 Owner income$504k
Owner income$504kHow Much Does A Pharmacy Owner Make? $130k Salary Plus Profit

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$504k  Net margin444%
Net margin444% Revenue for target pay~$842k
Revenue for target pay~$842k Business difficultyHard
Business difficultyHard


You’re weighing owner pay against a store that has heavy staffing, inventory, and reimbursement risk This US retail pharmacy estimate covers a five-year model period, with Year 1 planning assumptions of $842k revenue, 90% gross margin, and owner take-home before personal taxes that depends on pharmacy benefit manager (PBM) fees, payroll, debt, reserves, and location
Owner income$504kNet margin444%Revenue for target pay~$842kBusiness difficultyHardWant to test your pharmacy owner income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Actual owner income depends on revenue, margins, payroll, debt, reserves, and taxes; it is not guaranteed salary, tax advice, or owner distribution advice.
Want the pharmacy financial model view for owner income?
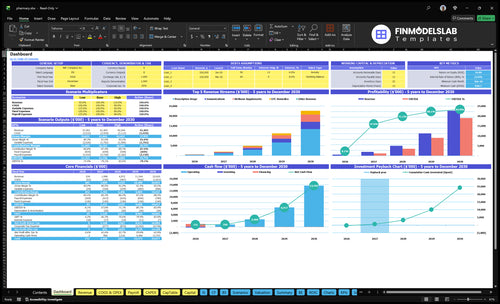
Dashboard tab shows revenue, gross profit, operating profit, and owner salary capacity in the Pharmacy Financial Model Template—open it.
Owner-income model highlights
- Owner salary capacity
- 110-280 weekday visitors
- 18%-38% conversion
- 60%-85% repeat rate
- Working capital and debt
Is owning an independent pharmacy profitable and worth it?
Yes, Pharmacy can be profitable, but only if volume, payer mix, and payroll coverage leave room for owner pay after cash reserves. The provided Year 1 model shows $842k revenue, $711k contribution profit, $1,975k payroll, $1,398k fixed costs, and about $374k operating profit before taxes, debt, and reinvestment. The hard part is cash flow: staffing shortages, compliance, reimbursement timing, inventory funding, and competition can drain it fast.
Profit drivers
- $374k operating profit is the cushion.
- $842k revenue supports owner pay.
- Volume and payer mix do the heavy lifting.
- Repeat use builds steadier cash.
Cash risks
- $1,975k payroll is a big load.
- $1,398k fixed costs are hard to flex.
- Reimbursement timing can delay cash.
- Use front-end sales, immunizations, and disciplined purchasing.
What is the difference between pharmacy owner salary and pharmacist salary?
A pharmacist salary is pay for work; pharmacy owner income can include salary plus profit distributions, but only after cash needs are covered. In this Pharmacy model, Year 1 includes a $130k Pharmacist in Charge salary and about $374k operating profit before debt, taxes, reserves, and reinvestment, so What Is The Most Critical Metric To Measure The Success Of Your Pharmacy Business? matters because owner pay follows cash flow, not just sales.
Salary vs. owner pay
- Pharmacist salary: $130k payroll cost
- Owner income: salary plus distributions
- Distributions come after cash obligations
- Ownership does not always pay more
Year 1 math
- Technicians: 15 × $45k = $675k
- Operating profit: about $374k
- Before debt, taxes, and reserves
- If owner is not pharmacist, $130k remains payroll
How many prescriptions does a pharmacy need to be profitable?
There isn’t one universal prescription count for a Pharmacy. Using the provided model, $281k in monthly fixed costs and a $65 prescription price imply break-even at about 512 prescriptions per month if prescriptions have to carry the store alone. Payer mix, reimbursement, wholesale cost, and front-end sales like OTC remedies, wellness supplements, and immunizations can move that number fast.
What moves break-even
- Payer mix changes cash flow
- Reimbursement can cut margin
- Wholesale cost changes profit
- Processing fees add drag
What lowers script needs
- OTC sales add margin
- Wellness items boost basket size
- Immunizations bring extra revenue
- Local payer mix can shift fast
Want to see the six pharmacy income drivers?
1
18%-38%Prescription Volume
Every extra visitor can turn into more fills when conversion rises from 18% to 38% and 60% of new buyers come back.
2
4.0%-3.0%Reimbursement Mix
PBM and DIR fees fall from 4.0% to 3.0%, so cleaner reimbursement keeps more cash from each fill.
3
10.0%-8.0%Drug Margin
Wholesale drug and product cost drops from 10.0% to 8.0%, and better generic mix protects margin on prescription-heavy sales.
4
1.5-2.2Front-End Sales
Basket size rises from 1.5 to 2.2 units per order, so OTC, wellness, and immunizations add higher-margin dollars.
5
$1.975MLabor Model
Payroll can reach about $1.975M, so staffing levels and owner coverage decide how much gross profit stays with the owner.
6
$1.398MOverhead Load
Fixed costs total about $1.398M, and cash bottoms near $647K in month 6, so rent, systems, reserves, and debt service can squeeze take-home fast.
