 Owner income$120k–$361.8k
Owner income$120k–$361.8kHow Much Does A Physical Therapist Owner Make? $120K-$362K Model

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$120k–$361.8k  Net margin-32% to 3%
Net margin-32% to 3% Revenue for target pay$1.43M
Revenue for target pay$1.43M Business difficultyHard
Business difficultyHard


A physical therapist owner in this model can plan around $120,000 of salary in the first year, with no supported profit draw because EBITDA is about -$100,900 after payroll, fixed costs, and visit-related expenses By the third year, modeled revenue reaches about $143 million, EBITDA reaches about $241,800, and owner pay capacity before taxes, debt, and reserves can reach about $361,800 if the owner is also the lead clinician These are researched assumptions, not guaranteed earnings Visits, payer mix, payroll, rent, billing fees, and reinvestment decide the real take-home
Owner income$120k–$361.8kNet margin-32% to 3%Revenue for target pay$1.43MBusiness difficultyHardWant to test your PT owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on patient volume, payer mix, payroll, taxes, debt, and reserve needs.
Want to stress-test a Physical Therapist clinic financial model?
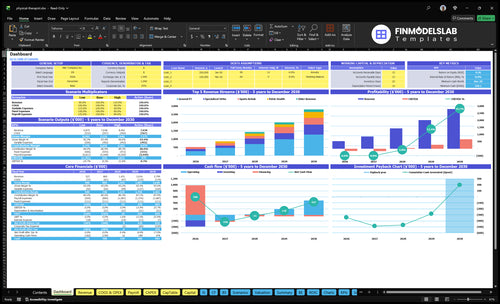
Open the Physical Therapist Financial Model Template to check revenue, EBITDA, owner salary, profit draw capacity, visits, utilization, payroll, and fixed costs. Assumptions cover therapist count, monthly treatments, price, capacity, COGS, marketing, EHR, wages, and rent; revenue grows from $43,880 to $119,282 by Year 3. Start with the income guide, then use this as the next step.
Owner-income model highlights
- Owner salary and draw
- Revenue, EBITDA, visits
- Year 3 growth case
Do physical therapy practice owners make more than staff PTs?
Not always: in this Physical Therapist model, staff pay is $85,000 for a General Physical Therapist, $95,000 for a Specialized Physical Therapist, and $120,000 for a Clinic Director / Lead PT, while the owner only makes more if profit remains after payroll, overhead, billing, marketing, reserves, and debt; track that with What Is The Most Critical Indicator Of Success For Your Physical Therapist Business?. Year 1 EBITDA is about -$100,900, so ownership adds risk before upside; by Year 3, EBITDA reaches about $241,800.
Staff Pay
- General Physical Therapist: $85,000
- Specialized Physical Therapist: $95,000
- Clinic Director / Lead PT: $120,000
- Lower upside, lower operating risk
Owner Upside
- Year 1 EBITDA: -$100,900
- Year 3 EBITDA: $241,800
- Profit must clear all major costs
- Upside starts after the clinic stabilizes
What is a good profit margin for a physical therapy clinic?
A good margin depends on whether you mean gross collections or operating profit; in this model, visit-related costs are 15% in Year 1, but payroll, rent, billing fees, no-shows, payer collections, and admin support can still push EBITDA margin to -192%. For startup cost context, see How Much Does It Cost To Open A Physical Therapist Business?. By Year 3, the model reaches 975 visits per month and $143 million revenue, with 169% EBITDA margin, so the real lever is overhead control.
Year 1 economics
- 15% visit-related costs
- -192% EBITDA margin
- Payroll drives the gap
- Billing and no-shows matter
Year 3 upside
- 975 visits per month
- $143 million revenue
- 169% EBITDA margin
- Fixed costs get spread out
How much revenue does a physical therapy clinic need to pay the owner?
A Physical Therapist clinic does not have one universal revenue target; it depends on the owner’s pay goal. With $317,500 in Year 1 non-owner payroll, $111,000 in fixed overhead, and 15% visit-related costs, the clinic needs about $621,800 in annual revenue to pay the owner $100,000, or $645,300 for $120,000. At about $116.70 per visit, that works out to roughly 444 to 461 visits per month before reserves and debt.
Owner pay math
- $100,000 owner pay needs $621,800
- $120,000 owner pay needs $645,300
- 15% visit costs scale with revenue
- 0.85 × revenue covers the rest
Volume check
- At $116.70 per visit, volume matters
- Need about 444 to 461 visits monthly
- That is before reserves and debt
- Higher payroll means more visits to break even
Want to see the six PT income drivers?
1
376-975/moVisit Volume
At 376-975 monthly visits, more appointments are the cleanest way to spread fixed costs and lift owner take-home.
2
$110-$142Net Price
A $110-$142 treatment price raises cash per visit before supply, billing, and labor costs.
3
60%-75%Clinician Utilization
At 60%-75% early utilization, every empty hour is lost revenue, so schedule fill turns staff time into profit.
