 Owner income≈$669K
Owner income≈$669KHow Much Posture Correction Owners Make: $67K To $326M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income≈$669K  Net margin79%–84%
Net margin79%–84% Revenue for target pay≈$847K
Revenue for target pay≈$847K Business difficultyHard
Business difficultyHard


A posture correction services owner can make little in the first year if the clinic is overstaffed, even with solid sales Here’s the quick math: Year 1 revenue is about $48,035/month, but 21% direct and variable costs, $17,000/month fixed overhead, and non-owner payroll leave about $66,900 before owner pay and reserves Paying the planned $145,000 CEO salary would put EBITDA near negative $78,100 in Year 1 By Year 5, the same model reaches about $385,000/month in revenue and $312M EBITDA after listed payroll, before taxes, reserves, debt, or owner distributions
Owner income≈$669KNet margin79%–84%Revenue for target pay≈$847KBusiness difficultyHardWant to test your owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on revenue, margins, payroll, taxes, debt, and reinvestment.
Want to check owner income in the Posture Correction Services model?
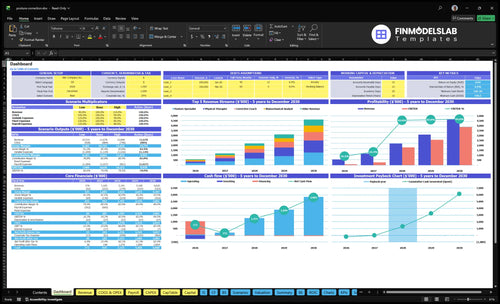
This Posture Correction Services Financial Model Template shows revenue, margin, costs, reserves, and owner take-home assumptions—open the model.
Owner-income model highlights
- Owner pay stays visible
- Revenue scales fast
- Scenarios test EBITDA swing
What posture correction business expenses reduce profit margin?
In Posture Correction Services, profit gets squeezed first by payroll and rent: Year 1 fixed overhead is $17,000/month, with $12,000 rent as the biggest fixed line and $329,500/year payroll, including a $145K CEO and Clinical Director salary. The variable load is another 21% of revenue, split across 6% device inventory, 3% diagnostic software, 9% lead acquisition, and 3% merchant fees; see What Are The 5 KPI Metrics For Posture Correction Services? for the main KPI set. Payroll and utilization decide the owner’s check.
Big fixed costs
- $12,000 monthly rent is the largest fixed line.
- $17,000/month fixed overhead sets the floor.
- $329,500/year payroll drives cash burn.
- Missed appointments waste paid staff time.
Variable margin leaks
- 21% of revenue goes to direct and variable costs.
- 9% lead acquisition pressure hits margin fast.
- 6% device inventory and 3% software add drag.
- 3% merchant fees stack on every payment.
How do solo and staffed posture correction models compare?
Posture Correction Services can be more profitable on a solo model because payroll and rent stay light, but the owner’s calendar caps revenue. A staffed clinic can scale much bigger, from $48,035/month in Year 1 to $385,000/month in Year 5, but it adds payroll, scheduling risk, and management work. Mobile service cuts rent but loses capacity to travel time, while leased clinics improve referrals and client experience but raise break-even pressure.
Solo model
- Higher margin with lean payroll
- Lower rent keeps fixed costs down
- Owner calendar caps revenue
- Best when demand is steady
Staffed and location models
- $48,035/month in Year 1
- $385,000/month by Year 5
- More scale but more payroll
- Leased clinics lift referrals, but raise break-even
How many posture correction clients to make owner income?
Posture Correction Services can’t safely pay a full $145K owner salary yet. Here’s the quick math: after 21% direct and variable costs, Year 1 contribution is about $37,948/month, then $17,000 fixed overhead and $15,375 non-owner payroll leave only $5,573/month, or about $66,900/year, before reserves. So the owner pay target is a planning output, not a guaranteed salary; to close the gap, the clinic needs more volume, better utilization, higher average revenue per client, lower payroll load, or a reserve-funded ramp.
Current owner pay gap
- $37,948 monthly contribution
- $17,000 fixed overhead
- $15,375 non-owner payroll
- $5,573 left for owner pay
What changes the math
- Increase client volume
- Raise utilization rates
- Lift revenue per client
- Cut payroll load or use reserves
Want the six owner income drivers?
1
$576K-$4.62MQualified Assessments
More paid assessments feed every later sale, so this is the first gate to revenue and owner take-home.
2
HighPackage Conversion
Turning more assessments into treatment packages lifts revenue fast without adding the same amount of fixed cost.
3
$85-$200Treatment Pricing
The mix across services sets revenue per client and margin, so price and service mix move income fast.
4
45%-85%Provider Utilization
Higher therapist fill rates spread payroll across more sessions, and empty slots drag earnings down.
5
HighAdd-On Revenue
Device sales and follow-up work add margin after the first visit, so attach rate matters.
6
$17K/moOverhead Control
With about $17K of fixed overhead and 16%-21% direct plus variable cost, marketing efficiency and cash reserves decide how much income stays in the business.
