$120k-$186k  Net margin7% to 66%
Net margin7% to 66% Revenue for target pay$1.6M
Revenue for target pay$1.6M Business difficultyHard
Business difficultyHard


This guide estimates outpatient clinic owner take-home across a five-year model, starting with $897,000 in first-year collected revenue It covers patient volume, reimbursement, provider mix, listed payroll, overhead, variable costs, reserves, and owner role It does not give a guaranteed salary, physician pay benchmark, tax advice, or legal advice
Owner income$120k-$186kNet margin7% to 66%Revenue for target pay$1.6MBusiness difficultyHardWant to test your outpatient clinic owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only, not guaranteed salary, tax advice, or owner distribution advice.
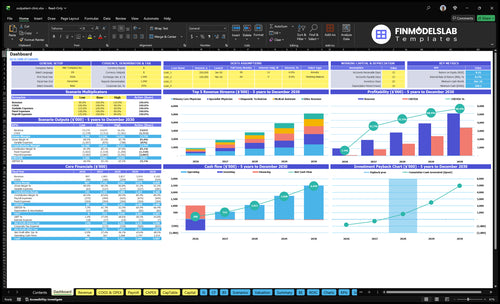
Want to check owner income in the Outpatient Clinic model?
This scenario view, not a promise, shows revenue, EBITDA-style profit, owner pay, cash reserve, and break-even charts; open the Outpatient Clinic Financial Model Template.
Owner-income model highlights
- $897k Year 1 revenue
- $510M mature-year revenue
- Provider, treatment, price tabs
- Payroll, overhead, cost tabs
- Debt, reserves, distribution tabs
- 65% to 90% capacity
- 17% to 14% costs
How much revenue does an outpatient clinic need to pay the owner?
Use collected revenue, not billed charges. In the Year 1 model, the outpatient clinic has $897k in revenue; after 17% COGS plus variable costs, $3,036k fixed overhead, and $325k listed admin payroll, the quick math shows about $116k operating profit. So the clinic can support a $120k owner-manager salary only if collections cover payroll first and cash reserves are built.
Pay the owner
- Use collected revenue, not billed charges.
- $897k is the Year 1 base.
- About $116k stays after costs.
- $120k owner pay is tight.
Protect cash
- Cover payroll before owner pay.
- Target $524k in reserve cash.
- That covers one month of overhead.
- Track collections every month.
Is owning an outpatient clinic profitable?
Yes—an Outpatient Clinic can be profitable under the researched assumptions, but scale does not guarantee profit. In the base staffed case, Year 1 revenue is $897k and operating profit is about $116k after listed costs. A lean owner-operated case can work too, but only if the owner covers management work and keeps fixed costs tight; at higher volume, the model shows $510M revenue at 90% capacity with 5 primary care physicians, 4 specialists, 3 diagnostic technicians, 3 procedure nurses, and 6 medical assistants. The real risks are utilization, compliance, staffing gaps, payer reimbursement, denials, and cash reserves.
Profit drivers
- Keep utilization high.
- Hold fixed costs down.
- Use fee-for-service throughput.
- Owner absorbs management work.
Key risks
- Low patient volume.
- Compliance mistakes.
- Staffing gaps.
- Reimbursement and denial pressure.
What outpatient clinic profit margin should an owner watch?
For an Outpatient Clinic, watch take-home cash, not just accounting margin. Year 1 modeled operating margin is 129% after the listed costs, but the $253k/month fixed overhead means empty rooms still hurt cash flow. For startup cost context, see What Is The Estimated Cost To Open And Launch Your Outpatient Clinic Business?
Cash margin drivers
- 17% COGS and variable costs start high
- They fall to 14% in the mature year
- $3k monthly malpractice coverage adds drag
- $12k monthly software also cuts cash
Cash outflow watchlist
- Staffing hits distributable cash first
- Billing labor and denials reduce collections
- Supplies and marketing stay variable
- Underused rooms slow early cash flow
Want the six outpatient clinic income drivers?
1
65%-90%Visit Volume
More visits set the revenue ceiling, and 65% to 90% capacity decides how hard fixed costs work for you.
2
$120-$290Payer Mix
Better payer mix lifts collected dollars per visit, so the same schedule can yield a lot more cash.
3
$19K-$29KProvider Output
Higher throughput lets each clinician spread labor across more billable work, which protects margin.
4
$50-$290Service Mix
More specialist and procedure visits push the average ticket up, while routine care keeps the base full.
5
14%-17%Revenue Cycle
Cleaner coding and faster collections keep earned revenue from getting stuck in denials or aged receivables.
6
$253K/moFixed Overhead
About $253K in monthly fixed overhead has to be covered before the clinic can pay owners and rebuild reserves.
