 Owner income$120k
Owner income$120kHow Much Patient Advocacy Owners Make: $120k Pay To $11M EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$120k  Net margin-181% to 48%
Net margin-181% to 48% Revenue for target pay$250k
Revenue for target pay$250k Business difficultyHard
Business difficultyHard


A patient advocacy business owner can plan for a $120,000 lead advocate salary in this model, but early profit does not support extra draws Researched assumptions show about $84,000 revenue in Year 1, $302,000 in Year 2, and $738,000 in Year 3, with EBITDA reaching break-even around Month 31 The higher-utilization staffed case reaches about $2385 million revenue and $1146 million EBITDA in Year 5 before taxes, reserves, debt service, or distributions Treat these as planning scenarios, not promised income
Owner income$120kNet margin-181% to 48%Revenue for target pay$250kBusiness difficultyHardWant to test your patient advocacy owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, labor, overhead, marketing, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice, and it does not model clinical outcome assumptions.
Want to see the Patient Advocacy income model?
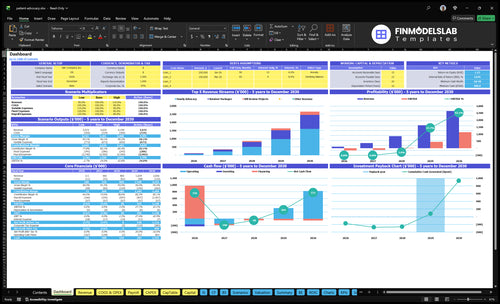
This screenshot shows revenue, margin, costs, reserves, and owner take-home assumptions in the Patient Advocacy Financial Model Template; open the model.
Owner-income model highlights
- Hourly and retainer pricing
- Bill review projects
- Month 31 break-even
- 480k cash floor
How many clients does a patient advocate need?
If Patient Advocacy bills $120/hour and a case takes 25 hours, that is about $3,000 per case, so $120,000 of owner pay alone needs roughly 40 cases before overhead. The bigger test is capacity: Year 1 break-even revenue is about $268,000, while modeled Year 1 revenue is about $84,000. By Year 3, modeled revenue reaches about $738,000 and EBITDA turns positive at about $26,000, but intake, documentation, referral work, admin, and follow-up all count.
Revenue math
- $120/hour is the billing rate.
- 25 hours per case equals about $3,000.
- $120,000 owner pay needs about 40 cases.
- Year 1 modeled revenue is about $84,000.
Real capacity
- Year 1 break-even is about $268,000.
- Year 3 modeled revenue is about $738,000.
- EBITDA turns positive at about $26,000.
- Nonbillable work also uses capacity.
How much should a patient advocate charge?
Patient Advocacy should charge $120/hour in Year 1, rising to $145/hour by Year 5, with higher pricing for complex billing work. Retainers should price at $115–$135/hour, and bill review should run $160–$190/hour; for success tracking, see What Is The Most Important Indicator Of Success For Patient Advocacy Business?. The main risk is unpaid scope creep, so calls, records review, and care-team follow-up need clear billable rules.
Core Rates
- $120/hour Year 1 advocacy rate
- $145/hour Year 5 advocacy rate
- $115–$135/hour retainer package rate
- $160–$190/hour bill review pricing
Scope Math
- 70–100 retainer billable hours
- 15–25 bill review project hours
- $300 Year 1 hourly case revenue
- $805 retainer; $240 bill review
What is the patient advocacy profit margin?
Patient Advocacy can look very profitable on paper, but revenue is not owner income. In the model, gross margin is 900% in Year 1 and 950% in Year 5 after third-party consults and specialized software, and you can see the startup cost context in How Much Does It Cost To Open, Start, And Launch Your Patient Advocacy Business?. The real squeeze is overhead: fixed costs are $4,770/month, payroll rises from $144,000 to $813,000, and marketing grows from $20,000 to $130,000.
Margin math
- Gross margin starts at 900%.
- Gross margin reaches 950% by Year 5.
- Contribution margin rises from 825% to 900%.
- EBITDA is negative in Years 1 and 2.
Cost pressure
- Fixed overhead is $4,770/month.
- Payroll grows from $144,000 to $813,000.
- Marketing grows from $20,000 to $130,000.
- EBITDA margin moves to 35%, 315%, then 481%.
Want the six main patient advocacy income drivers?
1
$120-$190Pricing Model
Higher rates move take-home fast because the same case time earns more across hourly advocacy, retainers, and bill reviews.
2
1.5-10hService Hours
More paid hours per client lift revenue without adding as many new cases, so utilization matters.
3
$160-$190Bill Review
Bill review brings the highest rate, but it only helps income if staff time stays tight and margin does not leak.
4
$400->$250Lead Cost
As customer acquisition cost (CAC) falls from $400 to $250, more of each marketing dollar turns into booked patients.
5
$813KPayroll Load
Year 5 payroll reaches $813K, so hiring pace and role mix decide how much gross profit reaches the owner.
6
31 moPayback Lag
The $4,770 monthly fixed bill and $480K minimum cash need push breakeven to month 31, so early draws stay limited.
