 Owner income$0
Owner income$0Physical Rehabilitation Owner Income: $0 In Year 1, Then Scale

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$0  Net margin-15%
Net margin-15% Revenue for target pay$425k
Revenue for target pay$425k Business difficultyHard
Business difficultyHard


You’re trying to see if this clinic can pay you, not just cover visits Based on the provided five-year model, first-year owner take-home should be planned at $0 because listed costs already leave a shortfall before therapist payroll, taxes, debt service, reserves, and reinvestment Results will change with payer contracts, staffing, market rent, collections, and whether the owner treats patients or manages the clinic
Owner income$0Net margin-15%Revenue for target pay$425kBusiness difficultyHardWant to test your owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only; it is not guaranteed salary, tax advice, or owner distribution advice.
Want to see the full Physical Rehabilitation clinic model?
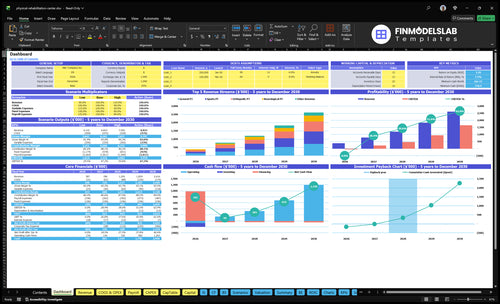
The Physical Rehabilitation Financial Model Template dashboard shows revenue, operating profit, cash flow, and owner take-home scenarios; open the model.
Owner-income model highlights
- Year 1/2/5 revenue: $387,360, $785,754, $2,616,084
- Costs: 14% variable, $16,300 fixed
- Owner pay: salary, distributions, reserves
How much profit can a physical rehabilitation center make?
A Physical Rehabilitation center can make little or no owner profit in Year 1, then move into meaningful distributions once visits, collections, and staffing are stable; track this through What Is The Most Critical Metric To Measure The Success Of Physical Rehabilitation Business?. In the researched case, Year 1 shows $387,360 revenue and about -$32,470 after listed costs but before therapist payroll, while Year 2 reaches $785,754 revenue and about $264,863 before clinician payroll and reserves.
Owner Economics
- Year 1 revenue: $387,360
- Year 1 pre-clinician result: -$32,470
- Year 2 revenue: $785,754
- Year 2 pre-clinician profit: $264,863
What Changes Take-Home
- Pay clinician wages first
- Hold reserves for cash gaps
- Cover debt before distributions
- Push utilization across providers
How does payer mix affect rehab clinic owner income?
Payer mix changes owner income because you get paid on collected revenue, not billed charges; if you’re sizing startup costs, use How Much Does It Cost To Open And Launch Your Physical Rehabilitation Business? as the baseline. In Physical Rehabilitation, treatment prices run from $120 to $160 in Year 1 and $140 to $180 in Year 5, and weighted revenue per completed visit rises from about $137 to $158. Billing and collection fees fall from 40% to 30% of revenue, but Medicare, commercial insurance, workers’ compensation, cash-pay, denials, and delays can still shift cash timing, so model sensitivity instead of payer-rate promises.
Revenue math
- $120-$160 Year 1 price band
- $140-$180 Year 5 price band
- $137 per completed visit in Year 1
- $158 per completed visit in Year 5
Cash risk
- Fees drop from 40% to 30%
- Medicare can slow payment timing
- Commercial rates vary by contract
- Denials and delays hit collections
How many patients does a rehab clinic need to pay the owner?
For Physical Rehabilitation, the real answer is completed visits, not patient count, because one patient can attend several visits and cancellations cut revenue. With $30,467 in monthly fixed overhead plus support payroll, $13,692 collected per completed visit, and 86% contribution after variable costs, break-even before therapist payroll is about 259 completed visits per month. The model is at about 236 completed visits, so it is short before owner pay, and every extra $1,000 of monthly owner pay needs about 85 more completed visits at Year 1 economics.
Use visits, not patients
- 259 visits breaks even before therapist pay
- 236 visits is the current model
- One patient can create many visits
- Cancellations directly reduce revenue
Owner pay math
- $30,467 monthly fixed overhead plus support payroll
- $13,692 collected per completed visit
- 86% contribution after variable costs
- $1,000 more pay needs about 85 more visits
Want the six drivers that move owner pay?
1
236/moVisit Volume
At 236 completed visits a month in Year 1, every filled slot adds direct revenue, so volume is the main income lever.
2
$137/visitCollections Rate
At $137 collected per visit, cleaner billing and better reimbursement raise cash without adding many extra hours.
3
40%-65%Utilization Mix
A 40% to 65% capacity range shows how much income improves when clinician time is filled instead of idle.
4
14%Leakage Control
Missed visits and authorization delays add to the 14% variable-cost drag, so tighter scheduling protects margin.
