 Time to Open6-12 monthsSetup window
Time to Open6-12 monthsSetup windowHow To Open A Pediatric Clinic: 6 To 12 Month Launch Roadmap

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6-12 monthsSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckPayer enrollmentEnrollment lag
Key BottleneckPayer enrollmentEnrollment lag First Revenue StepBooked visitsBilling live
First Revenue StepBooked visitsBilling live



You’re opening a pediatric office that has to work for babies, children, teenagers, parents, payers, and staff from day one This launch guide covers the 6 to 12 month opening path, including licensing, payer credentialing, site setup, EHR, vaccine readiness, staffing, and first-patient flow, with financial validation used only to test timing and capacity
Time to Open6-12 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckPayer enrollmentEnrollment lagFirst Revenue StepBooked visitsBilling liveLaunch timeline
Short web summary of the clinic launch plan; the XLSX export contains the full Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11
Legal / compliance
- Permit review
- License filings
- Insurance bind
- Policy draft
- Final inspection
Payer credentialing
- Payer packet
- Medicaid CHIP enrollment
- Commercial enrollments
- Rate setup
- Approval follow-up
Lease / buildout
- Site lock
- Floor plan
- Buildout work
- Furnish rooms
- Equipment install
EHR / billing
- Software selection
- System setup
- Data migration
- Billing rules
- Live testing
Staffing / training
- Role plan
- Recruit team
- Onboard hires
- Clinical training
- Dry run
Vendors / launch
- Vaccine sourcing
- Lab vendors
- Stock supplies
- Patient outreach
- Go-live prep
Why test Pediatric Clinic launch assumptions before you sign the lease?
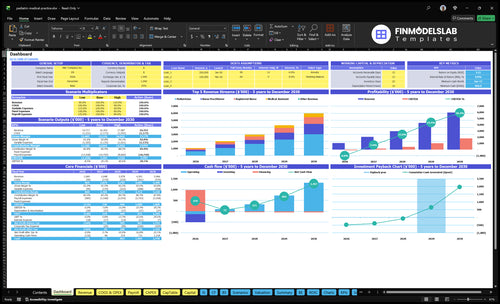
Pediatric Clinic Financial Model Template shows revenue ramp, staffing, fixed costs, variable costs, cash runway, and break-even path so you can validate Year 1 before lease or hires.
Year 1 model highlights
- 2 pediatricians, 1 nurse practitioner
- Revenue about $883k monthly
- Variable costs at 18%
- Fixed overhead: $1.475m
- Wages about $625k
- Test before payer approvals
What can go wrong opening a pediatric clinic?
If you open a Pediatric Clinic before payer approvals, billing checks, and vaccine handling are ready, you can trigger denied claims and unsafe care fast. The safe move is to verify payer status, test the claim workflow, confirm CLIA needs for lab testing, and use a soft opening before the first full schedule.
Main risks
- Denied claims from missing approvals
- Billing errors from weak workflows
- Vaccine risk from poor storage logs
- Safety gaps from weak triage
Open only when ready
- Check payer approval status first
- Test one claim end to end
- Log vaccine temperatures daily
- Use staff scripts and EHR templates
How do you get patients for a pediatric clinic?
Get patients by building a steady referral path from newborn follow-ups, well-child visits, and sick visits, then make it easy to find and book you online; for setup costs, see What Is The Estimated Cost To Open And Launch Your Pediatric Clinic?.
Use insurance directory listings, local SEO, a local search profile, online scheduling, OB/GYN relationships, hospital newborn referral pathways, daycare and school outreach, parent groups, and community events. In Year 1, plan on 320 monthly visits per pediatrician and 280 monthly visits per nurse practitioner before capacity adjustment, and track booked visits, no-shows, payer mix, and billing acceptance.
Patient sources
- Start with newborn follow-ups
- Fill well-child visits
- Add sick visits
- Use OB/GYN referrals
Capacity checks
- Track booked visits weekly
- Watch no-shows by payer
- Review payer mix monthly
- Confirm billing acceptance fast
What licenses do you need to open a pediatric clinic?
