 Time to Open3-6 monthsSetup window
Time to Open3-6 monthsSetup windowHow to Open a Skin Cancer Screening Clinic in 3 to 6 Months

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open3-6 monthsSetup window  Launch Sequence6 stagesCompliance first
Launch Sequence6 stagesCompliance first Key BottleneckCredentialingProvider readiness
Key BottleneckCredentialingProvider readiness First Revenue StepBooked examsBooking live
First Revenue StepBooked examsBooking live


To open a skin cancer screening clinic, you need licensed provider coverage, state-compliant ownership, malpractice coverage, private exam rooms, dermoscopy tools, an EHR, billing setup, pathology or referral workflows, and a launch plan for booked skin exams A typical launch takes 3 to 6 months, but payer credentialing, provider readiness, and leasehold work can stretch the timeline The researched Year 1 staffing plan starts with 1 dermatologist, 1 physician assistant, 2 medical assistants, 1 photography technician, and 1 clinic manager First revenue comes from booked self-pay visits, insured exams once billing is live, and employer or community screening events
Time to Open3-6 monthsSetup windowLaunch Sequence6 stagesCompliance firstKey BottleneckCredentialingProvider readinessFirst Revenue StepBooked examsBooking liveLaunch timeline
This short web summary shows the launch path, and the XLSX export holds the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6
Licensing and compliance
- Board filing
- Malpractice policy
- HIPAA setup
- OSHA review
Site and equipment
- Lease signed
- Fit-out plan
- Buy dermoscopy
- EHR install
Staffing and training
- Role plan
- Recruit clinicians
- Credential hires
- Train workflows
Payer and billing
- Payer list
- Submit enrollments
- Build charge flow
- Claim test
Marketing and opening
- Launch message
- Physician outreach
- Screening campaigns
- Open house
Finance and operations
- Cash forecast
- Hire manager
- Inventory order
- Go-live checklist
Why pressure-test the Skin Cancer Screening Clinic before opening?
See revenue, costs, cash needs, assumptions, payer mix, and break-even logic in the Skin Cancer Screening Clinic Financial Model Template; open it now.
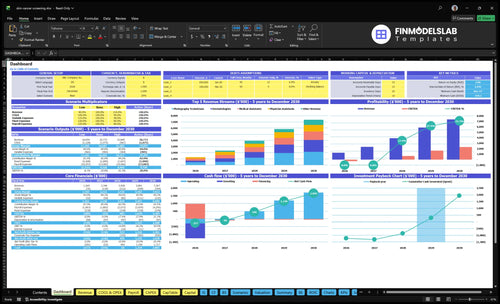
Financial model highlights
- 1 dermatologist, 1 PA
- 2 MAs, 1 tech
- 1 clinic manager
- $1,057k gross revenue
- 85% variable/direct load
- $315k overhead
- $638k visible payroll
- Opening-month cash strain
- Ramp and breakeven path
What do you need to open a skin cancer screening clinic?
A Skin Cancer Screening Clinic needs compliant medical ownership, live licensed provider coverage, written protocols, and payer-ready operations before seeing patients; use How To Write A Business Plan For Skin Cancer Screening Clinic? to map those launch gates. The need is real: the American Academy of Dermatology Association reports 1 in 5 Americans will develop skin cancer in their lifetime, so delays in supervision, pathology, or referrals create clinical and legal risk.
Clinical Requirements
- State-compliant medical ownership structure
- Licensed dermatologist or qualified provider coverage
- Medical director oversight when required
- PA and NP scope-of-practice compliance
Operating Setup
- Malpractice insurance active before care
- HIPAA, OSHA, EHR, billing setup
- Consent forms and clinical protocols
- Pathology, referral, and escalation workflow
How do you get patients for a skin cancer screening clinic?
For a Skin Cancer Screening Clinic, start with local SEO pages, online booking, primary care referrals, employer screenings, community education, insurance directory listings, and reminders; the first revenue usually comes from self-pay skin exams, then insured visits once payer setup is active, as outlined in What Does It Cost To Run A Skin Cancer Screening Clinic?
Match marketing to capacity: the Year 1 model assumes 65% dermatologist utilization and 60% physician assistant utilization, so don’t overspend if scheduling, callbacks, and follow-up aren’t staffed. One clean rule: fill the calendar before you scale spend.
