 Time to Open4-9 monthsSetup window
Time to Open4-9 monthsSetup windowHow to Open a Regenerative Medicine Clinic in 4 to 9 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open4-9 monthsSetup window  Launch Sequence7 stagesCompliance first
Launch Sequence7 stagesCompliance first Key BottleneckProtocol gateApproval path
Key BottleneckProtocol gateApproval path First Revenue StepBooked consultsScreening ready
First Revenue StepBooked consultsScreening ready


You’re opening a regulated medical practice, so the launch plan starts with clinical scope, physician oversight, facility readiness, vendors, staff, and patient intake This guide uses a 4 to 9 month launch window and a Year 1 to Year 5 model period to check timing, staffing, revenue ramp, and runway before the first patient
Time to Open4-9 monthsSetup windowLaunch Sequence7 stagesCompliance firstKey BottleneckProtocol gateApproval pathFirst Revenue StepBooked consultsScreening readyLaunch timeline
Short web summary of the launch plan; the XLSX export carries the full Gantt chart with dates, owners, and dependencies.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7
Legal / compliance
- State filing
- Protocol review
- Malpractice bind
- Consent package
Facility buildout
- Lease signed
- Buildout plan
- Room construction
- Safety inspection
Equipment / suppliers
- Vendor shortlist
- Supplier onboarding
- Order equipment
- Delivery checks
Staffing / training
- Role offers
- Credential checks
- Clinical training
- Mock procedures
Systems / billing
- EMR setup
- Billing setup
- Form testing
- Go-live audit
Marketing / referrals
- Offer messaging
- Referral outreach
- Consult booking
- Opening campaign
Want to test the launch plan before signing commitments?
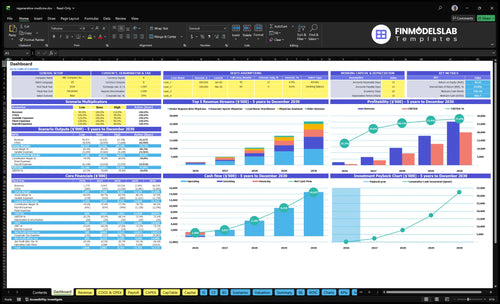
Open the Regenerative Medicine Clinic Financial Model Template for launch dashboard, staffing, revenue ramp, capacity, cash runway, and sensitivities.
Financial model highlights
- 4 roles, no PA
- 45/40/50/35% capacity
- $148,250 monthly revenue
- 12% kits and supplies
- 4% lab processing
- Slower acquisition stress test
- Delayed opening month
Can you open a regenerative medicine clinic?
Yes, you can open a Regenerative Medicine Clinic, but only after legal and clinical authority is clear; start with state medical practice rules, ownership limits, supervision, and treatment scope before signing a lease. Use How Much To Open Regenerative Medicine Clinic? only after the launch blocker is cleared: unclear permission to offer or market the service.
Check Before Launch
- Validate state ownership rules
- Confirm medical director duties
- Review informed consent language
- Audit advertising and outcome claims
Regulatory Red Flags
- Apply FDA biologics rules
- Check 21 CFR Part 1271
- Limit non-physician control
- Get state-specific legal counsel
How do you get patients for a regenerative medicine clinic?
If you're filling a Regenerative Medicine Clinic, start with compliant education and candidacy screening, then push local search pages and referral ties; if you’re mapping the launch, How To Launch Regenerative Medicine Clinic? fits that first step. The first cash comes from booked consultations, screenings, and approved treatment plans, not broad outcome promises. In year 1, role-level capacity only rises from 35% to 50%, so patient acquisition has to fill consult slots gradually.
Get patients
- Use compliant education first
- Screen candidacy before selling
- Build local search pages
- Ask orthopedics for referrals
Track demand
- Track consult volume weekly
- Watch conversion rates closely
- Count no-shows every month
- Review patient reviews often
How long does it take to start a regenerative medicine clinic?
