 Time to Open8-12 weeksLaunch runway
Time to Open8-12 weeksLaunch runwayHow To Open An Overdose Prevention Program In 8 To 16 Weeks

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open8-12 weeksLaunch runway  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckAuthorization gateState rules
Key BottleneckAuthorization gateState rules First Revenue StepPaid cohortTraining live
First Revenue StepPaid cohortTraining live


Key Takeaways
- Authority and protocols must be signed before launch.
- Naloxone supply and training capacity set day-one volume.
- Partner referrals drive attendance, trust, and event flow.
- Funding and reporting protect runway, renewals, and credibility.
Time to Open8-12 weeksLaunch runwayLaunch Sequence6 stagesCompliance firstKey BottleneckAuthorization gateState rulesFirst Revenue StepPaid cohortTraining liveLaunch timeline
This short web timeline summarizes the launch plan, and the XLSX export contains the detailed Gantt chart.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Compliance / protocols
- Review standing order
- Confirm insurance coverage
- Draft clinical protocols
- Complete privacy review
Naloxone supply
- Set supplier terms
- Place naloxone order
- Build stock controls
- Set reorder trigger
Training / curriculum
- Finalize curriculum outline
- Prepare instructor scripts
- Train lead instructors
- Run pilot sessions
Partner outreach
- Map partner sites
- Confirm referral flow
- Book first groups
- Set outreach calendar
Data systems
- Configure CRM
- Build scheduling forms
- Set reporting fields
- Test privacy access
Launch / events
- Create launch message
- Recruit event staff
- Publish outreach calendar
- Run first event
Why test the launch plan before hiring or ordering supplies?
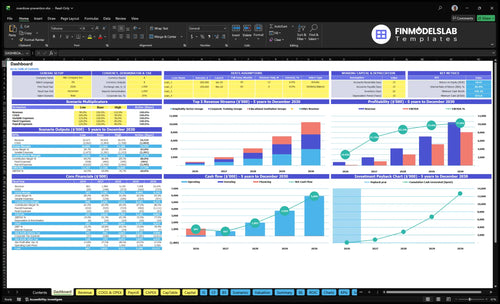
This Overdose Prevention Program Financial Model Template shows launch timing, revenue, costs, cash needs, assumptions, and breakeven—open it before hiring.
Financial model highlights
- Revenue: $861k to $10.476M
- EBITDA: $172k to $8.067M
- Month 2 breakeven
- 9-month payback
- Cash runway, staffing, supplies
How do you get first funding for an overdose prevention program?
If you’re trying to fund an Overdose Prevention Program, start with paid contracts and funded pilots, not just grants. The fastest first dollar is a signed training agreement or one funded pilot, because grant timing can lag operating readiness; for example, Year 1 pricing can be How Increase Overdose Prevention Program Profits? at $1,200 for corporate groups, $900 for educational groups, and $1,000 for hospitality groups.
First funding paths
- Local health department contracts
- County opioid settlement-funded pilots
- Nonprofit grants
- Employer training
Year 1 sales mix
- 15 corporate groups at $1,200 = $18,000
- 10 educational groups at $900 = $9,000
- 20 hospitality groups at $1,000 = $20,000
- Total Year 1 training revenue: $47,000
What are common mistakes starting an overdose prevention program?
Most launch mistakes are preventable: don’t hand out naloxone before protocols are approved, train staff before the documentation is ready, or announce events before supply is confirmed. A go or no-go readiness review should check supplier access, a reorder point, a referral path, privacy controls, and grant reporting before public rollout.
Launch gaps
- Do not distribute before protocols are approved.
- Do not train before documentation is ready.
- Do not announce before naloxone is on hand.
- Do not skip privacy controls.
Run checks
- Use CRM and scheduling software at $450 per month.
- Track groups, attendance, referrals, follow-up.
- Validate staffing against 18 billable days per month.
- Test 45% Year 1 occupancy before launch.
How long does it take to start an overdose prevention program?
An Overdose Prevention Program usually takes 8 to 16 weeks to launch. The pace depends on state rules, standing order setup, naloxone supplier approval, educator training, partner site agreements, outreach calendar, and reporting tools. Month 1 covers staff, office, CRM, insurance, supplier process, curriculum, and equipment, and paid group training can start once documentation is ready.
Launch timing
- 8 to 16 weeks is the practical range
- State rules can slow approval
- Supplier approval adds lead time
- Untested reporting creates delays
Setup work
- Month 1: staff and office setup
- Month 1: CRM, insurance, supplier process
- Month 6: curriculum development continues
- Month 12: mobile training vehicle launch
Check whether the program is ready to distribute naloxone and teach overdose prevention
Launch readiness checklist
Use this go-live approval checklist to confirm the program is ready before opening.
Authority
- Naloxone authority confirmedCritical
State authority must be in place before any kit handoff or class starts.
- Medical oversight signedCritical
Standing order or medical oversight sets who can approve use and training.
- Liability insurance boundHigh
Insurance should be active before staff meet clients or store inventory.