To open a Pediatric Clinic in the US, you typically need active state medical licenses, compliant entity setup, malpractice coverage, HIPAA and OSHA programs, DEA registration if prescribing controlled substances, a CLIA waiver for in-office lab tests, local permits, and vaccine program enrollment where used; this is not legal advice, and What Is The Most Important Indicator To Measure The Success Of Pediatric Clinic? matters once licensing clears.
Core Licenses
- Active state medical licenses for clinicians
- State medical board compliance rules
- Entity setup and ownership review
- Local business permits before opening
Operating Rules
- DEA registration: $888 per 3 years
- CLIA waiver: $248 every 2 years
- OSHA bloodborne training at least annually
- Vaccine programs serve children through age 18
Validate whether the pediatric clinic is ready before opening day
Launch readiness checklist
Use this go-live approval checklist to confirm the pediatric clinic is ready before opening.
Clearance
- Entity and ownership documentedCritical
This must match state ownership rules before contracts and billing start.
- State medical license verifiedCritical
No patient care can start until the pediatric license is active.
- Local permits clearedHigh
Occupancy and local permits need to be in hand before opening day.
- Malpractice coverage boundCritical
Coverage must be active before any child is seen in the clinic.
Facility
- Exam rooms ready for pediatricsCritical
Rooms need safe flow, child-sized setup, and clean work space.
- Vaccine refrigerator tested and loggedCritical
Cold storage must hold safe temperatures before vaccine stock arrives.
- Clean waste flow approvedHigh
Cleaning and medical waste steps must work before first visits.
Access
- EHR configured for visitsCritical
Visit notes, orders, and charting must work before opening.
- Billing and claims rules loadedCritical
Claims setup must be ready so visits can turn into cash.
- Scheduling and phone system testedHigh
Families need a working way to book, reschedule, and reach the clinic.
- Website and profile liveMedium
Parents should find hours, services, and location before launch.
Supplies
- Pediatric supplies fully stockedCritical
Basic exam and treatment supplies must cover the first patient wave.
- Immunization registry workflow activeCritical
Vaccines need a clear record path to avoid missed reporting.
- Lab waiver if testing offeredHigh
Basic test plans need the right waiver before any on-site lab work.
Staffing
- Clinical roles staffed to planCritical
The opening schedule needs enough clinicians and support staff on site.
- New hire training completedCritical
Staff must know charting, handoffs, safety steps, and escalation rules.
- After-hours coverage policy setHigh
Families need clear guidance when the clinic is closed.
Cash
- Payer credentialing completeCritical
If payers are not ready, the clinic can see patients but not bill cleanly.
- Copay and claims flow testedHigh
First visits need a working payment and claim path from day one.
- Cash runway covers Month 13Critical
The model shows minimum cash at $469k in Month 13, so launch cash must cover that dip.
- Go-live signoff completedCritical
This final check confirms no blocker remains for safe opening.
What drives a pediatric clinic launch?
1Payer Credentialing
Claim gateApproved provider numbers let insured visits bill cleanly from day one.
2Medical Compliance
License gateLicenses, policies, and insurance must be in place before payer enrollment and opening.
3Location Buildout
6-12 moUsable rooms and working utilities prevent opening-week bottlenecks and keep visits moving.
4Pediatric Staffing
Yr1 teamYear 1 team of 2 pediatricians, 1 nurse practitioner, 2 registered nurses, 2 medical assistants, and 2 admin staff supports 65% and 60% utilization.
5Supply Readiness
7%+2%Cold chain, supplies, and lab vendors must be ready before families book service-heavy visits.
6Patient Acquisition
4% revLocal search, directories, and referral paths turn payer-ready capacity into booked first visits.
Payer Credentialing And Insurance Contracts
Payer Credentialing
If insured visits can’t be billed on day one, the clinic is open in name only. Commercial plans, Medicaid, CHIP, provider enrollment, group enrollment, contracts, fee schedules, and directory listings all sit on the critical path, and credentialing often runs 60–120 days.