4
$9.25KFixed Overhead
With $9.25K of fixed overhead each month, rent, insurance, software, and admin hit EBITDA fast if volume slips.
5
6%-4%Referral Flow
Better referrals and fewer no-shows can pull marketing spend from 6.0% toward 4.0% of revenue.
6
$663KOwner Role
The owner's mix of patient care and management decides how much of that Year 5 EBITDA turns into take-home.
Physical Therapist Core Six Income Drivers
Patient Volume And Capacity
Patient Volume And Capacity
Patient volume is the main revenue engine here. The model shows 376 monthly visits and $43,880 in monthly revenue in Year 1, then 975 visits and $119,282 by Year 3. That jump only helps if visits are actually completed and billed, because empty slots and late cancels still leave therapist payroll on the books.
Capacity matters as much as demand. Several service lines rise from 60% to 75% capacity, so the owner’s income improves when the clinic fills more of each therapist’s schedule without adding the same level of labor cost. One clean rule: track billed visits, not booked appointments.
Measure Billed Visits Weekly
Track the gap between booked, completed, and billed visits every week. If cancellations rise, collections fall fast even when therapists are fully scheduled, so the clinic can look busy while cash stays weak. Here’s the quick math: 376 visits at $43,880 is far less cash than 975 visits at $119,282, so small fill-rate gains matter.
- Completed billed visits, not bookings
- No-show rate by therapist
- Schedule fill rate by service line
- Capacity at 60% and 75%
- Open slots left each week
If capacity moves from 60% to 75%, revenue can rise without a matching jump in fixed cost, which improves cash flow and gives the owner more room to pay themselves. If slots stay open, payroll keeps running and margin gets squeezed.
1
Net Revenue Per Visit And Payer Mix
Net Revenue Per Visit
Net revenue per visit is what the clinic actually collects for each completed PT visit after denials and payment delays. Modeled treatment prices run from $110 for General PT in Year 1 to $142 for Pelvic Health in Year 5, but payer mix across Medicare, commercial insurance, cash pay, workers’ comp, and self-pay decides what the owner really keeps.
Here’s the quick math: at 376 monthly visits, every $5 change in net collection per visit moves monthly revenue by about $1,880 (376 × $5). That can change cash for payroll, rent, and owner draw fast, so listed prices are not reimbursement guarantees.
Track Collections By Payer
Measure collected revenue per completed billed visit by payer and service line, not just posted charges. Also track denial rate, days to collect, and write-offs, because those are the gaps between a strong fee schedule and real cash.
- Split collections by payer.
- Use completed billed visits.
- Watch denials and delays.
- Forecast owner draw monthly.
If Medicare or other lower-paying payers take a bigger share, net revenue per visit falls even when visit count holds. Tight claims work, cleaner authorizations, and payer-aware pricing protect profit and make owner pay more predictable.
2
Clinician Productivity And Payroll Leverage
Payroll Leverage
Payroll is the biggest cost, so owner pay rises only when completed visits grow faster than wages. With Year 1 wages at $437,500—about $36,458 per month—the clinic needs enough billed visits to cover therapists, assistants, admin, billing, and marketing before the owner sees much draw. If revenue stays flat, each new FTE lowers margin.
This driver includes visits per therapist per day, utilization rate (paid time filled with visits), cancellations, and support staffing. Here’s the catch: a packed schedule that misses visits or uses unsafe productivity targets can still hurt collections and quality. At modeled Year 1 revenue of $43,880 per month, wages alone absorb about 83% of annual revenue, so small inefficiencies hit cash fast.
Track Visits Per Paid Hour
Track completed billed visits, not booked slots, then compare them to payroll each month. The best check is visits per therapist per day by provider, plus cancellation rate and no-show recovery. If visits do not rise faster than payroll, gross margin narrows and the owner’s take-home pay drops, even if the schedule looks full.
Use support staff to protect therapist time. Good admin, billing, and reminders can lift completed visits without forcing noncompliant quotas. Test staffing changes in small steps; if a new hire does not increase completed visits and collections, payroll leverage gets worse and cash flow tightens before the owner can pay themselves.
3
Overhead Cost Structure
Fixed Overhead Burn
$9,250 a month comes off the top before the first visit, so this clinic starts with a real cash hurdle. That fixed burn includes $5,000 rent, $1,200 liability insurance, $800 utilities, $700 accounting and legal, $600 maintenance, $400 EHR, $300 supplies, and $250 telecom. One clean line: fixed overhead is paid whether the schedule is full or not.
Here’s the quick math: fixed overhead alone is $111,000 a year. On top of that, Year 1 also carries visit-linked costs like 45% billing fees and 60% marketing, so owner take-home depends on both volume and collection quality. If completed visits slip, overhead stays put and profit drops fast.
Separate Fixed Burn From Visit Costs
Track fixed overhead and visit-linked costs in different buckets. Fixed burn should stay near $9,250 unless rent, insurance, or software changes. Billing fees and marketing should be tied to collected revenue, not booked visits, so you can see the real margin after denials, delays, and no-shows.