5
$163K/moFixed Overhead
$163K a month in fixed overhead sets the cash floor, so steady throughput is what protects owner take-home.
6
5 specialtiesReferral Flow
Five specialties broaden referral paths and help keep new patient flow steadier across the clinic.
Physical Rehabilitation Core Six Income Drivers
Completed Visit Volume
Completed Billable Visits
Income rises when patients complete billable visits, not when they inquire. Year 1 runs at about 236 completed visits per month, or 54 per week, and Year 5 reaches 1,379 per month, or 318 per week. At about $117.75 contribution per Year 1 visit before fixed payroll and overhead, each extra completed visit lifts owner income fast.
This driver includes evaluations, follow-up adherence, and schedule fill. The key input is the completed-to-scheduled visit rate; if staffing is stretched or slots are overbooked, care quality drops and the gain can fade. If the clinic keeps visits flowing without waste, cash and profit improve before the owner draws pay.
Raise Visit Completion
Track scheduled visits, completed visits, cancellations, and no-shows each week. Use completed visits ÷ scheduled visits to see where revenue leaks. In a Year 1 model, even small losses hurt because the clinic is still close to break-even before payroll and overhead.
- Fill follow-ups before new starts.
- Review no-shows by therapist.
- Do not overbook beyond safe staffing.
1
Reimbursement And Collections
Collected Revenue Per Visit
Use collected revenue per visit, not billed charges. The model shows weighted revenue per completed visit of $13,692 in Year 1 and $15,813 in Year 5, with service prices from $120 to $160 in Year 1. Billing and collection fees equal 40% of revenue in Year 1 and 30% in Year 5, so denials, payer rules, delayed authorizations, and contract adjustments directly cut cash available for payroll and owner pay.
Here’s the quick math: at 236 monthly visits, a $10 swing in collection per visit changes revenue by about $2,360 per month. That’s enough to move the clinic from thin profit to real draw money. What this estimate hides: if cash posting lags, reported revenue can look fine while the bank balance stays tight.
Measure Net Cash Fast
Track cash collected per completed visit, denial rate, authorization lag, and contract adjustment write-offs every month. Compare billed charges to cash received, then fix the biggest leak first. If payer rules are the issue, tighten pre-auth checks; if denials are the issue, clean up documentation and coding before claims go out.
- Watch cash per visit weekly.
- Audit denials by payer.
- Post collections daily.
- Forecast owner draw from cash, not charges.
Price changes matter, but collection quality matters just as much. A clinic with strong visit volume still starves if 40% of revenue gets lost to billing and collection costs in Year 1. Cut that drag, and more of each completed visit turns into usable cash for rent, payroll, and the owner’s paycheck.
2
Clinician Utilization And Labor Cost
Clinician Utilization
Profit rises when therapists stay busy with completed visits and payroll grows only as demand grows. In Year 1, service capacity runs at 40% to 65%; by Year 5, it moves to 70% to 85% as the clinic scales from 5 therapists to 20 therapists. If schedules lag, labor becomes idle cost and owner draw gets squeezed.
Here’s the quick math: every extra filled slot must cover therapist pay plus support staff, including a $90k clinic manager, $45k administrative assistant, and $35k receptionist. Hiring ahead of demand hurts cash flow fast, while safe visit loads and care quality protect margin and keep revenue per visit from leaking into overtime and wasted payroll.
Track Utilization Weekly
Track booked hours, completed visits, no-shows, and visits per therapist every week, then compare them to service capacity by year. Use the same report to test whether each therapist’s load stays inside safe limits at 40% to 65% in Year 1 and 70% to 85% in Year 5. That tells you when labor is earning its keep.
Payroll should follow demand, not hope. Add support staff only when completed volume can absorb them, and keep wage structure aligned with collection timing so cash does not get trapped in front-loaded headcount. One empty schedule slot is not just lost revenue; it also raises labor cost per visit and cuts the cash left for owner pay.
3
Cancellations And Authorization Leakage
Cancellations And Authorization Leakage
Missed visits cut revenue fast because rent, admin payroll, and therapy staff still run. In Year 1, the clinic has about 236 completed visits per month but needs roughly 259 just to cover listed fixed and support costs before therapist payroll, so even a small no-show or late-authorization leak can push owner income down.
Include same-day cancellations, care-plan drop-off, and late authorizations in the loss rate. Use an editable no-show percentage on scheduled visits, not completed visits, so the forecast shows the real cash hit before revenue is booked.
Track leakage before it hits pay
Measure scheduled visits, completed visits, and the gap between them every week. Here’s the quick math: if scheduled slots rise but completions stay flat, the owner still pays the same overhead while take-home income shrinks. The model should let you stress test the no-show rate month by month.
Use a short control list: authorization status, confirmation calls, reschedule speed, and unused therapist time. If leakage rises in ramp-up months, fix the process fast, because each lost visit makes it harder to cover the monthly cost base and delays owner pay.