A Regenerative Medicine Clinic usually takes 4 to 9 months to open, and the faster end only happens with existing medical space, ready physicians, limited compliant services, and simple workflows. The timeline slips when lease talks, buildout, state registrations, provider hiring, malpractice coverage, equipment delivery, supplier onboarding, EMR setup, protocol review, and pre-launch marketing stack up. Do not start the first operating month until consent forms, emergency procedures, supplier files, and documentation are tested.
Fast launch path
- 4 months is the fast end
- Use existing medical space
- Start with limited services
- Keep workflows simple
Main delay drivers
- Lease negotiation slows the start
- Buildout and equipment add time
- EMR setup and protocol review
- Test consent and emergency files first
Confirm the clinic is ready before doors open
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Regulatory
- State board rules reviewedCritical
You need this before any patient care starts.
- Corporate practice risk checkedCritical
This protects the clinic structure and physician control.
- HIPAA and OSHA setup readyHigh
Privacy and workplace safety must be in place before launch.
- Malpractice coverage boundCritical
No clinical work should start without active coverage.
Clinical offer
- Service menu approvedCritical
The menu must match scope, training, and risk controls.
- Physician oversight documentedCritical
Clear oversight is needed for safe care and chart review.
- Consent forms testedHigh
Patients need clear consent before any procedure.
Facility
- Procedure rooms readyHigh
Rooms must support safe prep, treatment, and recovery.
- Emergency protocols writtenCritical
Staff need a fast response plan for adverse events.
- Ultrasound and centrifuge testedHigh
If offered, these tools must work before the first case.
Supplies
- Supplier documents storedMedium
This proves sourcing, warranties, and chain of custody.
- Biologic workflow testedHigh
Testing lowers waste and avoids delays in treatment day.
- Refrigeration and storage verifiedHigh
Sensitive materials need stable storage before launch.
Staffing
- Clinical staff scheduledHigh
You need full coverage in the first operating week.
- Role-based training completeCritical
Teams must know intake, prep, and escalation steps.
- Capacity by role confirmedMedium
Year 1 staffing assumes 35% to 50% coverage by role.
Revenue
- Booking an d billing testedCritical
Patients need a clean path from booking to payment.
- Referral plan activeHigh
This supports early patient flow after opening.
- Cash runway model checkedCritical
Your model shows a minimum cash need of $803k.
Which six launch drivers decide opening readiness?
1Compliant Scope
License gateLegal review of services, claims, consent, and sourcing is the gate that determines opening on time.
2Clinical Team
4 rolesYear 1 staffing of four clinical roles supports steadier consult flow and cleaner handoffs.
3Facility Workflow
WorkflowRoom layout, storage, and patient flow cut delays in consults, procedures, recovery, and notes.
4Supplier Readiness
16% varValidated suppliers, cold storage, and backups reduce canceled procedures and last-minute reschedules.
5Patient Pipeline
First consultsLocal SEO, referrals, and education drive first consults faster than waiting until opening month.
6Operating Ramp
$148K/moAt 35% to 50% Year 1 capacity, modeled revenue tests whether demand covers staffing and burn.
Compliant Clinical Scope
Clinical Scope Compliance
Clinical scope compliance is the first launch gate because a regenerative medicine clinic has to align treatment offerings, biologic sourcing, clinical claims, consent forms, and physician oversight with federal and state rules. If you book patients before legal and clinical review, you can end up reworking the menu, ads, and intake docs after first consults, which slows opening and makes day-one care messy.
This is not just a legal issue; it hits operations. The clinic should not open until the service menu, supplier files, consent language, advertising, and medical director sign-off are complete. Late changes can ripple into staffing, supply orders, and cash needs, and they can also undermine the Year 1 plan of about $148,250 monthly revenue at stated capacity.
Pre-Launch Review Checklist
Start by freezing every treatment, biologic, and claim in one review pack. Here’s the quick math: the model assumes 16% total variable clinical cost, with 12% for biologic kits and supplies and 4% for lab processing and consumables, so an unapproved service line can change both margin and compliance at once.
- Lock the menu before ads run.
- Check supplier files for each biologic.
