 Owner income$13.5M
Owner income$13.5MHow Much a Radiation Oncology Center Owner Can Make: $129M Year 1

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$13.5M  Net margin74.5%
Net margin74.5% Revenue for target pay$18.1M
Revenue for target pay$18.1M Business difficultyHard
Business difficultyHard


You’re buying heavy equipment before the referral engine is fully proven, so owner income has to be modeled from center-level cash flow, not assumed like a physician salary Using the provided five-year assumptions, the center generates $181M in first-year revenue and $129M in EBITDA before debt service, reserves, taxes, and reinvestment Scope includes treatment volume, payer collections, staffing, equipment, fixed overhead, and owner take-home limits
Owner income$13.5MNet margin74.5%Revenue for target pay$18.1MBusiness difficultyHardWant to test your own owner income case?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only, not guaranteed salary, tax advice, or owner distribution advice.
Want to see the full Radiation Oncology Center financial model?
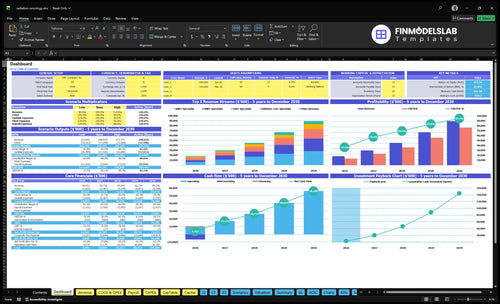
The Radiation Oncology Center Financial Model Template shows dashboard, income outputs, costs, reserves, and owner take-home assumptions; open the model. It also maps monthly revenue, EBITDA margin, payroll growth, fixed overhead, utilization, and distributable cash, using $59k monthly fixed costs, $117M first-year payroll, 600% IMRT utilization, 450% SBRT utilization, and $181M first-year revenue.
Owner-income model highlights
- Owner take-home output
- Revenue and margin charts
- Scenarios and staffing tabs
Is a radiation oncology center profitable?
Yes, a Radiation Oncology Center is profitable in the researched base case: first-year revenue is $181M and EBITDA is $129M before debt service, reserves, taxes, and reinvestment; for startup-cost context, see How Much To Start Radiation Oncology Center Business?. Here’s the quick math: EBITDA margin is about 71.3% ($129M / $181M), while fixed overhead is $708k annually, or about 0.4% of revenue, so utilization carries the model.
Profit Drivers
- Keep treatment volume high
- Protect reimbursement rates
- Maximize machine utilization
- Fill capacity through referrals
Cash Risks
- Control staffing costs
- Reduce claim denials
- Prevent equipment downtime
- Watch payer timing closely
What operating costs affect radiation oncology center profit margin?
If you’re modeling a Radiation Oncology Center, profit margin is mostly a cost-control and utilization problem, not just a revenue problem; the biggest drains are payroll, medical physicist coverage, dosimetry, nursing, supplies, software, billing, referral marketing, equipment service, lease, insurance, utilities, IT, and maintenance. For planning context, see How Do I Write A Business Plan For Radiation Oncology Center? Fixed overhead runs about $59k a month, and variable expenses fall from 180% to 122% of revenue across the model.
Big cost buckets
- Clinical payroll is the biggest cost
- Physicist, dosimetry, and nursing matter
- Supplies and software add steady drag
- Billing, marketing, and service fees stack up
Margin drivers
- Utilization drives margin, not revenue alone
- Fixed overhead stays near $59k monthly
- Variable expense ratio improves from 180% to 122%
- First-year payroll is $117M
How much revenue does a radiation oncology center need?
A Radiation Oncology Center needs about $1.9M in monthly revenue to break even before owner distributions. That comes from roughly $1.565M in monthly payroll and fixed overhead, divided by an 82% contribution margin. If first-year monthly revenue is $15M, the base case clears operating break-even, but owner pay should stay separate from taxable income, debt service, and reserves.
Break-even math
- $1.9M monthly break-even
- $1.565M payroll plus overhead
- 82% contribution margin
- Operating break-even only
Owner pay setup
- Keep salary separate
- Keep taxable income separate
- Keep owner distributions separate
- Fund reserves and debt first
Want the six income drivers that matter most?
1
$18.1MTreatment Volume
More treated cases turn the fixed clinical base into revenue, and Year 1 sales are about $18.1M.
2
$800-$3.7KPayer Mix
Better reimbursement per treatment lifts revenue faster than cost, so mix changes move owner take-home.
3
40%-85%Utilization Rate
Pushing machine use toward the upper end spreads fixed costs over more treatments and lifts margin.
4
$1.17MStaffing Model
Year 1 payroll starts at about $1.17M, so hiring ahead of demand can cut EBITDA and cash.
5
$59K/moFixed Overhead
About $59K a month in lease, service, insurance, utilities, IT, and upkeep sets the breakeven floor.