Supply
- Supplier contract signedCritical
A signed supplier keeps naloxone kits flowing after launch.
- Kit storage securedHigh
Secure storage protects kits, supplies, and expired stock.
- Expiration logs readyHigh
Inventory logs make expiration tracking and refills visible.
- Reorder points setMedium
Reorder points stop stockouts when demand spikes.
Curriculum
- Curriculum approvedCritical
Approved curriculum keeps education consistent across sites.
- Demo devices availableHigh
Demo devices make overdose response practice hands-on.
- Training logs readyHigh
Training logs prove staff completed the right steps.
Partners
- Health department partner readyHigh
Health department ties build trust and referrals.
- Shelter referral path liveHigh
Shelters can send high-risk clients to you fast.
- Clinic contacts setHigh
Clinic contacts keep intake and follow-up moving.
Staffing
- Program director assignedCritical
The director owns approvals, QA, and escalation.
- Lead instructors scheduledHigh
Lead instructors cover classes and refreshers.
- Sales account manager assignedHigh
Sales account coverage keeps partner outreach moving.
- Administrative coordinator hiredHigh
Admin coverage keeps scheduling and records current.
Runway
- Billable days match modelCritical
The model assumes 18 billable days and 45% occupancy in Year 1.
- Occupancy target checkedHigh
Occupancy must build from 45% in Year 1 toward the plan.
- Procurement ratios match modelHigh
Check 8% naloxone procurement and 3% training supplies.
- Month 2 cash above $873kCritical
Month 2 cash must stay above $873,000 at the low point.
- Go-live signoff completeCritical
Go-live signoff should wait until every gate is green.
Which launch drivers matter most before opening?
1Legal Authority
Launch gateWithout written authority and protocols, the program can't safely distribute naloxone or open events.
2Naloxone Supply
Supply gateApproved supply and stock tracking prevent stockouts and keep launch trainings on schedule.
3Training Team
20 FTETrained instructors and approved materials keep day-one education consistent and defensible.
4Partner Network
Partner sitesSigned sites and referral paths fill events and make launch attendance more predictable.
5Funding Pipeline
$873KCommitted grants and contracts protect runway before revenue turns positive.
6Data Controls
CRM readyClean reporting protects privacy, supports renewals, and catches outreach misses fast.
Legal Authority And Protocols
Legal Authority and Protocols
Launch is binary here: if the program cannot prove authority to distribute, it cannot safely open. For an overdose prevention program, that means a written state-specific review, a standing order or medical oversight if required, approved overdose-prevention protocols, training records, and insurance in place before the first event.
The bottleneck is opening under unclear authority. One Program Director should own sign-off, while the team confirms state naloxone laws, eligible distributors, participant materials, storage and reporting rules, and staff training. If any one of those is missing, day-one distribution stops, partner onboarding gets slower, and compliance risk jumps.
Confirm authority before scheduling training
Build the approval pack first: legal review, distribution authority, protocol sign-off, participant handouts, storage rules, reporting rules, and staff training documentation. That keeps the launch sequence real. One clean rule: no signed authority, no live event.
Use a short go/no-go checklist before each site visit. Verify state naloxone law, who may distribute, who oversees the program, and how records will be stored. If approval slips by even 1 event, you delay first revenue, waste staff time, and risk a bad first partner experience.
- Confirm state naloxone law.
- Lock legal oversight.
- Approve participant materials.
- Document storage and reporting.
- Train staff on protocol.
1
Naloxone Supply Chain
Naloxone Kit Supply Readiness
If you don’t have kits on site, you can’t start training or hand off a real readiness signal. This driver is direct capacity control: the launch works only when you have an approved supplier, a kit assembly process, a storage plan, expiration tracking, a reorder point, and a distribution log.
The cost load is real but predictable. The source assumption uses naloxone kit bulk procurement at 8% of revenue in Year 1, or about $68,880 on $861,000 of modeled Year 1 revenue, then 6% by Year 5. A supplier delay or stockout can cancel events, slow partner onboarding, and weaken day-one credibility.
Set the supply gate before the first event
Before launch, forecast kits by event, check bulk procurement terms, define the storage owner, and set replenishment triggers. Track lot and expiration where required, because missing inventory control can turn a booked training into a canceled one. One stockout can stop the event, so the supply plan has to work before the first client date.
- Forecast kits by event.
- Assign one storage owner.
- Track lot and expiration.
- Set reorder triggers early.
- Log every distribution.
2
Training Curriculum And Educators
Instructor Readiness
If the instructors are not trained and the session tools are not approved, the program can’t open cleanly on day one. This driver is the service itself: scripted teaching, hands-on demos, and proof that every class was delivered the same way.
The staffing load is heavy: 20 Lead Instructor FTE at $75,000 each implies about $1.5 million in annual payroll. Manuals and supplies are modeled at 3% of Year 1 revenue. If scripts, handouts, demo devices, or attendance logs slip, partner trust drops fast.
