 Owner income$250K + dist.
Owner income$250K + dist.How Much Does A Radiologist Practice Owner Make On $467M Revenue?

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$250K + dist.  Net margin~39%
Net margin~39% Revenue for target pay~$638K
Revenue for target pay~$638K Business difficultyHard
Business difficultyHard


Key Takeaways
- Volume drives revenue first, then collections.
- Payer mix changes cash per study.
- Staffing protects turnaround, quality, and margin.
- Fixed costs and reserves shape owner cash.
Owner income$250K + dist.Net margin~39%Revenue for target pay~$638KBusiness difficultyHardWant to test your radiologist owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate only. Actual owner pay depends on collections, case mix, payroll, taxes, debt, reserves, and entity setup. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the Radiologist model?
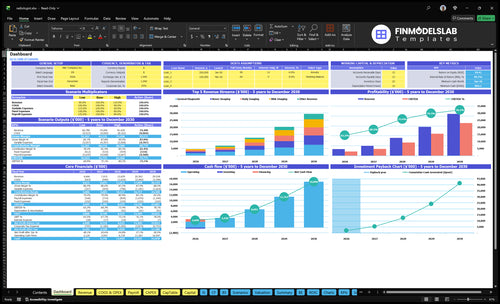
The Radiologist Financial Model Template shows income outputs, modality assumptions, costs, reserves, charts, and tables. Open it.
Owner-income model highlights
- Owner take-home scenarios
- Volume and pricing
- Fixed costs and reserves
How can a radiologist owner increase take-home income?
Radiologist owner take-home income rises fastest when you grow contracted volume, improve modality mix, and push capacity from 60% toward 85%. The modeled path moves monthly revenue from about $3,888K in Year 1 to $246M by Year 5, but only if coverage, payer terms, and capital spend stay tight.
Grow volume
- Win more contracted reads
- Shift to stronger modality mix
- Extend service hours
- Recruit coverage early
Protect take-home
- Push payer rates up
- Hold capital spend to plan
- Watch burnout and turnaround
- Avoid idle equipment
How much revenue does a radiology practice need to pay the owner?
If you want a $250K owner salary, a Radiologist practice needs about $689K in revenue before reserves and debt, using the given 79% payroll contribution. Here’s the quick math: $250K owner pay plus $1.925M visible non-owner payroll and $102K fixed overhead, then divide by 79%. The true floor is higher once equipment, staffing, bad debt, and reinvestment hit.
Owner pay math
- $250K owner salary target
- 79% payroll contribution
- $1.925M visible non-owner payroll
- $102K fixed overhead
What changes the threshold
- Equipment pushes cash needs up
- Staffing raises the real break-even
- Bad debt cuts usable revenue
- Reinvestment lowers owner pay room
What costs reduce radiologist owner income?
Radiologist owner income gets cut by fixed overhead, per-read pay, software, marketing, and outside support costs. For startup spend context, see How Much Does It Cost To Open And Launch Your Radiologist Business?. In the first-year model, the big drains are 12% per-read compensation, 2% specialized software, 5% sales and marketing, and 2% volume-linked professional services, plus $85K monthly fixed overhead and $4,425K visible first-year payroll including the owner salary.
Core income drains
- 12% per-read compensation
- 2% specialized software
- 5% sales and marketing
- 2% volume-dependent professional services
Cash-flow risks
- $85K monthly fixed overhead
- $4,425K visible first-year payroll
- Equipment debt and scanner reserves
- Billing delays and added clinical support
Want the six radiology income drivers?
1
$7.8MStudy Volume
Year 1 volume totals about 3,400 studies a month, so each added read lifts revenue before most costs move.
2
3.3xPayer Mix
The spread from $90 general reads to $300 neuro reads shows why mix changes can swing revenue fast.
3
$90-$330Modality Mix
A heavier share of neuro, body, MSK, and pediatric work lifts average price per study above general diagnostic.
4
$468KStaffing Leverage
Year 1 payroll is about $468K, so labor only pays if each FTE adds enough reads and avoids idle time.
5
$350KTech Burden
About $350K of launch tech and equipment spend plus $102K of fixed overhead can slow cash take-home if ramp is late.
6
$250KOwner Pay
The $250K owner salary and reserve rule decide how much of the $3.0M Year 1 EBITDA becomes take-home.
Radiologist Core Six Income Drivers
Imaging Study Volume And Reading Capacity
Imaging Study Volume and Reading Capacity
Volume is the first revenue lever. The model starts at ~2,580 completed studies per month in year 1 and rises to ~13,177 per month by year 5, with first-year monthly revenue shown at ~$3,888K. One clean rule: more reads only help if turnaround, accuracy, and credentialing stay tight.