Pharmacy Core Six Income Drivers
Prescription Volume And Payer Mix
Prescription Volume and Payer Mix
Prescription volume lifts revenue, but payer mix decides how much cash reaches the owner. With 37,960 annual visitors and 18% buyer conversion, the model implies about 6,833 buyers a year. If prescriptions are 45% of sales mix at a $65 average price, more scripts only help when reimbursement clears drug cost, PBM fees, labor, and the cash tied up in inventory.
Here’s the quick math: commercial, Medicare Part D, Medicaid, and cash-pay claims can all pay differently and settle on different timelines. So script count per day is only half the story; the other half is prescription gross profit and repeat refill behavior. One clean line: more volume with weak reimbursement can raise work and cut owner draw.
Track Profit per Script
Measure scripts per day, gross profit per prescription, and days to cash by payer. That tells you whether volume is actually funding pay, rent, and inventory, or just creating busy work. A refill that comes back on time is more valuable than a one-off fill if it arrives with better spread and lower rework.
Use a simple test: compare commercial, Medicare Part D, Medicaid, and cash-pay claims on the same fill volume, then watch which mix leaves the best margin after acquisition cost and labor. If reimbursement falls below total fill cost, higher script count can still reduce owner income. Track refill rate, reject rate, and claim reversals every month.
- Track scripts per day.
- Track gross profit per script.
- Split results by payer.
- Watch refill repeat rates.
- Flag slow-paying claims early.
1
Reimbursement Rates, PBM Fees, And DIR Fees
Reimbursement Timing and PBM/DIR Fees
If payments land late or are trued up after the fill, strong script volume can still produce weak cash. In this model, 40% PBM (pharmacy benefit manager) and DIR (direct and indirect remuneration) fees hit Year 1, easing to 30% by Year 5, so a 1% swing moves about $84k on Year 1 revenue and about $891k on the simple Year 5 revenue estimate.
The key inputs are script count, payer mix, realized reimbursement, payment lag, and post-sale fee true-ups. Cash flow can fall before accounting profit does, which can squeeze owner pay if payroll, rent, and inventory must be covered first. Cash is the first place the gap shows up.
Track Net Cash by Payer
Build on-time, delayed, and lower reimbursement scenarios. Measure net collected per script after PBM and DIR fees, then compare it with drug cost and labor. If realized reimbursement slips, cut owner draw forecast first, because the cash hit shows up before the income statement tells the full story.
- Track days to payment.
- Separate fee true-ups.
- Reforecast owner pay monthly.
What this estimate hides is timing risk. A pharmacy can look busy and still miss cash targets if remittance arrives late or fees settle lower than expected, so the owner should watch collected margin, not just billed sales.
2
Generic Mix, Acquisition Cost, And Wholesaler Terms
Acquisition Cost And Generic Mix
This driver is the gap between script revenue and what the pharmacy pays to buy the drug. In this model, wholesale drug and product cost is 100% of revenue in Year 1, improving to 80% by Year 5. A 1% COGS change moves Year 1 profit by about $84k, so buying terms and mix change owner pay fast.
The risk is simple: not every generic has the same spread, and slow-moving stock ties up cash before it earns anything. If a product sits on the shelf, the business still carries rent, labor, and reimbursement timing. The owner’s take-home depends on how fast inventory turns and how much cash is left after product cost.
Track Turns And Terms
Measure inventory turns, dead stock, payment terms, and preferred wholesaler pricing every month. Here’s the quick math: better buying lowers cash tied up on shelves, but only if order size matches sell-through. If buying runs ahead of demand, cash gets trapped in inventory instead of flowing to payroll and owner draws.
- Track days on hand by item.
- Cut slow movers fast.
- Compare buy price by generic.
- Watch cash tied to stock.
Use item-level margin to drop weak generics and favor faster turns. A cheap drug can still hurt profit if fees, shrink, or stale stock wipe out the spread. The owner gets paid from cash left after product cost, so tighter buying usually helps more than chasing every discount.
3
Front-End Sales And Clinical Services
Front-End Sales and Clinical Revenue
Front-end and clinical sales give the pharmacy a second income stream beyond prescriptions. In Year 1, the mix includes 20% OTC remedies at $22, 20% wellness supplements at $38, and 15% immunizations at $55. By Year 5, supplements rise to 27% and immunizations to 20%, which can lift margin and spread risk if prescription reimbursement is thin.
The catch is cash timing. Immunization and other service revenue may face reimbursement delays, so the posted price is not always the cash collected. Track basket size, units per order, seasonality, and repeat use, because more front-end mix can support owner draw only if labor stays controlled and service cash comes in on time.
Measure the non-script basket
Use weekly sales by category and tie it to customer counts. If basket size rises while labor hours stay flat, more of each visit turns into gross profit instead of extra payroll. That matters most when prescription margins are pressured.
- Track OTC, supplement, vaccine sales.
- Measure units per order.
- Watch immunization season peaks.
