 Owner income$0
Owner income$0How Much Psilocybin Therapy Center Owners Make at $816K/Month

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$0  Net margin-1.4%
Net margin-1.4% Revenue for target pay$695k
Revenue for target pay$695k Business difficultyHard
Business difficultyHard


A psilocybin therapy center owner may have little to no first-year distribution in this researched base case Here’s the quick math: $81,600/month in revenue less 20% direct costs leaves $65,280/month of contribution, then $24,900 fixed overhead and $40,833 visible payroll leave about negative $453/month before owner pay, taxes, debt service, and reserves Mature modeled revenue rises to $669,700/month by Year 5, but owner income depends on expanded staffing, compliance load, reserves, and whether the owner also holds a paid clinical or management role
Owner income$0Net margin-1.4%Revenue for target pay$695kBusiness difficultyHardWant to test your owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income depends on revenue, margin, payroll, taxes, debt, and reserves.
Want to check owner income in the Psilocybin-Assisted Therapy Center model?
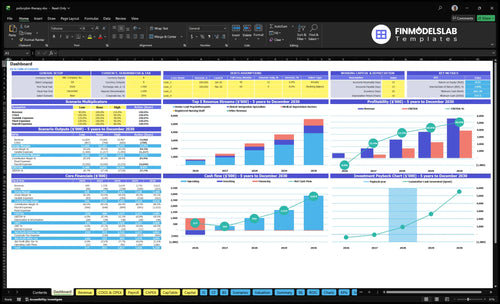
The Psilocybin-Assisted Therapy Center Financial Model Template dashboard shows revenue, gross margin, fixed costs, payroll, operating profit, cash flow, and owner compensation. It also shows Year 1 revenue at $81,600/month, Year 5 at $669,700/month, direct costs falling from 20% to 12%, and fixed overhead at $24,900/month; open the model to review the tabs, charts, and reserve policy.
Owner-income model highlights
- Owner pay source rules
- Revenue and margin trends
- Utilization and reserve policy
Can a psilocybin therapy center be profitable?
Yes, a Psilocybin-Assisted Therapy Center can be profitable, but the base case is basically break-even: $81,600 monthly revenue minus 20% direct costs leaves $65,280 contribution, then $24,900 fixed overhead and $40,833 payroll leave about -$453/month before owner pay and reserves; see What Are Operating Costs For Psilocybin-Assisted Therapy Center? for the operating cost side. The business only clears profit with higher utilization, tighter scheduling, controlled compliance spend, and enough licensed practitioner capacity.
Base Case Math
- $81,600 monthly revenue
- $65,280 contribution after direct costs
- $65,733 overhead plus payroll
- -$453/month before owner pay
Profit Levers
- Raise practitioner utilization
- Tighten session scheduling
- Control compliance cost
- Protect licensed capacity
What revenue is needed to pay a psilocybin therapy center owner?
Psilocybin-Assisted Therapy Center needs about $82,167/month just to hit first-year break-even before owner pay, using $65,733 of fixed overhead and visible payroll at an 80% contribution margin. After that, owner pay is not profit you can spend freely; it still has to cover reserves, taxes, debt service, and reinvestment. Here’s the quick math: at an 80% margin, every $1 of owner pay needs about $1.25 of extra revenue.
Base break-even
- $65,733 fixed overhead and payroll
- 80% contribution margin
- $82,167/month pre-owner-pay break-even
- Revenue is not take-home pay
Owner pay math
- Pay starts above break-even
- Keep reserves after payroll
- Cover taxes and debt service
- Reinvest before raising draws
What costs reduce psilocybin therapy center profit margin most?
If you’re asking what squeezes the Psilocybin-Assisted Therapy Center margin most, it’s clinical staffing, long session blocks, facility cost, liability insurance, compliance, and patient acquisition; see What 5 KPIs Should Psilocybin-Assisted Therapy Center Track? for the metrics that expose the leak fast. Year 1 direct and variable costs already total 20% of revenue, with 5% clinical supply, 3% testing and screening, 8% intake and digital marketing, and 4% compliance/legal oversight. Monthly fixed costs add $24,900 before a single extra session, and staffing cuts cannot replace licensed care standards.