First patient channels
- Local SEO for skin exams
- Online booking on every page
- Primary care referrals
- Insurance directory visibility
Revenue and capacity
- Self-pay skin exams first
- Insured visits after payer setup
- Employer wellness screenings
- Reminder campaigns keep fills up
How long does it take to open a skin cancer screening clinic?
A Skin Cancer Screening Clinic usually takes 3 to 6 months to open, and the main delay is dermatology provider credentialing. Here’s the quick math: while that runs, you can push lease talks, room setup, dermoscopy sourcing, EHR setup, hiring, local SEO, referral outreach, and staff training. Self-pay screening events can start sooner, but only if licensing, documentation, privacy, and follow-up workflows are already in place.
What can move in parallel
- Negotiate the lease early
- Set up exam rooms fast
- Source dermoscopy equipment
- Build the EHR workflow
What can block launch
- Complete payer enrollment
- Finish provider credentialing
- Secure malpractice coverage
- Pass inspection and supervision checks
Confirm the clinic is safe, compliant, and ready before opening day
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Licensing
- Entity and licenses confirmedCritical
The clinic needs a legal base and active licenses before any patient visit.
- Medical director model approvedCritical
A clear oversight model avoids scope and supervision gaps at launch.
- Malpractice policy boundCritical
Coverage must be active before staff start screening patients.
Clinic setup
- Exam rooms inspection readyCritical
Rooms need power, privacy, and workflow space before first use.
- HIPAA privacy controls liveCritical
Patient data must be protected before photos and charts are created.
- OSHA safety plan postedHigh
Staff need clear safety steps for sharps, cleaning, and exposures.
Tools
- Dermoscopy tools installedCritical
Screening needs working dermatoscopes and image capture from day one.
- EHR templates and access liveCritical
Charts, photos, and notes must flow into the record without delay.
- Pathology follow-up workflow setCritical
Biopsy results need a tracked handoff so abnormal findings are not missed.
Staff
- Provider coverage matches scheduleCritical
Booked visits must have licensed coverage in the opening month.
- Team trained on screening flowCritical
Staff need one shared process for intake, exam, photos, and escalation.
- Scheduling and intake scripts readyHigh
Clear scripts cut check-in delays and reduce missed screening details.
Access
- Eligibility and consent forms approvedCritical
Consent and coverage checks must happen before the first exam starts.
- Patient reminders testedHigh
Reminders help keep first visits and follow-ups from slipping.
- Local referral list loadedHigh
Complex cases need a ready handoff path before launch traffic begins.
Billing
- Billing workflow testedCritical
Visits must be documented and billed cleanly to support cash flow.
- Cash runway covers openingCritical
Year 1 EBITDA is negative, so cash needs to cover the launch gap.
- Go-live model signed offCritical
Launch is ready only when patients can be seen, documented, billed, and followed up.
Which launch drivers decide opening readiness?
1Licensing
3-6 moLicensing and dermatologist credentialing are the first gate; without them, opening slips past the target window.
2Facility
Mock visitExam rooms, lighting, EHR access, and utilities must work on site before the first patient walks in.
3Compliance
Tested flowConsent, photos, pathology, and follow-up need one clean handoff, or suspicious lesions get lost.
4Billing
Test claimPayer enrollment and claim testing must work early, or booked visits won't turn into cash.
5Staffing
Day-one teamDay-one staffing needs 1 dermatologist, 1 PA, 2 MAs, 1 photo tech, and 1 manager to keep intake moving.
6Patient Flow
$4K/moThe first 30 to 90 days need booked visits, local search, referrals, and tight callback discipline.
Medical Licensing And Provider Coverage
Medical licensing gate
A skin cancer screening clinic cannot open like a normal office. It has to clear state medical board rules, ownership limits, and any corporate practice of medicine rules before the first patient is booked. If the state requires a medical director, provider licenses, or specific supervision for physician assistants and nurse practitioners, those items have to be in place first.
The biggest launch risk is the dermatologist hire and credentialing path. The readiness signal is a fully covered schedule with compliant sign-off before day one. Year 1 assumes 1 dermatologist and 1 physician assistant, so one missing credential can force delays, cancel visits, and leave the clinic unable to operate as planned.
Lock provider coverage early
Build the license file before you market or schedule. Verify each clinician’s license status, scope, supervision rules, malpractice insurance, and written exam protocols, then document who can sign off on which exam steps. If the clinic needs a medical director, get that agreement done early so the org chart matches the law.