- Set an editable no-show rate.
- Apply it to scheduled visits.
- Track authorizations daily.
- Rebook canceled slots fast.
4
Facility And Equipment Overhead
Fixed Facility Overhead
Facility and equipment overhead is the monthly cash load the clinic must cover before owner pay. Here it totals $16,300 per month or $195,600 per year: $10,000 lease, $1,500 utilities, $2,000 insurance, $800 software, $500 office supplies, $300 licenses, and $1,200 maintenan ce and cleaning.
At 236 completed visits per month in Year 1, that fixed load is about $69 per visit before therapist payroll and owner draw. At 1,379 visits per month in Year 5, it falls to about $12 per visit. The risk is simple: too much space too early, while utilization is still low.
Track Space Cost per Visit
Measure this using lease, utilities, insurance, software, office supplies, licenses, and maintenance, then divide by completed visits. Keep startup buildout and equipment recovery out of the monthly operating run rate so you do not hide the real hurdle.
Watch utilization every month. If visits lag, fixed overhead eats more of each dollar collected, which squeezes cash and owner pay. The clean control is space size: match square footage and support costs to the visit volume you can fill now, not the volume you hope to reach later.
5
Referral Pipeline And Patient Acquisition
Referral Pipeline
Referral pipeline is the flow of physician, post-surgery, discharge, and local-reputation referrals that turn into authorized visits. Volume rises from 54 visits per week in Year 1 to 318 visits per week in Year 5, so demand has to scale with staff or the clinic will carry empty slots, weaker collections, and lower owner pay.
The key input is completed visits, not lead count. Track source mix, authorization rate, and completed-visit collections by payer and source. If leads do not turn into visits, marketing spend becomes dead cash flow instead of revenue.
Improve Referral Conversion
Measure each referral source by completed visits and collections, then rank it by conversion. Physician referrals, post-surgical demand, discharge relationships, and community visibility should earn more spend only when they fill the calendar.
Use a weekly dashboard for referrals, authorized visits, cancellations, and schedule fill. Cut channels that create inquiries but not visits; that protects margin and keeps payroll aligned with actual demand.
6
Compare low, base, and mature owner-income scenarios
Owner income scenarios
Owner income moves with visit volume, pricing, and staffing. Early losses can happen even when demand is rising because fixed payroll and facility costs hit first.
| Scenario | Low CaseDownside case | Base CasePlan case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is a Year 1 ramp case where owner income stays negative because visit volume is still low and fixed costs hit early. | This is the modeled run-rate case where owner income turns positive as visit volume spreads fixed costs across more treatments. | This is the stronger earnings path where a fuller clinic and better pricing drive the highest operating surplus in the model. |
| Typical setup | The clinic runs about 236 visits a month, 54 a week, and $32,280 in monthly revenue at $136.92 per visit, with 40% to 65% capacity and about 14% variable costs. | The clinic runs about 463 visits a month, 107 a week, and $65,480 in monthly revenue at $141.52 per visit, with 13.4% variable costs and a stronger operating surplus. | The clinic reaches about 1,379 visits a month, 318 a week, and $218,007 in monthly revenue at $158.13 per visit, with 11% variable costs and mature capacity. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | -$59k/yearCautious start | $223k/yearCore plan | $1.65M/yearFull schedule |
| Best fit | Use this to stress-test cash needs if referrals start slow or hiring comes before the schedule fills. | Use this as the normal planning case for steady ramp, solid utilization, and controlled overhead. | Use this to test upside if the clinic reaches mature utilization and pricing holds. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Physical Rehabilitation Porter's Five Forces Analysis
- Physical Rehabilitation BCG Matrix
- Physical Rehabilitation Business Model Canvas
- Tracking 7 Core KPIs for Physical Rehabilitation Success
- Physical Rehabilitation Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Physical Rehabilitation Profitability
- Analyzing the Running Costs for Physical Rehabilitation Clinics
- Physical Rehabilitation Center Startup Costs: $125K CAPEX Plan
- Physical Rehabilitation Financial Model Template in Excel
- How To Open A Physical Rehabilitation Center In 4–9 Months
- How to Write a Physical Rehabilitation Business Plan: 7 Key Steps
- Physical Rehabilitation Marketing Mix
- Physical Rehabilitation Marketing Plan
- Physical Rehabilitation Business Proposal
- Physical Rehabilitation PESTEL Analysis
- Physical Rehabilitation Pitch Deck Example Editable PPTX
- Physical Rehabilitation Business SWOT Analysis
- Physical Rehabilitation Value Proposition Canvas
Frequently Asked Questions
Plan for $0 owner take-home in the first year under the provided assumptions The clinic generates $387,360 of revenue, but 14% variable costs, $195,600 fixed overhead, and $170,000 listed support payroll leave about -$32,470 before therapist payroll, taxes, reserves, debt service, or owner distributions