Outpatient Clinic Core Six Income Drivers
Patient Visit Volume And Capacity
Visit Volume and Capacity
Volume sets the income ceiling. In this model, the clinic runs at 65% capacity in Year 1 and produces $748k monthly revenue; mature-year capacity reaches 90% and $4,252k monthly revenue. That gap is the owner’s upside, but only if each added visit still covers provider time, supplies, billing cost, and exam room use.
Track visits per provider per month, operating days, no-show rate, appointment length, and room turnover. Here’s the quick math: if visits rise faster than staffing or patient flow, revenue can climb while profit and owner pay slip. One clean rule: don’t add slots unless reimbursement and capacity both support them.
Track Capacity Weekly
Measure the full funnel, not just booked slots. Use booked visits, completed visits, no-shows, exam room utilization, and hours worked per provider to see real capacity. A full schedule that is slow, under-staffed, or badly mixed can still hurt cash flow if overtime, rework, or delays eat the margin.
- Watch visits per provider monthly.
- Track no-shows by service type.
- Limit slot length drift.
- Match rooms to staffing.
If onboarding lags or patient flow breaks, the clinic can miss revenue while fixed overhead keeps running, which cuts the cash available for owner distributions.
1
Payer Mix And Net Reimbursement
Payer Mix And Net Reimbursement
Payer mix is the share of visits paid by commercial insurance, Medicare, Medicaid, cash pay, and patient deductibles. In an outpatient clinic, it drives cash per visit because billed charges are not the same as allowed amounts or actual collections. A mature-year service can range from $50 for medical assistant work to $290 for specialist physician services.
One clean line: the payer mix decides how much of each visit turns into cash. If balances age, eligibility is missed, or reimbursement does not cover the service cost, owner take-home falls even when visit volume looks fine. That is why a full schedule can still produce weak distributions.
Track Net Reimbursement By Payer
Measure allowed amount, actual cash collected, and days in accounts receivable by payer and service type. Compare each visit to the mature-year price range of $50 to $290, then check what really lands in cash. That shows which services support owner pay and which ones only look good on paper.
Watch eligibility checks, deductible exposure, and patient balance aging every week. If a payer mix or service line does not cover labor, supplies, and billing cost, adjust the schedule, tighten collections, or shift more visits toward better-paying payers before distributions get squeezed.
- Track cash by payer class.
- Separate billed and collected amounts.
- Flag aged balances fast.
- Review underpaid services monthly.
2
Provider Productivity And Staffing Leverage
Provider Utilization
Provider utilization is the share of paid clinical time spent on billable visits and procedures. In Year 1, staffing is 2 primary care physicians, 1 specialist physician, 1 diagnostic technician, 1 minor procedure nurse, and 2 medical assistants; the mature year scales to 5, 4, 3, 3, and 6. Moving utilization from 65% to 90% lifts capacity without a matching jump in labor, so labor cost per visit falls and more cash can reach the owner.
Lower staffing is not automatically better. If schedules get too tight, compliance slips, notes lag, and burnout rises, which can hurt patient experience and clinical quality. The real limit is the point where more booked time starts slowing documentation, follow-up, or safe care.
Measure and Protect Capacity
Track visits per provider per day, appointment length, no-show rate, room turns, and documentation time. Use those inputs to test whether the clinic can hold near 90% capacity without overtime or quality drift. If utilization stays near 65%, the owner pays for idle labor; if it runs too hot, missed follow-up and burnout can erase the gain.
- Review schedule fill daily.
- Watch note lag weekly.
- Cap overbooked slots.
- Match staffing to service mix.
3
Service Mix And Ancillary Revenue
Service Mix and Margin
An outpatient clinic’s income changes with service mix because not every visit pays the same. Year 1 prices are $120 primary care, $180 diagnostics, $250 specialist visits, $150 minor procedures, and $50 medical assistant services; mature-year prices rise to $140, $210, $290, $175, and $60. That is about a 17% to 20% price lift.
Here’s the catch: add-ons like diagnostics, lab-related services, procedures, preventive care, chronic care, and specialty visits can lift revenue, but supplies, reagents, referrals, coding, and payer rules take a bite out of it. The owner only wins if the mix improves gross margin per visit, not just billed revenue.
Track Margin by Service Line
Measure each service by volume, price, direct cost, and net collections. The key input is not total visits alone; it is the share of visits in higher-margin services and the cost to deliver them. If a $180 diagnostic or $250 specialist visit needs heavy supplies or extra coding work, the margin can shrink fast.
Use service-level reporting to see which visits create cash after staff time, reagents, and payer write-offs. Then push scheduling toward the services that leave the best net margin, and drop add-ons that add work but no profit. That is what helps fund owner pay.
4
Billing, Denials, And Collections
Billing, Denials, And Collections
Billing, denials, and collections decide how much of each visit becomes cash. In this clinic, weak eligibility checks, prior auth misses, bad coding, or slow denial follow-up can delay owner pay even when revenue looks fine on paper. The key gauges are clean claim rate, denial rate, net collection rate, days in accounts receivable, and billing cost per visit.
