 Time to Open12 weeksOpening prep
Time to Open12 weeksOpening prepHow To Open A Patient Transport Service In 60–120 Days

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Time to Open12 weeksOpening prep  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckInsurance gateLead time
Key BottleneckInsurance gateLead time First Revenue StepPrivate-pay ridesBooking live
First Revenue StepPrivate-pay ridesBooking live


Key Takeaways
- Complete compliance, insurance, and permits before first trips.
- Use vehicle checks and backup capacity to cut cancellations.
- Train drivers on securement, CPR, and patient assistance.
- Build referral sources early to speed first revenue.
Time to Open12 weeksOpening prepLaunch Sequence6 stagesCompliance firstKey BottleneckInsurance gateLead timeFirst Revenue StepPrivate-pay ridesBooking liveLaunch timeline
Short web summary of the launch plan; the XLSX export carries the detailed Gantt Chart and task dependencies.
Launch scheduleWeek 1Week 2Week 3Week 4Week 5Week 6Week 7Week 8Week 9Week 10Week 11Week 12
Compliance
- Register entity
- Review transport rules
- Broker credential packet
- Secure permits
- Policy signoff
Insurance
- Quote auto policy
- Compare cover limits
- Bind policy
- Issue certificates
- Confirm exclusions
Vehicles
- Source vehicles
- Inspect units
- Add equipment
- Register fleet
- Set maintenance plan
Staffing
- Post driver roles
- Screen applicants
- Background checks
- Train drivers
- Final shift roster
Dispatch
- Select dispatch tool
- Build trip flows
- Set service area
- Test bookings
- Support desk setup
Outreach
- Build referral list
- Send intro pack
- Call facilities
- Run pilot trips
- Start paid trips
Why test the Patient Transport Service model before launch?
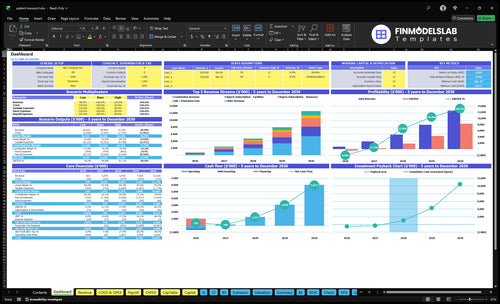
Open the Patient Transport Service Financial Model Template to see revenue, costs, cash needs, assumptions, and break-even logic.
Financial model highlights
- 60-month horizon
- Year 1 AOVs: $60/$75/$70
- Repeat orders: 15/8/15
- 15% plus $2 fees
- Driver schedule and utilization
- Insurance burden in costs
- Trips, payer mix, staffing
- Runway and breakeven path
How do you get clients for a patient transport service?
For a Patient Transport Service, first clients should come from credible healthcare referral sources, not broad ads alone. Start with dialysis centers, rehab facilities, senior living communities, hospital discharge planners, home health agencies, case managers, Medicaid brokers, and private-pay caregivers; see What Is The Estimated Cost To Open And Launch Your Patient Transport Service Business? for launch budgeting context. In Year 1, a practical mix is 70% individual patients, 25% facilities, and 5% insurance, because reliability is what gets repeat bookings.
Best referral sources
- Dialysis centers first
- Rehab and discharge planners
- Senior living communities
- Home health and case managers
What closes repeat business
- Hit on-time pickups
- Keep vehicles clean
- Use trained drivers
- Set missed-pickup steps
How long does it take to start a patient transport business?
For a Patient Transport Service, the practical launch window is 60–120 days. It can move faster if you start private-pay, but broker-based launch usually takes longer because vehicle acquisition, accessibility equipment, inspections, commercial auto insurance underwriting, driver onboarding, dispatch setup, facility approvals, and payer credentialing all have to line up. Don’t open until test trips, pickup protocol, documentation, and billing handoff work in real conditions.
Fast launch path
- 60–120 days is the launch window.