Biggest cost pressure
- Clinical staffing drives quality and labor cost.
- Long sessions reduce daily throughput.
- Patient acquisition takes 8% of revenue.
- Compliance and legal oversight take 4%.
Fixed monthly load
- $12,000 lease each month.
- $6,500 insurance each month.
- $1,800 secure health IT and EHR upkeep.
- $2,200 utilities and security.
Want to see the main income drivers?
1
$81.6K/moProgram Volume
More completed programs lift revenue fastest, and Year 1 already implies about $81.6K a month.
2
$4.5K-$5KProgram Price
Higher program prices raise gross revenue without adding much direct cost, so take-home income climbs fast.
3
40%-90%Utilization
Better use of therapists, doctors, and facilitators spreads payroll across more sessions and protects EBITDA.
4
12%-20%Variable Cost
Each point cut in direct client cost flows straight into contribution margin and cash.
5
$24.9K/moFixed Overhead
Lease, insurance, IT, and admin keep cash pressure high until volume is large enough to cover them.
6
$0Reserve Policy
Keeping early cash in reserve can hold owner distributions near zero until breakeven and payback improve.
Psilocybin-Assisted Therapy Center Core Six Income Drivers
Completed Treatment Volume And Capacity Utilization
Completed Treatment Volume
Volume sets the revenue ceiling. With the Year 1 output assumption, the center delivers 96 senior psychotherapy programs, 30 integration sessions, 6 medical supervision services, 24 nursing services, and 30 group facilitation services a month, or 186 services total. If those slots go unfilled, top-line income drops right away, and owner pay feels it fast.
Capacity rises as utilization improves: senior lead from 60% to 90%, integration from 50% to 85%, and medical supervision from 40% to 80%. The real cap is not demand alone; it is prep time, treatment time, integration time, licensed staffing ratios, and room turns. No completed session, no revenue.
Fill the Schedule, Not Just the Pipeline
Track booked vs. completed sessions, no-shows, room use, and clinician hours by role. If utilization rises without adding fixed payroll, more revenue should drop to profit and owner draw. If it does not, the schedule is leaking somewhere.
- Watch slot fill by service line.
- Track cancellations by step.
- Measure room turns per day.
- Match staffing to licensed ratios.
If prep, treatment, or integration bottlenecks stay fixed, higher demand will not convert into cash. The missed slots show up as lower monthly revenue and weaker distributions.
1
Program Pricing And Revenue Per Client
Pricing Per Client
Pricing moves revenue faster than cost cuts when demand and access hold. Here’s the quick math: if one client uses all five billed services, revenue per client rises from $6,900 in Year 1 to $7,800 in Year 5, a 13% increase. That lifts gross revenue and helps cover fixed overhead, but only if clients still accept the offer at the new price.
This driver includes the price for each service line: $4,500 senior lead psychotherapy, $250 integration, $1,200 medical supervision, $800 nursing, and $150 group facilitation in Year 1, rising to $5,000, $300, $1,400, $900, and $200 in Year 5. Affordability, payer mix, jurisdiction, and clinical protocol cap how far pricing can move owner income.
Measure Realized Price, Not List Price
Track realized revenue per client, not just posted rates. Separate billed revenue from cash collected and owner distributions, because timing, deposits, and reserves change what the owner can actually pay themselves. If price rises but conversion falls, the higher rate may not improve take-home income.
- Track revenue by service line.
- Watch client mix and payer mix.
- Test price against close rate.
- Review collection timing monthly.
A higher realized price helps more when staffing and clinical capacity stay full, because each filled slot carries more revenue before fixed overhead. If access is tight or protocols limit volume, the ceiling is price-sensitive, so the owner should forecast revenue per client separately from salary, profit draw, and retained cash.