Readiness is approved provider numbers plus a clean billing test before the first insured appointment. If this slips, you can still see families, but claims stall, cash comes in late, and well-child visits, sick visits, and newborn follow-ups may need self-pay handling or rescheduling.
Start Enrollment Early
File payer packets as soon as the legal entity, licenses, and malpractice binder are active. Track each payer by submission date, missing items, provider number, effective date, and directory update. One clean rule helps: don’t book insured patients until the first test claim pays or rejects for a known fix.
- Submit commercial, Medicaid, CHIP together.
- Match individual and group enrollment.
- Verify fee schedules before scheduling.
- Test claim codes before first visits.
1
Medical Compliance And Legal Readiness
Medical Compliance Readiness
Medical compliance is the gate before you can hire, prescribe, bill, or open. For a pediatric clinic, that means licensed providers, legal entity setup, physician ownership rules where they apply, malpractice insurance, HIPAA and OSHA policies, prescribing rules, a CLIA waiver if testing is offered, and local permits. No compliance packet, no opening.
If this work slips, you can still have a lease, staff, and booked families, but you cannot safely see children on day one. State-specific verification also sits before payer enrollment, hiring, prescribing, and lab testing, so weak execution can push back first revenue and raise legal risk fast.
Lock the compliance file early
Build one launch folder with every active document: licenses, entity filings, insurance binders, and approved policies. The readiness signal is simple: each item is current, signed, and easy to show during state review. If testing is part of the launch, confirm the CLIA waiver and any local permit before you set the opening date.
Assign one owner to track renewals, signatures, and state verification. Then test the dependent steps in order: onboarding, prescribing, lab workflow, and billing setup. That sequence matters because a missing approval can idle payroll, delay patient visits, and force you to open with less than full service.
- Verify provider licenses first.
- Collect malpractice proof early.
- Approve HIPAA and OSHA policies.
- Confirm prescribing authority by state.
- File permits before patient scheduling.
2
Location Buildout And Exam Room Setup
Room Flow and Setup
Families feel the buildout before they meet the doctor. The clinic has to support safe waiting, front desk intake, exam rooms, sanitation, storage, accessibility, vaccine handling, and pediatric equipment. If usable rooms, working utilities, or cleaning paths are not ready, opening slips and the first week turns into a scramble.
The Month 1 fixed overhead is already live: $85k rent, $12k utilities, $15k EHR and software, and $800 IT support per month. If the layout slows check-in, room turnover, or vaccine handling, you burn cash before visits start and create bottlenecks on day one.
Test the patient path first
Walk the full visit flow before opening. Check that parents can enter, wait, check in, move to a room, and leave without crossing dirty traffic or crowding the front desk. Secure records areas, storage, and vaccine handling before the first appointment. One clean handoff from intake to rooming saves time all day.
- Map door-to-discharge flow.
- Test power, internet, and refrigeration.
- Confirm cleaning stations and turnover steps.
- Lock secure records and supply storage.
3
Pediatric Staffing And Provider Coverage
Provider Coverage
Opening depends on having enough licensed hands on the floor. The Year 1 plan assumes 2 pediatricians, 1 nurse practitioner, 2 registered nurses, 2 medical assistants, and 2 admin staff, so a staffing miss can delay first visits even if the space is ready. Here’s the quick math: disclosed clinician and support wages total $750,000 per year before admin pay.
If schedules, triage, billing, and front desk coverage are thin, parents feel it first as long waits, missed calls, or canceled same-day sick visits. The readiness signal is simple: trained staff, visit protocols, schedule templates, and after-hours coverage are all live before day one.
Staff Before You Open
Lock the roster in order: licensed providers first, then nursing and medical assistant coverage, then admin for scheduling and billing. Do not open with a full appointment grid until each role is trained on intake, vaccine flow, charting, and parent calls. One clean rule: if a shift cannot be covered, the template is not ready.