- Confirm state rules first
- Map PA and NP scope
- Set supervision in writing
- Finish credentialing before ads
- Test exam sign-off workflows
What this setup hides is timing. Credentialing, payer enrollment, and license review can all move at different speeds, so a booked calendar is not the same as launch-ready coverage. By Year 5, the model grows to 5 dermatologists, which makes early documentation even more important because each new hire has to fit the same compliant process.
1
Facility And Equipment Readiness
Exam Rooms and Equipment Ready
This launch driver decides whether the clinic can open on time and safely see patients on day one. You need private exam rooms, good lighting, dermatoscopes, imaging or documentation tools, EHR access, infection control supplies, storage, cleaning, and a clear intake flow. If any of the core pieces are missing, staff start working around gaps, and that slows visits, hurts patient confidence, and can delay opening.
Here’s the quick math: fixed non-payroll costs already visible are $20k for the lease, $25k for utilities, $18k for EHR licensing, and $2k per month for maintenance and cleaning. That’s $65k per month before payroll or supplies. A delayed equipment delivery or EHR setup pushes cash out while revenue is still at zero.
Run a Mock Visit First
Don’t treat setup as done until a mock visit works with no workarounds. Verify the lease is signed, utilities are live, cleaning is scheduled, the EHR is licensed and logins work, and all equipment has been delivered and tested. If patients can’t move from intake to exam room to documentation without staff improvising, the clinic is not ready.
- Test room flow end to end.
- Confirm lighting in every exam room.
- Check storage, cleaning, and supply restock.
- Validate EHR access before first patient.
2
Compliance And Clinical Workflows
Clinical Workflow and Compliance
For a skin cancer screening clinic, compliance is not paperwork on the side; it is part of safe care on day one. You need HIPAA privacy safeguards, OSHA safety steps, consent forms, documentation standards, lesion photo rules, and a clear biopsy referral path before the first patient walks in.
The main launch risk is a lost handoff after a suspicious finding. If intake, photos, referral, pathology lab coordination, abnormal lesion follow-up, and escalation rules are not tested end to end, the clinic can open with visits booked but no safe way to close the loop. Year 1 direct cost assumptions also matter: pathology lab fees at 40% of revenue and medical consumables at 20% of revenue leave only 40% before fixed overhead.
Test the Follow-Up Chain Before Opening
Build the workflow in order: consent, exam note, lesion photo, biopsy decision, lab send-out, result tracking, patient callback, and escalation. The readiness signal is a tested workflow from intake through follow-up, with no skipped steps and no manual scramble after a suspicious lesion is found.
- Verify HIPAA and photo storage rules.
- Train staff on OSHA safety steps.
- Map every biopsy handoff.
- Assign abnormal-result follow-up owner.
- Test pathology turnaround and callbacks.
What this hides is timing risk. If pathology or follow-up slips, the clinic can still see patients, but it cannot safely operate from day one at full confidence. That can slow opening, strain staff, and create cash pressure if visits generate costs before the result-tracking process works.
3
Billing, Payer, And Revenue Cycle Readiness
Payer Path Ready
A skin cancer screening clinic can open with booked visits, but it cannot turn those visits into cash on time if payer enrollment and provider credentialing are still pending. The first revenue gate is simple: get the billing path live before the first patient, or insured visits can sit unpaid while the clinic still owes rent, staff, and vendor bills.
This setup includes coding workflows, eligibility checks, claim submission, denial management, and patient statements. The Year 1 prices are $650 for dermatologist visits, $500 for physician assistant visits, $300 for medical assistant services, and $1,000 for photography technician services, so even small billing delays can slow cash right when day-one operating costs start.
Test the Cash Path First
Before launch, run a test claim and a self-pay collection workflow. That means confirming the payer list, provider IDs, coding rules, card capture, and patient statement steps actually work in the clinic’s billing system, not just on paper. If the clinic can’t submit a clean claim or collect a card at checkout, opening date is too early.
- Verify payer enrollment status.
- Confirm each provider is credentialed.
- Test eligibility before booking.
- Set self-pay prices in advance.
- Train staff on card collection.
- Send one sample patient statement.
- Track denial fixes before opening.