- Approve consent forms and scripts.
- Get medical director sign-off first.
If the scope is clean before launch, the clinic can open with safer patient flow, cleaner marketing, and fewer forced changes after first consults. That keeps the schedule stable and avoids cancelling visits when a treatment or claim gets pulled late.
1
Physician And Clinical Team Readiness
Clinical Team Readiness
A regenerative medicine clinic can’t open cleanly if the right clinicians are hired before supervision, procedure training, and role splits are set. The Year 1 team is 1 senior regenerative physician, 1 associate sports physician, 1 lead nurse practitioner, 1 rehabilitation specialist, and 0 physician assistants, so the launch depends on clear coverage for consults, procedures, and follow-ups from day one.
The bottleneck is not headcount alone; it’s whether the team can safely handle intake, EMR documentation, and emergency drills without confusion. If those rules are late, first visits slow down, handoffs get messy, and patient safety takes a hit. Clean staffing here means steadier consult flow and fewer launch-day surprises.
Set roles before you set schedules
Lock the supervision structure first, then assign who handles intake, procedure prep, follow-up calls, and charting in the EMR (electronic medical record). The senior physician should own oversight, while the nurse practitioner and rehabilitation specialist should have written duties for pre-visit screening and post-procedure care.
Before opening, test the team with at least one mock day: one consult, one procedure flow, one documentation pass, and one emergency drill. If the team cannot move through those steps without questions, the clinic is not ready to take booked patients.
- Write supervision rules before hiring starts.
- Assign intake, follow-up, and charting.
- Run emergency drills with the full team.
- Verify no physician assistant tasks are assumed.
- Test handoffs before first consults.
2
Facility And Procedure Workflow
Clinic Flow Setup
Facility and procedure workflow is the day-one gate that decides whether you can actually treat patients on schedule. The space has to fit consults, procedure-room movement, privacy, recovery flow, supplies storage, documentation, and emergency protocols. If the room map does not match the services you chose, you get delays, awkward handoffs, and early capacity loss on the first day.
Do not overbuild or underbuild the layout, because needs vary by treatment type. The key test is simple: the chosen service menu must work inside the actual rooms, not just on paper. Room mapping, clean workflow design, patient intake routing, and procedure documentation testing should happen before opening, so staff can move patients, supplies, and records without blocking care.
Preopen Flow Test
Before launch, walk one patient through the full path: check-in, consult, procedure, recovery, discharge, and documentation. Then verify where supplies sit, where any specimen handling happens, and how staff respond if a patient needs escalation. That is the fastest way to catch a bottleneck before it hits first revenue.
- Map every room to one clear use.
- Test intake-to-recovery in real time.
- Confirm storage stays out of workflow.
- Check emergency steps with the team.
- Validate charting before opening day.
The main risk is opening in a space that cannot support the chosen services. When that happens, consults run late, recovery gets crowded, and staff spend day one fixing layout problems instead of serving patients.
3
Equipment And Supplier Readiness
Equipment and Supplier Readiness
This gate decides whether the clinic can open on time and run from day one. Biologics suppliers must be validated before bookings start, and that means supplier documents, chain of custody where relevant, storage rules, maintenance plans, and backup supply options are already in place. The Year 1 variable assumptions are 12% for biologic treatment kits and supplies and 4% for lab processing and consumables.
If documentation is missing or supply is unreliable, procedures get canceled or pushed, and first-week revenue suffers. If the clinic offers centrifuges or other processing tools, those units also need setup, testing, and maintenance checks before the first patient. One missed shipment can stall the whole day.
Validate the supply chain before scheduling
Lock in the full intake path before opening: approve suppliers, test ordering, confirm receiving steps, and verify storage and handling procedures. Keep a backup source for biologics and consumables so one delay does not stop treatment flow.
- Review supplier files and certifications
- Test chain of custody records
- Check storage and maintenance steps
- Confirm backup stock and reorder timing
For any processing equipment, run a live test with staff before bookings begin. That catches gaps in setup, calibration, and handoffs early, when fixes are still cheap and patient schedules are not on the line.