Patient Advocacy Core Six Income Drivers
Pricing Model
Pricing Model Drives Pay
Pricing sets revenue per case and what the owner can pay themselves. In patient advocacy, hourly work runs $120 to $145, retainer packages run $115 to $135 per hour across 70 to 100 billable hours, and bill review projects run $160 to $190 per hour. The clean math is simple: more paid hours at the right rate means more gross margin.
The risk is loose scope. If follow-up, family calls, or records chasing is unpaid, a high-fee case can turn into low effective hourly pay fast. Use packages for complex coordination, records review, and recurring family communication so the work stays priced to the time it really takes.
Track Effective Hourly Rate
Measure billable hours, unpaid follow-up, and effective hourly rate by case type. Compare hourly advocacy, retainers, and bill review projects so you know which mix protects owner draw. If the hours are not capped in writing, margin leaks into admin time and care-team follow-up.
- Price every scope change.
- Log unpaid time daily.
- Match packages to complex cases.
Keep the estimate tied to the case. The key inputs are price per hour, paid hours per engagement, and how much nonbillable coordination each client creates.
1
Billable Utilization
Billable Utilization
Owner income rises when more of the week turns into paid advocacy time. In this model, billable hours per engagement run from 25 to 35 for hourly advocacy, 70 to 100 for retainers, and 15 to 25 for bill review, so the same advocate can produce more revenue if scope stays tight and service quality holds.
Here’s the catch: intake, documentation, care-team follow-up, admin, referral development, and client education all eat working time. If those tasks expand, effective hourly pay falls, gross margin tightens, and less cash is left for owner draw. The quick test is billable hours divided by total working hours, by case type.
Raise Paid Advocacy Hours
Track billable hours, nonbillable hours, and revenue per advocate by service line. Then compare hourly advocacy, retainer work, and bill review separately, because the mix changes utilization and pay. A retainer with 70 to 100 billable hours can outperform a smaller hourly case only if follow-up does not spill into unpaid time.
Set clear scope, pre-book follow-ups, and use templates for notes and care-team updates. Measure the share of time spent on intake, documentation, and admin each week. If unpaid work keeps climbing, raise minimum case size, narrow service menus, or price for the extra labor so owner income does not get diluted.
- Count billable hours by case
- Track unpaid follow-up weekly
- Separate results by service type
- Price scope creep before it spreads
2
Client Acquisition
Referral-Led Client Acquisition
When referrals stay steady, the owner spends less time chasing low-fit leads and more time on billable advocacy. Here’s the quick math: annual marketing rises from $20,000 in Year 1 to $130,000 in Year 5, while customer acquisition cost (CAC) improves from $400 to $250. That shift supports more predictable case volume and protects utilization, which lifts take-home income.
This driver includes referral volume, lead quality, consultation close rate, and CAC by source. Useful sources are eldercare professionals, attorneys, caregiver groups, and healthcare-adjacent networks. What this estimate hides: referral channels must avoid improper referral payments and other compliance-sensitive arrangements, or the margin gain can turn into legal and cash flow risk.
Measure CAC by source
Track each source separately: referrals, paid search, events, and partner outreach. If 100 new clients cost $40,000 at a $400 CAC, and then $25,000 at a $250 CAC, that is $15,000 saved on the same volume. Lower CAC gives the owner more room to pay themselves after fixed overhead and staff time.
Focus on referral quality, not just count. Ask which sources bring complex, high-fit cases that convert fast and stay longer. Keep outreach documented, use plain referral rules, and have counsel review any partner setup so growth stays clean and the extra revenue does not get eaten by compliance or wasted marketing spend.
3
Case Complexity And Specialization
Complex Case Pricing
Complex cases can lift revenue fast because the client pays for judgment, not just time. In this model, hourly advocacy often runs $120 to $145, while bill review projects can reach $160 to $190 per hour. The upside only holds if scope stays tight, because unpaid follow-up, extra handoffs, and deep documentation can drag effective hourly pay down.
Track case type, billable hours, and handoffs per client. A care coordination case with many family updates may look premium, but if it turns into heavy admin, owner take-home falls. Keep the work clearly outside medical, legal, tax, or insurance advice unless properly qualified, so the business protects both pricing and risk.
Price by Scope, Not Emotion
Use case details to set price before work starts. Here’s the quick math: revenue per case = billable hours × hourly rate. Higher-value work includes eldercare navigation, insurance appeal support, condition-specific navigation, and records review. Those cases can justify higher fees only when you define what is included, what is excluded, and how many touchpoints the client gets.
- Track billable hours by case type.
- Count nonbillable handoffs and calls.
- Price extra documentation separately.
- Set boundaries on advice and follow-up.
If a case needs more coordination than planned, reset scope early. That protects gross margin and keeps more of the collected fee available for owner pay instead of getting eaten by unpaid work.
4
Staffing Leverage
Staffing Leverage
Staffing leverage means adding senior advocates in Year 2, patient advocates in Year 3, and operations support in Year 3 so one owner can serve more cases. Payroll rises from $144,000 in Year 1 to $813,000 in Year 5, while revenue is modeled to reach $2,385 million by Year 5. That only lifts owner pay if billable volume, pricing, and case mix cover training, quality control, and compliance.