4
Staffing And Scheduling Capacity
Day-One Staff Coverage
A screening clinic opens on time only if the schedule can run without heroics. Here, the startup team is 1 dermatologist, 1 physician assistant, 2 medical assistants, 1 photography technician, and 1 clinic manager, with Year 1 utilization of 65%, 60%, 70%, and 62%. That means the real launch risk is not just headcount, but whether each role has enough slack for intake, imaging, prior authorizations, reminders, and follow-up ownership.
One missing shift can stop the clinic flow. If the dermatologist or photo support is overbooked, patients wait, exam rooms back up, and suspicious findings may not get the right handoff. The readiness signal is a day-one schedule staff can actually work, with coverage for front desk intake, medical assistant rooming, photo support, and manager oversight already mapped.
Work The Schedule Before Opening
Build the schedule backwards from patient flow, not from titles. Verify who covers intake, room turnover, photo capture, prior authorization support when needed, reminder calls, no-show follow-up, and abnormal-result ownership. Test the full day in advance so every slot has a name on it, every handoff is clear, and the clinic can still run if one person is out.
- Assign one owner per handoff.
- Block time for photos and calls.
- Set no-show rules before launch.
- Confirm manager coverage every day.
- Test the schedule with real appointment slots.
At 70% medical assistant utilization and 62% photography-tech utilization, there is not much room for chaos. If onboarding slips, or if reminders and follow-up are not owned, first-week capacity drops fast and the clinic looks busier than it can safely serve.
5
Patient Acquisition And Referral Pipeline
Patient Acquisition And Referral Pipeline
Patient flow has to fill the first 30 to 90 days, not just build awareness. For a skin cancer screening clinic, that means local search, online booking, primary care referrals, employer wellness outreach, community education, insurance directory listings, and review capture all need to work before opening. The model assumes $4k per month in digital marketing, so launch pacing matters from day one.
The readiness signal is simple: booked appointments matched to provider capacity. First revenue should come from self-pay exams, then insured visits after payer readiness, plus employer or community screening events. If callbacks are slow or scheduling is loose, demand can pile up without turning into visits, which hurts cash, patient trust, and day-one utilization.
Build The First Booking Path
Before opening, verify that every lead source has one owner, one callback rule, and one booking path. The clinic should test how a new patient moves from search or referral to confirmed visit, then to reminder, intake, and follow-up. Local search, online booking, and referral routing must all point to the same schedule.
- Confirm callback time standards.
- Match slots to provider capacity.
- Load insurer directory profiles.
- Track employer event dates.
- Capture reviews after visits.
What this setup hides is simple: demand only helps if the clinic can answer fast, schedule cleanly, and keep no-shows low. If a strong lead source lands before staffing and calendar rules are ready, the clinic can open with interest but no usable revenue.
6
Related Products
- Skin Cancer Screening Clinic Porter's Five Forces Analysis
- Skin Cancer Screening Clinic BCG Matrix
- Skin Cancer Screening Clinic Business Model Canvas
- What 5 KPIs Matter For Skin Cancer Screening Clinic Business?
- Skin Cancer Screening Clinic Business Plan Template in Pre-Written Word
- How Increase Skin Cancer Screening Clinic Profits?
- What Does It Cost To Run A Skin Cancer Screening Clinic?
- Skin Cancer Screening Clinic Startup Costs: $970K CAPEX Plan
- Skin Cancer Screening Clinic Financial Model Template in Excel
- How Much Skin Cancer Screening Clinic Owners Make: $265K-$334M
- How To Write A Business Plan For Skin Cancer Screening Clinic?
- Skin Cancer Screening Clinic Marketing Mix
- Skin Cancer Screening Clinic Marketing Plan
- Skin Cancer Screening Clinic Business Proposal
- Skin Cancer Screening Clinic PESTEL Analysis
- Skin Cancer Screening Clinic Pitch Deck Example Editable PPTX
- Skin Cancer Screening Clinic Business SWOT Analysis
- Skin Cancer Screening Clinic Value Proposition Canvas
Frequently Asked Questions
Start with provider coverage, state medical rules, malpractice insurance, and a compliant care model Then set up exam rooms, dermoscopy tools, EHR, billing, pathology referrals, scheduling, and patient intake The researched Year 1 plan uses 1 dermatologist, 1 physician assistant, 2 medical assistants, 1 photography technician, and 1 clinic manager