- Compare repeat use by customer.
One clean test: compare front-end gross profit to service reimbursement lag. If vaccines sell well in season but cash settles late, working capital tightens and owner pay gets squeezed even when sales look strong.
4
Staffing Model And Owner-Pharmacist Involvement
Staffing And Owner Shifts
Payroll is the biggest controllable cost after drug margins. The disclosed line items add to $805k a year: $130k for the Pharmacist in Charge and 15 technicians × $45k = $675k. If the owner works shifts, near-term cash improves, but only until that labor has to be replaced.
Staff pharmacist coverage starts at 0.5 FTE (full-time equivalent) in Year 2 and reaches 1.5 FTE in Year 5, so staffing cost rises before the store is fully mature. Track overtime, scripts per labor hour, and burnout risk; if owner pay is really labor, not profit, it needs to be treated that way in the forecast.
Track Labor Per Script
Measure scripts per pharmacist hour, technician output, and overtime weekly. That tells you if staffing is too thin or if the owner is quietly subsidizing the business with unpaid labor. If technician productivity slips, labor cost climbs fast and owner draw falls with it.
- Count overtime by role.
- Review scripts per day.
- Separate owner labor from profit.
- Flag burnout before service slips.
5
Fixed Costs, Inventory Financing, Reserves, And Debt
Fixed Costs and Cash Available to the Owner
Accounting profit is not the same as cash the owner can take home. In Year 1, fixed costs total $1,165k per month, including $75k rent, $12k utilities, $800 pharmacy system fees, and $700 accounting and legal, plus other store costs. If reimbursement lags, inventory grows faster than sales, or debt payments and taxes hit first, owner draws can shrink fast.
This driver includes rent, software, overhead, loan payments, taxes, safety reserves, and the cash tied up in inventory on hand. The quick rule is simple: profit can look fine while cash is tight. If collections slow or stock builds, the pharmacy may need to delay owner distributions to protect working capital.
Track Cash, Not Just Profit
Watch days inventory on hand, reimbursement lag, and debt service every week. Those three items decide whether reported earnings become cash. Build a 13-week cash forecast, and set a minimum reserve before taking draws.
- Track inventory turns monthly.
- Separate tax cash from operating cash.
- Cap new stock until sales catch up.
- Delay owner pay when collections slip.
For this pharmacy, test what happens if reimbursement is delayed and inventory rises at the same time. That is the squeeze point where cash falls even though the income statement still shows a profit.
6
Compare low, base, and high pharmacy owner income cases
Owner income scenarios
Owner income moves with traffic, conversion, repeat use, mix, and reimbursement. In this model, payroll and fixed rent can squeeze take-home fast when visits slow.
| Scenario | Low CaseCash reserve risk | Base CaseModeled case | High CaseUpside cash strain |
|---|---|---|---|
| Launch model | Owner income stays near salary because traffic, conversion, and repeat fills run light. | Owner income tracks the model's base operating case and supports a healthy draw. | Owner income rises fast if repeat behavior, mix, and front-end sales all improve. |
| Typical setup | Weekday counts lag plan, repeat use is weaker, reimbursement is tighter, and payroll coverage eats most of the margin. | Year 1 lands at about $842k revenue, 90.0% gross margin, 84.5% contribution margin, $197.5k payroll, $139.8k fixed costs, and about $374k operating profit before debt, reserves, and taxes. | Traffic and conversion beat plan, repeat orders hold longer, prescription mix improves, COGS and fees stay lower, and front-end plus immunizations add more profit. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $130k - $175kSalary only | $340k - $400kCore case | $500k - $700kUpside case |
| Best fit | Use this to stress-test downside cash needs and a salary-only owner draw. | Use this as the planning case for lender, tax, and owner draw work. | Use this to test upside cash needs and a strong-growth owner draw. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Pharmacy Porter's Five Forces Analysis
- Pharmacy BCG Matrix
- Pharmacy Business Model Canvas
- 7 Core KPIs to Drive Pharmacy Profitability and Growth
- Pharmacy Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Pharmacy Profitability and Margin
- How Much Does It Cost To Run A Pharmacy Each Month?
- How Much Does It Cost To Open A Pharmacy? A $647K Startup Plan
- Pharmacy Financial Model Template in Excel
- How to Open an Independent Pharmacy: 6–12+ Month Launch Roadmap
- How to Write a Pharmacy Business Plan (7 Steps)
- Pharmacy Marketing Mix
- Pharmacy Marketing Plan
- Pharmacy Business Proposal
- Pharmacy PESTEL Analysis
- Pharmacy Pitch Deck Example Editable PPTX
- Pharmacy Business SWOT Analysis
- Pharmacy Value Proposition Canvas
Frequently Asked Questions
A pharmacy owner can plan around salary plus profit, not a guaranteed paycheck In the Year 1 assumptions, the Pharmacist in Charge salary is $130k, revenue is about $842k, and operating profit is about $374k before debt, reserves, and taxes Actual take-home depends on owner role, payer mix, and reinvestment needs