6
-$942KReserve Policy
Cash bottoms near negative $942K in Month 6, so reserve and debt choices decide how much equity stays intact.
Radiation Oncology Center Core Six Income Drivers
Treatment Volume
Treatment Volume
Treatment volume drives collections first. At the modeled monthly mix per specialist, billable activity is about $2.06M before payer collections: 350 IMRT at $1,200, 180 SBRT at $3,500, 320 IGRT at $1,100, 400 palliative care at $800, and 120 brachytherapy at $2,800.
The owner’s income pool rises only if that volume is profitable and clinically supportable. Weak referrals, scheduling gaps, or capacity limits can leave revenue below plan while payroll and facility costs keep running, so volume has to fill the schedule and clear through collections, not just show up on paper.
Track Fill and Cash
Measure volume by modality, specialist, and payer, then compare billed treatments to collected cash. Here’s the quick math: if the center misses volume in one service line, the lost cash is immediate and the fixed cost base still sits there, so owner pay gets squeezed fast.
Use a simple control set: referral source count, booked-treatment rate, no-show gaps, prior-authorization delays, and days to cash. One clean rule: if the schedule is thin, the margin problem starts before the finance model does.
- Track treatments by modality monthly
- Watch referral conversion by source
- Flag empty slots early
- Compare billed vs collected cash
- Check capacity before adding volume
1
Payer Mix and Reimbursement
Payer Mix and Reimbursement
Payer mix is the share of cases paid by each insurer, and reimbursement is the cash collected after billing. In the first-year model, source prices are $1,200 IMRT, $3,500 SBRT, $1,100 IGRT, $800 palliative care, and $2,800 brachytherapy. Same treatment volume can produce very different owner cash if the mix shifts toward lower-paying care.
Here’s the quick math: cash = billed treatments × price × collect rate. Prior authorization, denials, and slower payer payments can cut or delay cash, so accounting revenue may not match bank cash. What this estimate hides is payer-specific contract rates and denial patterns, which can move take-home pay before staffing and reserve decisions.
Track net collections by modality
Measure each modality separately: case count, allowed amount, denial rate, and days to collect. Compare IMRT, SBRT, IGRT, palliative care, and brachytherapy so you can see which services fund owner pay and which ones only add work. A small change in payer mix can swing monthly cash fast.
- Track denial rate by payer.
- Track days from claim to cash.
- Stress-test SBRT and palliative mix.
Use the slowest payer as the cash forecast, not the best one. If prior auth slips or denials rise, collections lag even when treatments stay full, and that lowers the cash available for owner draws.
2
Machine Utilization
Machine Utilization
Machine utilization is how much billable treatment load a linear accelerator can carry across IMRT, SBRT, IGRT, palliative care, and brachytherapy. In this model, launch utilization is 600% IMRT, 450% SBRT, 600% IGRT, 500% palliative care, and 400% brachytherapy. Mature utilization rises to 850%, 800%, 850%, 800%, and 700%. The owner earns more only when that load turns into collected cash after reimbursement, staffing, and downtime.
What this hides: capacity is fixed until patients, insurance approval, schedules, and clinical staff all line up. A machine sitting idle still carries lease, service, utilities, and maintenance costs, so missed slots hit gross margin fast and shrink profit available for owner pay.
Track Slot Fill, Not Just Installed Capacity
Measure booked hours, completed treatments, downtime, and referral lag by modality. If downtime, maintenance, or no-shows rise, utilization falls even when the machine is available. The goal is more billable treatments per day without adding avoidable overtime or pushing staff past safe staffing levels.
- Track booked vs. open slots daily.
- Separate planned and unplanned downtime.
- Review referral-to-start delays weekly.
- Match staffing to peak treatment blocks.
Run the forecast by modality and reimbursement, not by machine count. That’s how you see whether more utilization turns into distributable cash instead of just more wear, denials, or payroll pressure.
3
Staffing Model
Staffing Model
Radiation oncology staffing is not optional overhead; it is the clinical base that lets treatments happen. The listed first-year roles total $1.17M in annual payroll: $450k medical director, $210k medical physicist, $145k dosimetrist, 2 × $95k oncology nurses, $65k patient navigator, and $110k center administrator.
By year five, payroll rises to $1.875M, or $705k more. That cost only helps owner income if headcount matches utilization, meaning how much of available treatment capacity is actually filled. If staffing grows faster than billable volume, distributable cash drops even when care quality improves.
Match Headcount to Utilization
Track payroll per billable treatment, vacancy days, overtime, and schedule fill rate. Build the model by role, then test whether each added physicist, nurse, dosimetrist, or navigator lifts throughput enough to cover the added fixed cost. More staff helps only when it protects billable slots.
- Link each FTE to treatment volume.
- Watch overtime before hiring.
- Hire to remove bottlenecks only.
- Delay adds if utilization is weak.