Posture Correction Services Core Six Income Drivers
Qualified Assessments Booked
Qualified Assessments Booked
Booked assessments are the first real filter in a posture correction clinic. A booked visit only helps income if the person has a clear pain point, budget, and time to start care. More qualified bookings feed treatment plans, follow-ups, and device recommendations; weak bookings just fill the schedule with low-fit traffic.
Here’s the quick math: if show-up rates slip, provider utilization falls, and owner pay gets squeezed. That matters with $17,000/month in fixed overhead, plus 9% lead acquisition cost and 3% merchant fees. Better booked quality matters more than raw website traffic because attendance and plan fit drive actual revenue.
Track booked quality, not just volume
Measure booked consultations, show-up rate, referral source, and assessment-to-plan fit by provider. The best source is the one that sends people ready to act, not just people who clicked. A small list of qualified bookings usually beats a big list of low-intent leads.
- Track show-up rate by source
- Compare started plans by provider
- Drop low-fit referral channels fast
Use referral partners like fitness providers, employers, wellness partners, and healthcare-adjacent professionals. If booked assessments stay strong, calendars fill, and utilization can move toward the Year 1 range of 45% to 60%. If they weaken, fixed costs stay the same but profit and owner draw fall.
1
Package Conversion Rate
Package Conversion Rate
Package conversion rate is the share of assessments that turn into paid treatment plans. For a posture clinic, that is where cash starts, because booked assessments don’t pay rent until they convert. Higher conversion lifts revenue per lead, improves provider utilization, and helps cover the fixed $17,000/month overhead without adding more marketing.
Here’s the quick math: if assessment volume stays flat, better conversion raises paid plan count, so gross margin and owner draw rise faster than ad spend. Weak conversion does the opposite, since you still pay the 9% of revenue lead cost and 3% merchant fees while empty follow-up slots and device sales never materialize.
Track the handoff, not just the booking
Measure conversion by provider, service type, and lead source. The useful inputs are booked assessments, show-up rate, plan price, session cadence, home exercise support, reassessment timing, and expected functional goals without cure claims. Plans that explain next steps in plain English usually sell better than vague promises.
Test one script, one offer, and one follow-up cadence at a time. If conversion slips, the clinic can look busy but still lose cash because capacity is underused. Track the share of assessments that buy a plan, then compare it with revenue per client and the hours filled next week.
- Watch conversion by provider weekly.
- Split results by lead source.
- Review lost assessments within 48 hours.
- Standardize cadence and reassessment timing.
2
Average Revenue Per Client
Package Pricing per Client
Average revenue per client is the money collected per paying posture correction client, so it depends on the mix of assessments, multi-session plans, follow-ups, memberships, and add-ons. In Year 5, source treatment prices range from $85 for corrective coaching to $200 for biomechanical analysis, so the package mix can move revenue a lot without changing client count.
Here’s the quick math: ARPC = total revenue ÷ paying clients. If clients only buy the lower-priced visit, owner pay stays tight; if more clients move into higher-value plans, cash flow and profit improve. The catch is simple: higher prices help only when clients understand the plan and providers deliver the same result every time.
Test Price Against Completion
Track conversion, refunds, and completion rates by service type, because price changes can lift revenue but hurt volume if the offer feels unclear. Test each change against the full client path: assessment, plan acceptance, follow-up booking, and membership take-up.
- Price the plan, not one visit.
- Watch revenue per completed client.
- Check if refunds rise after changes.
- Compare results by provider and service.
- Keep add-ons ethical and tied to need.
If a higher price raises ARPC but cuts completion, the owner may see less real income after idle capacity and rework. The better test is whether each client leaves with a clear plan, stays on it, and buys the next step without confusion.
3
Provider Utilization And Capacity
Provider Utilization
Utilization is the share of bookable provider time that gets paid. In posture correction, that means assessments, therapy sessions, and follow-ups that actually show up and get billed. Year 1 is often only 45% to 60%; by Year 5, a tighter schedule can reach 75% to 85%. Lower use means weaker revenue and wasted wage capacity. One clean rule: empty slots do not pay owner income.
Here’s the quick math: revenue depends on available hours × utilization × price per session. For owner-led work, those hours are partly labor pay. For staffed delivery, profit only appears after wages and overhead. If no-shows rise or calendars stay thin, the clinic can look busy but still leave the owner with less cash to draw.
Measure Booked Time
Track booked assessments, kept appointments, no-show rate, and filled provider hours by service line. Also watch whether the mix leans toward biomechanical analysis or physical therapy, since Year 1 capacity can differ from 45% to 60%. That tells you where calendars are underfilled and where staffing is too early. If utilization falls, cut back hours before payroll eats margin.
Use standard session lengths and simple scheduling rules to protect margin. Standardized visits make it easier to forecast cash, reduce gaps between clients, and compare each provider’s output against pay. If one provider sits below target while another is overbooked, rebalance hours fast. The owner’s draw gets safer when each hour billed is close to each hour staffed.