- Private-pay can open faster.
- Vehicles and equipment come first.
- Inspections and insurance can slow you down.
Open only when ready
- Run test trips before launch.
- Confirm pickup steps work.
- Check documentation handoff.
- Verify billing flow in real trips.
What patient transport startup mistakes create launch risk?
The biggest launch risk for a Patient Transport Service is starting before the basics are documented and live. If vehicles are underinsured, drivers are untrained, dispatch is weak, or there’s no backup vehicle plan, the first week can go sideways fast. Before launch, require insurance proof, driver training files, vehicle inspection records, daily route checks, patient assistance standards, and billing documentation.
Launch risk points
- Underinsured vehicles create exposure.
- Untrained drivers raise care risk.
- Weak dispatch causes missed pickups.
- No backup plan hurts reliability.
Go-live checklist
- Verify insurance before first trip.
- Save driver training files.
- Record vehicle inspections daily.
- Open only after referral channels work.
Verify what must be ready before accepting patient rides
Launch readiness checklist
Use this go-live approval checklist to confirm the patient transport service is ready before opening.
Registration
- Business registration filed and activeCritical
The entity must exist before permits, bank setup, and contracts.
- State transport license verifiedCritical
No ride should start without the state permit.
- Local operating permits confirmedHigh
Local rules can block service even when the state license is ready.
- Commercial auto and liability boundCritical
Coverage must be active before the first ride.
Fleet
- Vehicle inspections passedCritical
Unsafe vehicles cannot carry patients.
- Wheelchair equipment testedHigh
If wheelchair rides are offered, the lift and anchors must work.
- Safety kit and cleaning setMedium
Supplies should support safe, clean handoffs on every trip.
Drivers
- Driver files completeCritical
Licenses, IDs, and records should be on file before dispatch.
- Background checks clearedCritical
Patients and facilities need vetted drivers.
- Transfer training passedCritical
Drivers must know pickup, transfer, and lift steps before launch.
Dispatch
- Service area map approvedHigh
Dispatch needs a clear zone so trips do not overrun capacity.
- Dispatch workflow testedCritical
Book, assign, and close trips before live requests start.
- Pickup protocol signed offCritical
Missed pickups damage trust and can stall repeat orders.
Revenue
- First-revenue channel liveCritical
At least one way to book rides must work on day one.
- Referral list approvedHigh
Facilities and payers drive early volume.
- Billing and claims testedCritical
Payment, invoicing, a nd claim steps must work without manual fixes.
- Year 1 mix validatedMedium
Use 70% individual patients, 25% facilities, 5% insurance as the launch mix check.
Go-live
- Cash runway covers Month 16Critical
Minimum cash hits $221k in Month 16, so runway must cover that dip.
- Staffing coverage schedule setHigh
Trips need enough coverage for dispatch, office work, and backfill.
- No-go criteria documentedCritical
Block launch if insurance, training, vehicles, pickup, or docs are not ready.
- Launch signoff recordedCritical
Final signoff should confirm all launch gates are green.
Want the six main launch drivers for patient transport?
1Compliance
Go/no-goClears permits, driver standards, and payer enrollment so first trips can run without shutdown risk.
2Vehicle Readiness
60-120 daysReduces first-week cancellations by matching vehicle mix, inspections, and backup capacity to routes.
3Insurance
Coverage onKeeps launch contract-ready with active coverage tied to vehicles, drivers, and service scope.
4Driver Training
Opening monthProtects opening capacity with screened, trained drivers ready for patient support and securement.
5Dispatch Ops
Test tripsImproves on-time trips by testing booking, routing, handoffs, and no-show handling before go-live.
6Referral Pipeline
70/25/5 mixDrives first revenue by booking patients, facilities, and insurance sources before opening.
Compliance And Credentialing
Compliance and Credentialing
This is the go/no-go gate. If state rules, local permits, payer requirements, driver standards, vehicle documents, and broker enrollment are not in place before first trips, the business may open late or start with rejected rides and billing delays.