2
Clinical Labor Utilization And Staffing Efficiency
Clinical Labor Efficiency
Staffing efficiency sets gross margin here because payroll is large and fixed before volume shows up. Year 1 staffing includes 2 senior lead psychotherapists, 3 clinical integration specialists, 1 medical supervision doctor, 2 registered nursing staff, and 1 group facilitation expert, plus visible fixed payroll of $490,000 a year, or about $40,833 a month.
When clinicians are underbooked, payroll becomes drag and owner take-home shrinks fast. When the schedule is pushed too hard, care standards, compliance, and safety take the hit. Here’s the quick math: every idle paid hour lowers margin, but every extra booked hour has to stay inside licensed ratios and protocol limits.
Track Paid Hours vs. Billable Hours
Measure each role’s billable utilization as booked client-facing time divided by paid time. Track it by role, week, and session type, so you can see whether the mix of therapy, integration, nursing, and supervision is covering the payroll base.
Watch two risks: low utilization creates payroll waste, and overbooking raises compliance and care risk. The owner’s income improves when the team is staffed to actual session demand, not just headcount, and when nonclinical work stays off senior clinicians’ calendars.
- Track booked hours by role
- Separate clinical and admin time
- Cap schedules to care rules
3
Variable Delivery Cost Per Treatment Program
Variable Delivery Cost Per Program
For this center, variable delivery cost is the direct spend tied to each treatment program, not rent or payroll. In Year 1, those costs equal 20% of revenue, so $81,600 revenue leaves $65,280 in contribution margin to help cover fixed overhead, debt, taxes, and owner pay.
Here’s the quick math: 5% clinical supply, 3% laboratory testing and screening, 8% patient intake and digital marketing, and 4% compliance and legal oversight. By Year 5, modeled variable cost drops to 12%, which lifts contribution margin to 88% and gives the owner more cash room before distributions.
Track Cost Per Delivered Program
Measure each cost bucket per delivered program, not just total spend. Track treatment count, revenue per program, supply cost, screening and lab cost, intake and marketing cost, and compliance cost, then compare them to revenue each month. That shows whether margin is widening because volume is up or because costs are actually falling.
Keep fixed items separate: rent, insurance, admin payroll, debt service, and owner pay. If variable cost stays at 20% or less, contribution holds at 80% or better; if it drifts above plan, owner pay gets squeezed fast even when topline revenue looks healthy.
- Track cost per treatment monthly
- Split direct from fixed costs
- Monitor each percentage bucket
- Review margin by program type
4
Fixed Overhead, Licensing, Compliance, And Facility Burden
Monthly Overhead Hurdle
Fixed overhead is the cash burn you pay before owner pay. The model shows $24,900/month in lease, insurance, secure health IT, utilities, accreditation, and admin office costs, plus $40,833/month in visible fixed payroll in Year 1. That is about $65,733/month before variable delivery costs, so the center has to clear a high monthly floor before the owner can take money home.
Here’s the quick math: that works out to about $788,796/year in fixed burden before owner draw, taxes, reserves, or reinvestment. If volume slips or staffing stays underused, profit gets squeezed fast. The hard truth is simple: this overhead is not background noise, it is the benchmark that decides whether the owner gets paid.
Track the burn before you pay yourself
Measure a monthly coverage ratio by dividing revenue by fixed overhead. Track each cost line on its own: lease, insurance, secure health IT, utilities, accreditation, and fixed payroll. If one line rises, you need higher utilization, better pricing, or leaner staffing before you take distributions.
- $24,900 nonpay overhead
- $40,833 fixed payroll
- Watch monthly revenue coverage
- Test staffing before adding space
The clean rule: do not treat regulated overhead as back-office noise. It is core economics, and it sets the monthly floor the center must clear before the owner can pay themselves.