Lock the session kit
Build one approved curriculum before you sell dates. Train instructors on overdose recognition, naloxone administration, and what proof must be saved after each class. Keep the same script, handouts, demo flow, and quality check for every site so the first events feel consistent and ready.
- Approved scripts
- Participant handouts
- Demo devices
- Attendance logs
- Completion records
Here’s the quick operating check: every booked session needs a trained Lead Instructor, supplies on hand, attendance captured, and a same-day quality review. Block any event that lacks documentation. If it can’t be proved, it didn’t happen.
3
Community Partnerships And Referrals
Community Partnerships and Referrals
This driver decides whether the program has real access on day one. Without signed or confirmed partner sites and a clear referral workflow, training can be ready but attendance stays weak, so opening looks active on paper and empty in practice.
The launch risk is handoff, not outreach volume. Health departments, shelters, libraries, clinics, recovery organizations, syringe service programs, first responders, and community groups need to know who books events, where naloxone can be distributed, and how referrals move after training. If that path is unclear, trust drops and first events get delayed.
Lock the partner handoff
Before opening, map each partner’s role, confirm distribution rules, and write the referral step down. Train site contacts on who to call, how to book, and what to say so the first sessions do not depend on memory or one person’s follow-up.
- Confirm partner sites in writing.
- Schedule the first events now.
- Assign one owner per site.
Treat warm introductions as launch inventory. If a site is not confirmed, the program can miss attendance even when training and supply are ready, so keep a live event calendar and a simple handoff sheet for every partner.
4
Funding And Contract Pipeline
Signed Funding First
This launch only works if cash is already committed. Grants, contracts, paid training agreements, funded pilots, donations, or sponsored events cover staff, supplies, outreach, and reporting before the first training date. Without that, you risk hiring early and missing day-one delivery.
The pricing plan is clear: $1,200 corporate, $900 educational, and $1,000 hospitality for Year 1 paid groups. With $861,000 modeled Year 1 revenue and Month 2 breakeven, the real bottleneck is timing signed money ahead of scale-up tasks.
Verify funding before staffing
Start with a live pipeline, not a staffing plan. Confirm which accounts are already warm: health departments, county opioid settlement-funded pilots, employers, shelters, schools, hospitality groups, and treatment centers. Then map each deal to a funding source, start date, and deliverable so the opening date matches the money.
- Get written commitment before hiring.
- Match scope to funder timing.
- Separate outreach from scale-up costs.
- Track signed value by launch month.
One clean rule: no committed cash, no expanded schedule. That keeps runway controlled and avoids the common trap of adding instructors before the first paid events are locked.
5
Data Reporting And Risk Controls
Data Reporting And Risk Controls
When you open this program, funders and partners will want proof fast. The launch risk is not the training itself; it’s whether you can show participant counts, kits distributed, trainings delivered, and referrals made from day one, with privacy controls in place.
That reporting setup also protects renewals. If overdose reversals are reported when available and grant tasks are tracked cleanly, you get a clearer compliance trail and faster fixes when outreach or supply plans are off. The software load is modest at $450 per month, but missing proof can still stall partner trust and renewal funding.
Set the reporting rules before the first event
Configure the CRM, define the data fields, and assign who enters each record before launch. The reporting process should capture the same core items every time: participant counts, kits, trainings, referrals, and any reported reversals. That keeps day-one operations simple and stops staff from improvising under pressure.
- Lock fields before first training.
- Train staff on same-day entry.
- Protect personal information first.
- Review outcomes every month.
Use the monthly review to compare outreach, supply use, and reported results. If attendance is low or kit use is higher than planned, you can correct fast instead of finding the gap at renewal time. Clean records also make grant reporting easier and reduce back-and-forth with partners.
6
Related Products
- Overdose Prevention Program Porter's Five Forces Analysis
- Overdose Prevention Program BCG Matrix
- Overdose Prevention Program Business Model Canvas
- What Are The 5 KPI Metrics For Overdose Prevention Program Business?
- Overdose Prevention Program Business Plan Template in Pre-Written Word
- How Increase Overdose Prevention Program Profits?
- What Are Operating Costs For Overdose Prevention Program?
- Overdose Prevention Program Startup Costs: $873K Cash Need
- Overdose Prevention Program Financial Model Template in Excel
- Overdose Prevention Program Owner Income: $110k Salary Plus Surplus
- How To Write Overdose Prevention Program Business Plan?
- Overdose Prevention Program Marketing Mix
- Overdose Prevention Program Marketing Plan
- Overdose Prevention Program Business Proposal
- Overdose Prevention Program PESTEL Analysis
- Overdose Prevention Program Pitch Deck Example Editable PPTX
- Overdose Prevention Program Business SWOT Analysis
- Overdose Prevention Program Value Proposition Canvas
Frequently Asked Questions
Either structure can work, but the funding path changes A nonprofit may fit grants, donations, and public health partnerships A for-profit may fit paid training contracts with employers, schools, hospitality groups, and treatment centers The model assumes Year 1 paid group prices of $900 to $1,200 and 45 total groups across three segments