4
Equipment and Facility Cost Structure
Equipment and Facility Overhead
Fixed overhead is about $230k per month before debt service: $25k lease, $15k service contracts, $85k liability insurance, $45k utilities and waste, $32k IT and security, and $28k maintenance. That’s a $2.76M annual cash load, so owner income depends on keeping treatment cash flow above this floor.
The key inputs are lease terms, contract scope, insurance limits, utility use, and equipment financing. The first six months also include a Linear Accelerator System capex line, but financing terms must be verified. Debt service and replacement reserves reduce cash available for owner pay, even if reported profit looks healthy.
Control the fixed-cost burn
Track each monthly line item against budget and tie it to treatment volume. A simple test is: if volume drops, does cash still cover $230k/month plus debt and reserves? If not, the owner draw needs to stay capped.
- Review lease escalators and renewals
- Audit service scope and uptime terms
- Separate debt service from operating costs
- Model replacement reserves before distributions
One clean rule: no reserve plan, no reliable owner pay. If financing for the Linear Accelerator System adds heavy debt service, cash gets tighter fast, so the model should show monthly free cash after all fixed facility and equipment costs.
5
Reserve and Debt Policy
Reserve and Debt Policy
Owner pay is not the same as accounting profit here. In a radiation oncology center, cash must first cover debt service, equipment upgrades, compliance, working capital, and reimbursement delays, so distributable cash can be lower than EBITDA. With $129M first-year EBITDA and $758M mature-year EBITDA, the reserve policy is a direct input to what the owner can take home.
Here’s the quick math: every $1 held for reserves or debt is $1 not distributed. That means the model needs a clear cash waterfall, or the owner draw will look too high on paper. What this hides: if claims slow down or equipment needs hit early, cash can get tight even when profit looks strong.
Set the cash reserve rule first
Model the reserve as a fixed policy, not a leftover. Track debt payments, capital reserve, compliance spend, and days sales outstanding (how long cash takes to arrive) before any owner distribution. If reserve funding rises, owner income falls one-for-one unless EBITDA grows faster.
Use a simple control list:
- Set monthly debt service coverage.
- Ring-fence equipment replacement cash.
- Hold working capital for reimbursement delays.
- Document when distributions can resume.
6
Compare ramp, base, and mature owner-income scenarios
Owner income scenarios
Owner income rises as utilization builds, but debt, staffing, and reserves shape how much cash is left to pay the owner.
| Scenario | Low CaseUtilization strain | Base CaseSteadier load | High CaseFull-load upside |
|---|---|---|---|
| Launch model | Year 1 ramp case uses $18.1M revenue and $13.5M EBITDA as the owner-income proxy. | Year 3 model case uses $45.0M revenue and $36.2M EBITDA as the owner-income proxy. | Year 5 mature case uses $89.3M revenue and $76.0M EBITDA as the owner-income proxy. |
| Typical setup | Volume is still ramping, payroll is heavy, and fixed overhead plus reserves reduce cash left for the owner. | Capacity is more stable, staffing is broader, and overhead is spread across more treatments. | The center runs near mature load, with stronger margin absorption but more debt and staffing pressure. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $13.5M EBITDA proxyRamp stress case | $36.2M EBITDA proxyBase case | $76.0M EBITDA proxyMature upside |
| Best fit | Use this to test a slow start or a tighter referral ramp. | Use this as the core operating plan and lender discussion case. | Use this to test what the business can produce if volume and staffing stay on track. |
Planning note: Scenario ranges use researched planning assumptions from the model and are not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Radiation Oncology Center Porter's Five Forces Analysis
- Radiation Oncology Center BCG Matrix
- Radiation Oncology Center Business Model Canvas
- What 5 KPI Metrics Matter For Radiation Oncology Center Business?
- Radiation Oncology Center Business Plan Template in Pre-Written Word
- How Increase Radiation Oncology Center Profits?
- What Are Radiation Oncology Center Operating Costs?
- Radiation Oncology Center Startup Costs: $68M CAPEX Plan
- Radiation Oncology Center Financial Model Template in Excel
- How To Open A Radiation Oncology Center In 12–24 Months
- How Do I Write A Business Plan For Radiation Oncology Center?
- Radiation Oncology Center Marketing Mix
- Radiation Oncology Center Marketing Plan
- Radiation Oncology Center Business Proposal
- Radiation Oncology Center PESTEL Analysis
- Radiation Oncology Center Pitch Deck Example Editable PPTX
- Radiation Oncology Center Business SWOT Analysis
- Radiation Oncology Center Value Proposition Canvas
Frequently Asked Questions
The researched model shows a first-year owner-income pool of about $129M EBITDA before debt service, reserves, taxes, and reinvestment That comes from $181M revenue, 180% variable plus COGS, $117M payroll, and $708k fixed overhead Actual owner take-home can be much lower if the center retains cash or carries equipment debt