5
Reserves, Reinvestment, And Owner Distribution Policy
Cash Before Owner Draws
Profit is not the same as spendable cash. In Year 1, the model is about negative $453/month before owner pay, taxes, reserves, debt service, or reinvestment, so distributions are not supported in the base case. That means the business needs cash discipline, not owner draws, until operations turn positive.
Pre-tax and post-tax income must stay separate. Owner compensation should be modeled as salary, distributions, and retained cash in different buckets. If those lines get mixed together, it is easy to overstate take-home pay and underfund the clinic’s working capital.
Set the Reserve Policy First
Track a monthly reserve target for payroll cushion, compliance updates, marketing, insurance renewals, facility improvements, and expansion. The first question is simple: after fixed overhead and variable costs, how much cash is left? If the answer is still negative, keep earnings inside the business and do not plan owner distributions.
Use a cash forecast, not just the income statement. Separate owner salary, distributions, and retained cash so you can see what is available after tax and after reinvestment. One clean rule helps: no draw until the reserve balance can cover the next operating shock.
6
Compare low, base, and high owner-income scenarios without implying a forecast
Owner income scenarios
Owner income shifts with utilization, compliance burden, staffing, and treatment volume. Early months can sit near break-even, while mature years can produce strong pre-tax cash flow.
| Scenario | Low CaseUtilization risk | Base CaseCompliance burden | High CaseCapacity limits |
|---|---|---|---|
| Launch model | This is the low-earnings path with early utilization and near break-even owner cash. | This is the modeled middle path with steady utilization and positive owner cash flow. | This is the strong-earnings path with fuller capacity and heavier reinvestment needs. |
| Typical setup | Year 1 sits at $81,600 monthly revenue, 80% contribution margin, $24,900 overhead, and $40,833 visible payroll, so pre-tax owner distribution is about zero. | By Year 3, revenue capacity reaches $313,810 a month with about 84.5% contribution margin before expanded payroll, reserves, taxes, and debt. | By Year 5, revenue capacity reaches $669,700 a month with about 88% contribution margin before expanded staffing and reinvestment. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $0Near break-even | $488k - $1.4MModeled cash flow | $1.4M - $3.9MUpside case |
| Best fit | Use this to test a slow launch, weak demand, or delayed ramp in treatment volume. | Use this as the planning case for a functioning center that keeps growing without assuming perfect occupancy. | Use this to test what happens if demand stays strong and the center keeps adding volume without losing control of costs. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Psilocybin-Assisted Therapy Center Porter's Five Forces Analysis
- Psilocybin-Assisted Therapy Center BCG Matrix
- Psilocybin-Assisted Therapy Center Business Model Canvas
- What 5 KPIs Should Psilocybin-Assisted Therapy Center Track?
- Psilocybin-Assisted Therapy Center Business Plan Template in Pre-Written Word
- How Increase Profits Psilocybin-Assisted Therapy Center?
- What Are Operating Costs For Psilocybin-Assisted Therapy Center?
- Psilocybin Therapy Center Startup Costs: $327K+ Before Opening
- Psilocybin-Assisted Therapy Center Financial Model Template in Excel
- How to Open a Psilocybin-Assisted Therapy Center in 9–18+ Months
- How To Write A Business Plan For Psilocybin-Assisted Therapy Center?
- Psilocybin-Assisted Therapy Center Marketing Mix
- Psilocybin-Assisted Therapy Center Marketing Plan
- Psilocybin-Assisted Therapy Center Business Proposal
- Psilocybin-Assisted Therapy Center PESTEL Analysis
- Psilocybin-Assisted Therapy Center Pitch Deck Example Editable PPTX
- Psilocybin-Assisted Therapy Center Business SWOT Analysis
- Psilocybin-Assisted Therapy Center Value Proposition Canvas
Frequently Asked Questions
In the first-year base model, owner distributions are effectively $0 because $81,600 monthly revenue produces $65,280 contribution after 20% direct costs, then $24,900 fixed overhead and $40,833 visible payroll use the cash Owner salary must be planned separately from distributions, taxes, reserves, and debt service