The readiness signal is a complete compliance file for the business, each vehicle, each driver, and every payer channel. One missing approval can block day-one operations even if the app, routes, and staff are ready.
Build the compliance file first
Start with the slowest approvals first, then work backward to opening day. Keep one dated checklist for filings, permits, driver credentials, vehicle papers, and broker enrollment so you can see what still needs action and what can slip the launch date.
Run a mock trip review before opening. If a trip still needs manual fixes to pass compliance checks, the first week will be messy. That leads to fewer rejected trips, cleaner billing, and lower shutdown risk only if the file is current and easy to audit.
- Confirm state rules early.
- Collect local permits before launch.
- File driver and vehicle records.
- Finish payer and broker enrollment.
- Track renewals on one calendar.
1
Vehicle Readiness
Vehicle Readiness
Vehicle readiness decides what trips you can take on day one. If the first fleet mix does not match ambulatory demand, wheelchair-access needs, and your service area density, you will get cancellations, slow dispatch, or a hard stop before opening. The launch risk is simple: no compliant, usable vehicle means no trip capacity.
This driver includes inspections, accessibility equipment checks, safety supplies, cleaning, and a maintenance plan. It also depends on insurance and driver assignment. If backup vehicles are not lined up, even one breakdown can cut first-week service and hurt trust with facilities and families.
Check Fleet Before Opening
Build the launch list around the exact trip types you can serve now: ambulatory rides, and wheelchair-accessible rides only if you have the vehicle and equipment to support them. Test every unit before opening and document that the vehicle, securement gear, safety kit, and cleaning setup are ready.
- Match vehicles to booked trip type
- Verify accessibility gear works
- Keep a backup unit ready
- Set maintenance and cleaning logs
If the first vehicle set is thin, your opening date may still stand, but service quality will slip fast. One missed inspection or failed equipment check can turn into a cancelled trip, delayed pickup, or a compliance issue before the first week is over.
2
Commercial Insurance
Commercial Insurance
For a patient transport service, commercial auto insurance, general liability, and workers’ compensation where required are a launch gate, not a back-office task. Without active proof of coverage tied to the right vehicles, drivers, and service scope, you can’t confidently open, contract, or respond to an incident on day one.
The main delay risk is underwriting approval. If the policy does not match the actual NEMT operation, trips can be blocked, payer acceptance can stall, and the business can be exposed to shutdown or claim problems before the first ride is completed.
Bind Coverage Before First Dispatch
Before launch, verify that the insurer has the exact vehicle list, driver roster, and service scope in writing. The readiness file should show active coverage for each vehicle and driver class, plus any payer-required coverage needed for billing and contracts.
- Match policy names to real vehicles.
- Confirm driver coverage before dispatch.
- Save certificates and endorsements.
- Check payer-required limits early.
- Recheck after any fleet change.
If coverage is still pending, hold launch. A clean insurance file is what lets you operate, sign contracts, and handle incidents without stopping day-one service.
3
Driver Hiring And Training
Driver Readiness
Driver hiring and training is a go-live gate for a patient transport service. If drivers are not cleared for clean driving records, background checks, patient service fit, CPR or first aid, wheelchair securement, and patient assistance standards, you cannot safely cover day one routes. Weak training shows up as missed pickups, unsafe transfers, and weaker referral trust.
The key dependency is vehicle availability and insurance approval before driver assignment. Your readiness signal is trained driver coverage for the opening month, not just a few hires. If the roster is thin, one callout can break the schedule and delay first revenue.
Train before first trips
Build the roster from the route plan. Verify each driver, then assign trips only after the vehicle and insurance file are active. That keeps the launch tied to actual capacity, not hopeful staffing.
- Check records and background first.
- Confirm CPR or first aid expectations.
- Test wheelchair securement hands-on.
- Document patient assistance standards.
- Cover opening month routes.