What this hides is workload strain. Cash flow and owner pay depend on actual throughput, not booked demand. If studies pile up, overtime, rework, and delayed sign-off can cut margin. The key inputs are completed studies by modality, utilization, read time, error rate, and staffing coverage. Model capacity runs from 60% to 85% by modality over time.
Protect throughput and turnaround
Track completed studies per day, not just referrals. Break volume out by modality and compare it with turnaround time and credentialed coverage. If the team cannot keep standard cases under the 24-hour promise, future volume can stall and owner pay gets squeezed by backlogs and added labor. Volume is only valuable when the pipeline moves.
- Count reads by modality daily.
- Watch turnaround time by case type.
- Track rework and add-on reads.
- Confirm credentialing before adding volume.
- Match staffing to peak workload.
Use a simple check: completed studies × net price per study = monthly revenue, then subtract radiologist workload costs and fixed overhead. Here’s the quick math: 2,580 studies now versus 13,177 later means the business must scale people and process with demand, or margin gets eaten by strain.
1
Payer Mix And Reimbursement
Reimbursement per Study
Payer mix sets the cash you get per read, so the same volume can produce very different income. In year 1, modeled prices are $90 for general diagnostic, $300 for neuro imaging, $220 for body imaging, $220 for musculoskeletal imaging, and $250 for pediatric imaging. By year 5, those rise to $100, $330, $240, $240, and $275.
Commercial, Medicare, Medicaid, self-pay, workers’ comp, and hospital contracts can all change collections, and no rate is guaranteed. That means owner income depends on the weighted average reimbursement per study, not just raw study count. A heavier share of low-paying work cuts cash flow fast, while higher-paying studies lift margin and make it easier to cover payroll, compliance, and owner pay.
Track Realized Cash per Read
Measure collections per study by modality and payer, then compare them to the contracted rate and the actual cash received. Here’s the quick math: collections per read = cash collected ÷ completed studies. If denials, underpayments, or payer shifts push that number down, profit and distributions shrink even when study volume stays flat.
- Track cash by payer and modality
- Watch denial and write-off rates
- Reprice weak contracts at renewal
2
Modality And Service Mix
Modality Mix Drives Revenue per Read
When the mix shifts from general diagnostic at $90 to higher-value work like neuro imaging at $300, revenue per study rises fast. Body and musculoskeletal imaging model at $220, and pediatric imaging enters after year one, so the owner’s income depends on which studies fill the schedule, not just total volume. For example, 100 neuro reads bring $30,000 vs. $9,000 for 100 general reads.
This matters for take-home pay because the revenue lift only sticks if referral demand, credentialed coverage, compliant billing, and equipment use all hold up. If the mix looks rich on paper but the team cannot cover the work or the scanner sits idle, margin drops and cash available for owner pay shrinks.
Track Mix by Modality and Margin
Track studies, price, and gross margin by modality each month. A simple split helps: count general diagnostic, neuro, body, musculoskeletal, and pediatric separately, then compare revenue per read and staffing load. Here’s the quick math: moving 20 studies from general diagnostic to neuro adds $4,200 in gross revenue before labor and overhead.
Manage the mix with referral contracts, credentialing, and coverage rules. If pediatric work starts after year one, make sure billing, staffing, and turnaround can handle it before you promise volume. The real test is whether higher-priced studies improve cash flow after reading cost, not just top-line revenue.
- Track reads by modality weekly.
- Watch payer rules by service line.
- Match coverage to higher-complexity demand.
- Check scanner use before adding work.
3
Staffing Model And Physician Leverage
Physician Leverage
Staffing is the first margin lever here. The model shows $4,425K of first-year visible payroll, including $250K for the CEO/Medical Director, $45K operations, $50K sales and business development, $375K IT support, and $60K billing and credentialing, plus 12% of revenue in per-read pay. If study volume rises faster than that fixed layer, owner profit improves.
Physician leverage means more reads per fixed doctor and admin dollar. The upside is better margin and more cash for owner pay. The risk is simple: if coverage is stretched too far, turnaround slips, quality drops, and referrals can slow. In this model, the limit is not just labor cost; it is keeping speed and accuracy high enough to hold the client base.
Track Reads per Fixed Seat
Measure reads per radiologist FTE, turnaround time, and read-quality issues every week. Use those three numbers to decide when to add staff, because the fixed roles only scale well when the 24-hour turnaround promise still holds. If per-read pay stays at 12% of revenue while fixed payroll is spread over more studies, margin improves and cash available for owner draw rises.
Here’s the practical test: if volume grows but missed coverage, re-reads, or credentialing delays show up, stop adding leverage and add capacity. The goal is not the lowest payroll ratio; it’s the best mix of speed, accuracy, and cash conversion.
- Track studies per radiologist monthly.
- Watch turnaround against the SLA.