Use a simple monthly check: completed billed visits, collected revenue, billing fee dollars, and marketing dollars. If volume rises but owner pay does not, the issue is usually overhead absorption, not demand. Keep one eye on rent and insurance, but make sure variable spend scales with actual collections.
- Watch fixed burn monthly.
- Track collected, not booked visits.
- Separate billing fees from rent.
- Cap marketing to revenue.
4
Referrals, Retention, And No-Shows
Referrals, Retention, No-Shows
This driver is about how ma ny completed billed visits you actually collect from direct access, physician referrals, online reviews, and repeat patients. In Year 1, the model needs about 461 visits per month to cover payroll, fixed overhead, and 15% visit costs, but it starts at 376. That gap matters because payroll and rent still hit even when visits cancel.
Track Completed Visits First
Measure booked visits, completed visits, and no-show rate every week, then split them by referral source. If the schedule fills but visits don’t happen, cash flow drops fast and owner pay gets squeezed. One clean rule: filled schedules do not pay bills; completed visits do.
- Track booked-to-completed visits.
- Count referrals by source.
- Watch plan completion rates.
- Call to reduce no-shows fast.
Here’s the quick math: at 376 visits, you are about 85 visits short of break-even. Better retention and fewer no-shows move you toward that line without adding rent or payroll, while weak referral flow or poor follow-up pushes owner income down even if the clinic looks busy.
5
Owner Role And Scale
Owner Clinical Hours
If the owner is also the Clinic Director / Lead PT at $120,000, those clinical hours can cover early payroll and help fund take-home pay before the schedule is full. The catch is simple: owner hours only help if completed billed visits stay ahead of labor and fixed overhead, not just booked slots.
Scale adds capacity, but it also adds risk. By Year 3, the plan reaches 4 General PTs, 2 Specialized Ortho, 1 Sports Rehab, 1 Pelvic Health, and 1 Pediatric PT. That can raise revenue, but it also brings more payroll, billing, hiring, and cash-flow pressure, so scale is a choice, not an automatic win.
Measure Hours Against Collected Visits
Track completed billed visits per owner hour, plus utilization, cancellations, and collections per visit. Those inputs tell you whether the owner’s clinical time is producing enough cash to support salary, staff payroll, and overhead.
Use the forecast to test each hire or specialty. If added therapists do not lift collected revenue faster than payroll and billing load, owner pay gets squeezed. One clean rule: grow only when the extra clinician’s visits can cover their pay and the support cost around them.
- Track completed visits, not booked slots.
- Watch no-shows and open gaps weekly.
- Compare revenue added to payroll added.
- Stress-test cash before adding specialties.
6
Compare low, base, and high PT owner income scenarios
Owner income scenarios
Year 1 and Year 2 still run negative EBITDA, so owner income stays close to salary. By Year 3, higher visit volume can start supporting a real draw.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | This is the thin-cash opening case, so owner income is basically salary only. | This is the Year 2 case, where volume improves but owner income is still tight. | This is the stronger Year 3 case, where higher volume starts to support owner draw. |
| Typical setup | Year 1 runs about 376 visits a month, $526,560 in annual revenue, and negative EBITDA, so there is no profit draw. | Year 2 reaches about 604 visits a month, $864,957 in annual revenue, and EBITDA is still negative, so salary stays the main owner pay. | Year 3 reaches about 975 visits a month, about $1.43M in annual revenue, and positive EBITDA, so owner pay can rise above salary. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $120,000Low case | $120,000Base case | $361,800High case |
| Best fit | Use this if you want to stress-test launch-year pay when the clinic is still loss-making. | Use this for a more normal early operating year with no profit draw yet. | Use this to test upside pay if volume, pricing, and staffing all hold together. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distribution forecasts.
Related Products
- Physical Therapist Porter's Five Forces Analysis
- Physical Therapist BCG Matrix
- Physical Therapist Business Model Canvas
- 7 Essential KPIs to Maximize Profit for Your Physical Therapist Practice
- Physical Therapist Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Physical Therapist Profitability
- How Much Does It Cost To Run A Physical Therapist Practice Monthly?
- Physical Therapy Clinic Startup Costs: $205K CAPEX Plan
- Physical Therapist Financial Model Template in Excel
- How to Start a Physical Therapy Practice in 3 to 9 Months
- How to Write a Physical Therapist Business Plan: 7 Steps to Financial Clarity
- Physical Therapist Marketing Mix
- Physical Therapist Marketing Plan
- Physical Therapist Business Proposal
- Physical Therapist PESTEL Analysis
- Physical Therapist Pitch Deck Example Editable PPTX
- Physical Therapist Business SWOT Analysis
- Physical Therapist Value Proposition Canvas
Frequently Asked Questions
In this model, owner pay starts with a $120,000 Clinic Director / Lead PT salary The first year does not support an added profit draw because EBITDA is about -$100,900 By Year 3, EBITDA reaches about $241,800, so total owner pay capacity can reach about $361,800 before taxes, debt, reserves, and reinvestment