The model starts with one Billing Specialist at $55k in Year 1 and scales to 20 FTE by Year 3, so billing payroll becomes a real margin line, not just admin noise. Here’s the quick math: if claims sit in A/R or get denied, cash lags while wages, supplies, and other costs still leave the bank. That can shrink distributions fast.
Track Cash, Not Just Charges
Measure the full revenue cycle from visit to deposit. A net collection rate is the share of allowed revenue actually collected, so it shows how much billable work turns into spendable cash. Track eligibility checks, prior auth, coding accuracy, denial reasons, appeal turnaround, patient balance collection, and billing cost per visit by payer and service type.
- Watch clean claims on first pass.
- Follow denials within 48 hours.
- Age patient balances by 30 days.
- Link billing cost to visit volume.
If days in A/R rises, cash gets stuck and owner draws slip. If patient balances age, collections fall even when clinical volume is strong. The fastest fix is tighter front-end checks, cleaner coding, and same-week denial work, because each step protects the cash conversion of every visit.
5
Fixed Overhead And Cash Reserves
Fixed Overhead Eats Owner Pay
Fixed overhead is the monthly bill that gets paid before the owner does. In this clinic, source fixed costs total $253k per month, including $15k lease, $3k professional liability insurance, $25k utilities and internet, $18k maintenance and cleaning, and $12k software, so every empty slot cuts distributable income fast.
Here’s the quick math: Year 1 fixed overhead plus listed admin payroll is about $524k per month. That means cash has to cover rent, insurance, software, and staff before any owner draw. If volume lags, profit can look fine on paper but cash still gets tight, especially when commitments are locked in ahead of patient demand.
Separate Reserves Before Owner Draw
Track fixed cost coverage, monthly cash reserve, and owner draw as three separate buckets. A clean rule is to hold reserves first, reinvest second, and only then pay the owner. Do not treat retained cash as spendable profit; it is the buffer that keeps the clinic open when visits dip or collections slow.
Watch the biggest fixed items every month: lease, insurance, utilities, cleaning, software, and admin payroll. If you sign space or equipment too early, overhead stays high while volume fills slowly. A simple control is to compare committed fixed costs to booked patient volume each month, then delay new contracts until the schedule supports them.
- Track monthly fixed cost runway.
- Ring-fence reserves from owner pay.
- Review lease and equipment commitments.
- Match overhead to booked visits.
6
Compare lean, base, and high-volume outpatient clinic income scenarios
Owner income scenarios
Owner income swings with visit volume, capacity, and staffing because lease and payroll stay fixed. These cases show what reaches the owner at lower, modeled, and stronger operating levels.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | Lower capacity and tighter staffing keep owner income near break-even. | The modeled Year 1 plan supports modest owner income after fixed costs. | Stronger utilization and pricing can lift owner income sharply in the mature year. |
| Typical setup | Lower visit volume, owner-manager coverage, and the smallest safe support team keep distributions tight. | Year 1 runs at 65% capacity with about $897k revenue, a 17% variable and COGS load, and $325k admin payroll. | The mature model runs at 90% capacity with about $5.1M revenue, a 14% variable and COGS load, and higher admin payroll. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $0 - $66kLow Case | $116kBase Case | $3.4MHigh Case |
| Best fit | Use this to test owner pay when demand stays soft and the clinic runs with limited distributions. | Use this as the main operating plan for Year 1 cash needs and owner income. | Use this to test upside if the clinic runs near target capacity and keeps costs on model. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Outpatient Clinic Porter's Five Forces Analysis
- Outpatient Clinic BCG Matrix
- Outpatient Clinic Business Model Canvas
- 7 Essential KPIs to Track for Your Outpatient Clinic
- Outpatient Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Outpatient Clinic Profitability and Margin
- Analyzing the Monthly Running Costs for an Outpatient Clinic
- Outpatient Clinic Startup Costs: $815K CAPEX Plus Cash Reserve
- Outpatient Clinic Financial Model Template in Excel
- How to Open an Outpatient Clinic: 6–12 Month Launch Roadmap
- How to Write an Outpatient Clinic Business Plan: 7 Action Steps
- Outpatient Clinic Marketing Mix
- Outpatient Clinic Marketing Plan
- Outpatient Clinic Business Proposal
- Outpatient Clinic PESTEL Analysis
- Outpatient Clinic Pitch Deck Example Editable PPTX
- Outpatient Clinic Business SWOT Analysis
- Outpatient Clinic Value Proposition Canvas
Frequently Asked Questions
A managing owner may use the modeled $120,000 Clinic Director salary if they actually run operations Distributions are separate and should come from profit after reserves, debt service, taxes, reinvestment, and clinical provider pay In the first year, modeled operating profit after listed costs is about $116,000 on $897,000 revenue