4
Device Add-Ons And Follow-Up Revenue
Device Add-Ons and Follow-Up Revenue
Devices can lift client value, but they are still secondary to the service model. The direct cost load is modest at 6% of revenue in Year 1, falling to 5% by Year 5, but that does not include returns, storage, compliance, or extra staff time. If follow-up plans do not improve adherence, they can add work without lifting owner pay.
Here’s the quick math: on $10,000 of device and add-on revenue, device COGS is about $600 in Year 1 and $500 by Year 5. That still leaves margin pressure from handling and check-ins. The driver helps only when repeat visits and maintenance plans create profitable recurring revenue, not just more inventory on hand.
Measure Attach Rate and Repeat Visits
Track client count, device attach rate, follow-up visit rate, price per add-on, and time per session. If the device sale or maintenance plan does not raise retention, it is not helping. Sell only what improves adherence and can still cover product cost plus the extra service time.
- Price above 6% COGS
- Watch returns and spoilage
- Bill check-ins separately
- Keep inventory tight
Sell support, not shelfware. If follow-up revenue smooths cash flow and keeps clients on plan, it can raise gross profit and make owner draws steadier. If it creates admin, storage, and compliance drag, it cuts into take-home income fast.
5
Overhead, Marketing, And Reserves
Overhead, marketing, and reserves
Fixed overhead is $17,000/month — including $12,000 rent, $1,500 cleaning and maintenance, $800 insurance, and $500 patient portal software. Add 9% of revenue for Year 1 lead acquisition and 3% merchant fees, and cash drag hits 12% before owner pay. If rent stays high before utilization rises, even a busy-looking clinic can run short on cash.
Reserves come before owner distributions. Here’s the quick math: cash left for the owner is about revenue × 88% minus $17,000, before any other payroll, debt, or taxes. That means the clinic can look full and still fail to pay the owner if collections lag or fixed costs are too heavy.
Track cash before pay
Measure monthly revenue, lead acquisition at 9%, merchant fees at 3%, and the cash left after the $17,000 overhead stack. Break out rent, because $12,000 is the biggest fixed line and the fastest way to squeeze owner pay if bookings slow.
- Track cash before owner draws.
- Test rent against utilization.
- Keep reserves ahead of distributions.
If rent rises before utilization does, reserve cash protects the owner’s income. A good month should fund the next slow one, not just pay this month’s bills.
6
Low, base, and high owner income scenarios
Owner income scenarios
Early-year pay is tight because payroll and fixed overhead sit in front of revenue, but income expands fast once utilization, pricing, and therapist count move up.
| Scenario | Low CaseDownside case | Base CaseModeled case | High CaseUpside case |
|---|---|---|---|
| Launch model | Year 1 is a ramp-up case, so owner pay is thin. | Year 3 is the modeled case, with better volume but an incomplete payroll build. | Year 5 is the strongest case, with the widest earnings capacity. |
| Typical setup | Year 1 revenue is $576,420, direct and variable costs run about 21%, fixed overhead is about $204,000, payroll is about $329,500, and EBITDA is about -$78,000. | Year 3 revenue is $2.191 million, direct and variable costs are about 18%, EBITDA is about $1.797 million, and the full Year 3 payroll detail is not provided. | Year 5 revenue is $4.620 million, direct and variable costs are about 16%, fixed overhead is about $204,000, payroll is about $559,000, and EBITDA is about $3.118 million before taxes and reserves. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $0No draw | Mid-six figuresModeled support | High six figuresUpside ceiling |
| Best fit | Founders stress-testing opening-year cash and thin take-home pay. | Teams planning a scaled clinic with incomplete Year 3 staffing detail. | Owners testing the mature clinic case and the upside ceiling. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Posture Correction Services Porter's Five Forces Analysis
- Posture Correction Services BCG Matrix
- Posture Correction Services Business Model Canvas
- What Are The 5 KPI Metrics For Posture Correction Services?
- Posture Correction Services Business Plan Template in Pre-Written Word
- How Increase Profits For Posture Correction Services?
- What Are Posture Correction Services' Operating Costs?
- Posture Correction Services Startup Costs: $730K Funding Plan
- Posture Correction Services Financial Model Template in Excel
- How To Open A Posture Correction Service In 6 To 12 Weeks
- How To Write A Business Plan For Posture Correction Services?
- Posture Correction Services Marketing Mix
- Posture Correction Services Marketing Plan
- Posture Correction Services Business Proposal
- Posture Correction Services PESTEL Analysis
- Posture Correction Pitch Deck Example Editable PPTX
- Posture Correction Services Business SWOT Analysis
- Posture Correction Services Value Proposition Canvas
Frequently Asked Questions
In the researched model, first-year operations support about $66,900 before owner pay and reserves The planned CEO and Clinical Director salary is $145,000, but paying it in full creates about negative $78,100 EBITDA in Year 1 By Year 5, revenue reaches $462M and EBITDA is about $312M before taxes and reserves