4
Patient Acquisition And Referral Pipeline
Patient Acquisition Pipeline
If you wait until opening month to build demand, the clinic can be open on paper and still sit empty. This driver covers local SEO, referral relationships, consult offers, review systems, and follow-up workflows that turn education into booked evaluations from day one.
The big risk is weak or noncompliant messaging. Keep the pitch on fit-for-care screening, not cure claims or aggressive promises, and give orthopedic, sports medicine, pain management, chiropractic, and wellness partners time to learn the service before launch.
Build Demand Before Open
Lock the funnel before the doors open: publish the local search page, set the consult offer, load the review request process, and assign who follows up on every lead. If the first outreach is already live, bookings can start faster and the first revenue is less likely to lag behind staffing and rent.
Test the full path end to end: inquiry, callback, screening, consult booking, and post-visit follow-up. That keeps candidacy evaluation and trust-building moving in sequence, so the opening does not depend on hope or walk-ins.
- Start referral outreach before opening.
- Use compliant, education-first language.
- Track every lead source.
- Ask for reviews after service.
- Follow up until consults are booked.
5
Operating Model And Revenue Ramp
Revenue Ramp Readiness
Open-on-time risk here is simple: if consult volume, conversion, and provider capacity do not match, the clinic can open with weak cash flow even if the space is ready. The model says monthly revenue at stated capacity is about $148,250 before variable clinical costs, and the quick math for 1 senior physician at 60 treatments per month, $2,500 per treatment, and 45% capacity is about $67,500.
This driver covers consultation volume, treatment conversion, provider capacity, staffing, follow-up cadence, cash-pay collection, and runway. The variable clinical cost assumption is 16%, so weak early demand or slow collections can tighten cash fast. The main bottleneck is hiring ahead of demand without enough runway to carry the ramp.
Cash Ramp Checks
Before opening, tie the first 90 days to a plain weekly model: consults booked, consult-to-treatment conversion, treatments per provider, cash collected, and variable cost dollars. If any one of those is off, opening on paper can turn into a cash squeeze in real life.
Set the follow-up path and payment flow before day one. Verify who books returns, who collects at checkout, and how many treatments each clinician can safely handle under the supervision plan. Keep staffing and hiring aligned to actual volume, not the best-case revenue chart.
- Test consult-to-treatment conversion.
- Match bookings to provider capacity.
- Track cash-pay collection daily.
- Hold runway for 16% variable costs.
- Delay hiring until demand proves out.
6
Related Products
- Regenerative Medicine Clinic Porter's Five Forces Analysis
- Regenerative Medicine Clinic BCG Matrix
- Regenerative Medicine Clinic Business Model Canvas
- What 5 KPIs Should Regenerative Medicine Clinic Monitor?
- Regenerative Medicine Clinic Business Plan Template in Pre-Written Word
- How Increase Regenerative Medicine Clinic Profitability?
- What Are Regenerative Medicine Clinic Operating Costs?
- Regenerative Medicine Clinic Startup Costs: $240K+ CAPEX Plan
- Regenerative Medicine Clinic Financial Model Template in Excel
- How Much Does a Regenerative Medicine Clinic Owner Make? $480k+
- How To Write A Business Plan For Regenerative Medicine Clinic?
- Regenerative Medicine Clinic Marketing Mix
- Regenerative Medicine Clinic Marketing Plan
- Regenerative Medicine Clinic Business Proposal
- Regenerative Medicine Clinic PESTEL Analysis
- Regenerative Medicine Clinic Pitch Deck Example Editable PPTX
- Regenerative Medicine Clinic Business SWOT Analysis
- Regenerative Medicine Clinic Value Proposition Canvas
Frequently Asked Questions
Start with compliant clinical scope and physician oversight Then secure the site, procedure workflow, suppliers, staff training, EMR, consent forms, and referral plan A practical launch often takes 4 to 9 months In the researched case, Year 1 starts with 4 clinical roles and capacity assumptions from 35% to 50%