- Cap overtime before error rates rise.
- Link bonuses to quality and speed.
- Delay hires until coverage breaks.
4
Equipment, Facility, And Technology Cost Burden
Fixed Facility and Tech Burden
This business can look profitable on paper while cash stays tight. Fixed overhead totals $85K a month, or $1.02M a year, before equipment leases, debt service, or replacement reserves. That stack includes $25K rent, $12K cybersecurity and backup, and $15K malpractice, so owner pay depends on monthly cash coverage, not just reading volume.
Add specialized imaging software at 2% of first-year revenue, and the cash burden rises as collections grow. The inputs that matter are rent, software, cyber, malpractice , legal, accounting, liability, and the lease or debt schedule. If those costs are not covered first, distributions can force the owner to fund operations out of pocket.
Protect Cash Before Owner Pay
Track monthly fixed cash burn against collections, not just booked profit. A clean dashboard should show $85K base overhead, 2% of revenue software spend, and all lease, debt, and reserve payments. If the business misses one of those lines, owner pay should wait.
Set a rule: fund backup systems, compliance, and equipment reserves before any draw. That keeps take-home income tied to real cash, not paper profit. One clean test: if the month cannot cover the full fixed stack, the owner does not get paid.
5
Owner Pay, Reserves, And Distributions
Owner Pay and Cash Draws
Owner income here is a policy choice, not just a profit line. The model pays the CEO / Medical Director $250K from launch through Month 60, but extra distributions only work if cash stays ahead of debt, equipment replacement, working capital, malpractice exposure, and compliance spend.
The first-year EBITDA (earnings before interest, taxes, depreciation, and amortization) is about $314M after modeled costs, but that does not equal cash you can take home. Keep salary, business profit, available cash, reserves, and personal taxes separate so a strong month does not get overdrawn.
Fund reserves before owner draws
Track monthly collections, debt service, reserve targets, and replacement spending before setting distributions. Add a check for malpractice claims and compliance costs, since those can hit cash before profit shows the damage.
- Set a cash reserve floor.
- Separate payroll from draws.
- Forecast taxes on distributions.
- Review liquidity before every payout.
If growth needs more staffing or faster turnaround coverage, hold back owner draws and let cash build first. The clean rule is simple: pay the salary on schedule, then fund reserves, then take distributions only from cash left after obligations.
6
Compare lean, base, and mature radiologist owner-income scenarios
Owner income scenarios
Owner income moves with case mix, utilization, and staffing. Early ramp is salary-led; mature volume can lift distributions, but reserves and equipment spend still take a bite.
| Scenario | Low CaseEarly ramp | Base CaseScaling | High CaseMature |
|---|---|---|---|
| Launch model | This is a salary-led early ramp with limited distribution and tighter cash control. | This is the working-case model with steady volume, broader modality mix, and moderate owner draw. | This is the stronger-earnings path with higher utilization, better mix, and more room for distributions. |
| Typical setup | Year 1 volume, roughly $4.7M revenue, about 21% combined direct and variable costs, and a one-owner medical director role with reserve discipline. | Midpoint volume and capacity assumptions drive a blended neuro, body, MSK, and pediatric mix with lean staffing and controlled overhead. | Year 5 style volume, roughly $29.5M revenue, higher capacity use, and better spread across neuro, body, MSK, and pediatric reads. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $250k - $350kIncome floor | $350k - $700kCore plan | $700k - $1.5MUpside path |
| Best fit | Use this to stress-test a slow ramp and salary-first planning. | Use this as the working plan for a mixed outpatient practice. | Use this to test upside when volume, mix, and efficiency all improve. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Radiologist Porter's Five Forces Analysis
- Radiologist BCG Matrix
- Radiologist Business Model Canvas
- 7 Critical KPIs to Measure Your Radiologist Practice Success
- Radiologist Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Radiologist Practice Profitability
- How Much Does It Cost To Run A Radiologist Practice Monthly?
- Radiologist Startup Costs: $804K Opening Cash And CAPEX Plan
- Radiologist Financial Model Template in Excel
- How To Open A Radiology Practice In 6–18 Months With A Clear Launch Plan
- How to Write a Business Plan for a Radiologist Practice (7 Steps)
- Radiologist Marketing Mix
- Radiologist Marketing Plan
- Radiologist Business Proposal
- Radiologist PESTEL Analysis
- Radiologist Pitch Deck Example Editable PPTX
- Radiologist Business SWOT Analysis
- Radiologist Value Proposition Canvas
Frequently Asked Questions
A radiologist owner can model $250K in salary plus possible distributions In the first year, the assumptions show about $467M in revenue and ~$314M in EBITDA after visible operating costs That profit is not the same as take-home cash because taxes, debt service, equipment reserves, and reinvestment still come first