More staff can raise capacity, but it also cuts flexibility and adds management load. If added advocates do not turn nonbillable work into paid hours, the owner ends up funding payroll growth instead of taking home more profit. Here’s the quick math: payroll grows about 5.6x from Year 1 t o Year 5, so the business needs steady case flow and tight scope control to keep draws safe.
Track capacity before you hire
Measure billable hours per advocate, revenue per case, and payroll as a share of revenue before each hire. Tie senior advocates to complex cases, patient advocates to higher case volume, and operations support to less admin drag. If a role does not lift billed capacity, it can lower owner income even when revenue looks bigger on paper.
Use staffing only when the pipeline can fill the added hours. Track intake, scheduling, documentation, follow-up, and compliance work, then forecast how many paid hours each hire must create to cover salary plus oversight. If scope is loose or handoffs are messy, unpaid work rises fast and effective margin falls.
5
Overhead And Reserves
Overhead and Reserve Discipline
$4,770 a month in fixed overhead covers rent, utilities, privacy-compliant CRM and billing software, supplies, legal and accounting, IT, telecom, and training. That base cost is small, but it still sets the floor for owner pay. When revenue-linked costs fall from 175% in Year 1 to 100% in Year 5, more profit can stay in the business instead of being eaten by operating drag.
The cash rule matters too: the minimum cash need is $480,000 at Month 31. That means the owner should not pull every dollar of EBITDA, or earnings before interest, taxes, depreciation, and amortization. Safer draws start after break-even and after reserves are funded, so the business can handle slow collections, unpaid follow-up, and case spikes without starving payroll or operations.
Hold the Line on Cash
Track fixed overhead, revenue-linked cost %, and cash on hand every month. If overhead rises above $4,770 without more billable hours, owner pay gets squeezed fast. If costs stay high in Year 1, keep draw policy tight and use cash to build the reserve instead of paying out profit too early.
- Watch monthly overhead per active client.
- Check reserve runway against Month 31.
- Set draws after break-even only.
Here’s the quick math: lower overhead and lower variable costs raise the share of revenue that can become free cash. But what this estimate hides is timing risk, since patient work can bill late and collect late. That’s why the reserve is not optional; it protects owner pay when collections slip or case volume dips.
6
Compare lean, base, and high patient advocacy owner income scenarios
Owner income scenarios
Owner income shifts with client mix, staffing, and marketing spend. Year 1 is cash negative, Month 31 is near breakeven, and Year 5 is strongly profitable.
| Scenario | Low CaseHard ramp | Base CaseBreakeven path | High CaseScale win |
|---|---|---|---|
| Launch model | This is the early ramp case, where owner pay is likely limited until funding covers the Year 1 loss. | This is the modeled breakeven case, where the business is close to covering payroll and overhead from operations. | This is the upside case, where scaled client volume and a larger team produce strong owner income. |
| Typical setup | Year 1 reaches about $84,000 revenue, with 75% hourly advocacy, $144,000 payroll, $57,240 fixed overhead, and $20,000 marketing, so EBITDA is about -$152,000. | Year 3 reaches about $738,000 revenue, with direct costs still light, $487,000 payroll, $70,000 marketing, and EBITDA near $26,000. | Year 5 reaches about $2.385 million revenue, with $813,000 payroll, $130,000 marketing, and EBITDA near $1.146 million. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | -$152,000Loss year | $26,000Near breakeven | $1.146MUpside year |
| Best fit | Use this to stress-test cash needs when demand is still thin and owner pay is not yet dependable. | Use this as the main planning case if you expect steady client flow and gradual team expansion. | Use this to test upside if referral flow, pricing, and staffing all scale cleanly. |
Planning note: These scenario ranges are researched planning assumptions from the model, not guaranteed earnings, salary promises, tax advice, or distribution forecasts.
Related Products
- Patient Advocacy Porter's Five Forces Analysis
- Patient Advocacy BCG Matrix
- Patient Advocacy Business Model Canvas
- 7 Critical Financial KPIs for Patient Advocacy
- Patient Advocacy Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Patient Advocacy Profitability
- How to Budget and Run a Patient Advocacy Business Monthly
- Patient Advocacy Startup Costs: $585K CAPEX And $480K Cash
- Patient Advocacy Financial Model Template in Excel
- How To Start A Patient Advocacy Business In 6–10 Weeks
- How to Write a Patient Advocacy Business Plan (7 Steps)
- Patient Advocacy Marketing Mix
- Patient Advocacy Marketing Plan
- Patient Advocacy Business Proposal
- Patient Advocacy PESTEL Analysis
- Patient Advocacy Pitch Deck Example Editable PPTX
- Patient Advocacy Business SWOT Analysis
- Patient Advocacy Value Proposition Canvas
Frequently Asked Questions
The model includes a $120,000 lead advocate salary, but extra draws are not supported in the early ramp EBITDA is -$152,000 in Year 1 and -$124,000 in Year 2 By Year 5, the staffed case reaches about $1146 million EBITDA before taxes, reserves, debt service, or distributions