- Assign one owner per shift.
- Test sick and well-visit templates.
- Train after-hours call coverage.
- Confirm billing handoff before launch.
A weak staffing setup can create a day-one bottleneck even with demand in the pipeline. If one provider calls out and there is no backup, the clinic loses capacity, and first revenue slips while fixed costs keep running.
4
Vaccine, Lab, Supply, And Vendor Readiness
Vaccine, Lab, and Supply Readiness
This driver decides whether the clinic can deliver pediatric care on day one. Vaccine refrigeration, temperature logs, immunization registry workflow, and stocked medical supplies and PPE must be ready before families arrive, or visits stall and opening slips.
The Year 1 model assumes 7% of revenue for medical supplies and vaccines and 2% for lab test outsourcing. If in-office tests are offered, a CLIA waiver is part of readiness. The real risk is booking patients before storage, vendors, and staff can support care.
Lock Vendor and Storage Controls Before Scheduling
Verify the storage process, inventory control, backup power or backup storage plan, vendor contacts, and delivery timing before the first appointment is opened. Keep a written list of vaccine and supply reorder points, plus who checks logs each day. That is the difference between a clinic that opens and one that cancels visits.
Train staff on receiving, storing, documenting, and restocking supplies before launch. Test the immunization registry workflow and any lab send-out process with one mock visit. What this hides: if families can book visits but vaccines, PPE, or lab partners are not live, first-day revenue drops and trust takes the hit.
5
Patient Acquisition And Local Demand
Patient Demand Before Opening
This clinic can’t treat demand as a marketing problem only. If parents book insured visits before payer enrollment, directory listings, and claim rules are live, the schedule fills but cash doesn’t. The opening date is really gated by whether the first appointment can be booked, seen, coded, and billed on day one.
Year 1 marketing and patient acquisition is modeled at 4% of revenue, so the spend is modest, but only if the flow works. Here’s the quick check: live website, local search profile, directory listings, referral scripts, and online scheduling must be ready before outreach starts, or you risk manual workarounds and delayed first revenue.
Build Demand in the Right Order
Start with insurance directories, local search, and online scheduling, then add OB/GYN and hospital newborn paths, daycare and school relationships, parent groups, and community events. One clean rule: don’t spend on traffic until the claim path is ready. If booked visits can’t be submitted, your first-patient marketing just creates unpaid work.
- Live website and scheduling.
- Directory listings and referral scripts.
- Payer-ready billing workflow.
- Tracked first appointments by source.
6
Related Products
- Pediatric Clinic Porter's Five Forces Analysis
- Pediatric Clinic BCG Matrix
- Pediatric Clinic Business Model Canvas
- 7 Critical KPIs for Scaling a Pediatric Clinic
- Pediatric Clinic Business Plan Template in Pre-Written Word
- Increase Pediatric Clinic Profitability: 7 Actionable Strategies
- How to Calculate Monthly Running Costs for a Pediatric Clinic
- How Much Does It Cost To Open A Pediatric Clinic? $370K CAPEX
- Pediatric Clinic Pro Forma & 5-Year Financial Model Template in Excel
- How Much Does a Pediatric Clinic Owner Make? $59K To $871K
- How to Write a Pediatric Clinic Business Plan in 7 Steps
- Pediatric Clinic Marketing Mix
- Pediatric Clinic Marketing Plan
- Pediatric Clinic Business Proposal
- Pediatric Clinic PESTEL Analysis
- Pediatric Clinic Pitch Deck Example Editable PPTX
- Pediatric Clinic Business SWOT Analysis
- Pediatric Clinic Value Proposition Canvas
Frequently Asked Questions
Start with licensing, entity setup, payer credentialing, malpractice coverage, HIPAA and OSHA policies, a clinic site, EHR, billing setup, pediatric staff, and vaccine readiness Plan around a 6 to 12 month timeline In the researched case, Year 1 staffing starts with 2 pediatricians, 1 nurse practitioner, 2 registered nurses, 2 medical assistants, and 2 admin staff