Keep a backup driver list ready. If onboarding slips, the opening schedule will slip too, and facilities will notice the first missed pickup fast.
4
Dispatch And Trip Operations
Dispatch And Trip Operations
Dispatch is the day-one control center. For a patient transport service, it covers booking intake, trip confirmation, routing, driver communication, no-show handling, documentation, billing handoff, and patient service rules. If this flow is not ready, you may open late even if you have vehicles and drivers, because trips still fail at the handoff point.
The key dependency is driver schedule and vehicle status. A weak dispatch process creates late pickups, missed appointments, and messy records, which then trigger disputes with families, facilities, and payers. Successful test trips before launch are the readiness signal, because they show the team can move from booking to arrival without manual chaos.
- Inputs: booking intake, route rules, driver contact list
- Inputs: no-show policy, trip logs, billing packet
- Inputs: patient service script, backup vehicle plan
Test the trip flow before opening
Run at least one end-to-end test trip for each service type you plan to launch. That means booking, confirmation, driver assignment, pickup, drop-off, trip note, and billing handoff all work with real people and real timing. If any step still needs a founder to fix it live, the launch plan is not ready.
Assign one person to watch the clock and one to watch the records. Confirm driver availability, vehicle status, and backup coverage before each trip window, then document who handled no-shows, delays, and patient updates. Clean handoffs matter here, because a missed note or late status update can turn one bad trip into a payer dispute.
5
Referral And Payer Pipeline
Referral Pipeline
This launch driver decides whether you have booked or qualified trip sources before opening. For this business, that means dialysis centers, rehab providers, senior care organizations, hospital discharge planners, home health agencies, case managers, private-pay families, and transportation brokers ready to send rides from day one. If those sources are not in place, vehicles sit idle and first-month revenue ramps slower.
The Year 1 mix assumes 70% individual patients, 25% facilities, and 5% insurance readiness. That mix matters because individual demand can start fast, but facility relationships usually create steadier volume. Insurance is the slowest path, so if payer setup is weak at launch, early trips may still run, but claims and reimbursement can lag.
Pre-Open Demand Setup
Before opening, verify every referral path that can produce a real trip request, not just a warm lead. Get the list of active contacts, decision makers, billing rules, and booking method for each source. One clean pipeline is better than ten vague promises.
Sequence the work around readiness: confirm facility contacts, document payer requirements, and track which sources are booked, qualified, or still pending. If you can’t point to actual trip sources, the launch plan is too thin and your first-week dispatch schedule will be unreliable.
- Confirm discharge planner contacts
- Log facility booking rules
- Track qualified trip sources
- Separate private-pay and payer leads
- Test handoff from referral to dispatch
6
Related Products
- Patient Transport Service Porter's Five Forces Analysis
- Patient Transport Service BCG Matrix
- Patient Transport Service Business Model Canvas
- 7 Critical Patient Transport Service KPIs to Track for Scale
- Patient Transport Service Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Patient Transport Service Profitability
- Operating Costs for a Patient Transport Service Platform (2026 Forecast)
- Patient Transport Service Startup Costs: $105M Before Vehicles
- Patient Transport Financial Model Template in Excel
- How Much Do Patient Transport Service Owners Make at 15% Take-Rate
- How to Write a Patient Transport Service Business Plan in 7 Steps
- Patient Transport Service Marketing Mix
- Patient Transport Service Marketing Plan
- Patient Transport Service Business Proposal
- Patient Transport Service PESTEL Analysis
- Patient Transport Service Pitch Deck Example Editable PPTX
- Patient Transport Service Business SWOT Analysis
- Patient Transport Service Value Proposition Canvas
Frequently Asked Questions
Start with compliance, insurance, vehicles, drivers, dispatch, and referrals Use the 60–120 day window as your planning range, then build backward from the first ride The Year 1 model assumes 70% individual patients, 25% facilities, and 5% insurance, so outreach should not wait until opening week