How Much Does It Cost To Open A Surgical Center? $335M CAPEX Plan

A researched planning estimate for this surgical center shows $3345 million in startup CAPEX before working capital, debt service, or owner distributions The largest line is facility build-out at $15 million, followed by operating room equipment at $800,000, anesthesia machines at $300,000, and sterilization equipment at $250,000 Total funding need can exceed CAPEX because the center also carries $53,800 in fixed monthly overhead and about $620,000 in Year 1 salaried administrative and support payroll Treat these as researched planning assumptions, not vendor quotes or guaranteed costs
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
This estimates capitalized startup assets only for a surgical center.
CAPEX only This calculator covers capitalized startup assets only. It excludes inventory, payroll runway, deposits, debt service, working capital, licensing fees, recurring software, insurance, financing costs, and operating expenses.
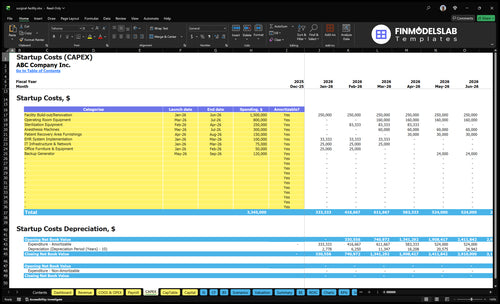
What should you review in this screenshot?
Open the Surgical Center Financial Model Template CAPEX tab: $3.345M startup costs, Month 1–9 timing, depreciation, amortization; review assumptions.
Screenshot highlights
- Payer ramp-up and working capital
- Procedure volume assumptions
- $4,500 Year 1 price
- 500%-550% role capacity
- $538k fixed overhead
- 165% variable cost load
How much money do you need to open a surgical center?
YOU NEED ABOUT $33M–$45M IN RESEARCHED CAPEX TO OPEN A SURGICAL CENTER, BUT TOTAL FUNDING MUST ALSO COVER PRE-OPENING EXPENSES, WORKING CAPITAL, CASH RESERVES, AND CONTINGENCY; CHECK What Is The Current Growth Trend Of Your Surgical Center? BEFORE YOU LOCK THE RAMP.
CAPEX DRAW
- START WITH $33M–$45M RESEARCHED CAPEX
- PLAN DRAWS FROM MONTH 1 TO MONTH 9
- DO NOT TREAT THIS AS EQUIPMENT COST ONLY
- ADD CONTINGENCY ABOVE CONSTRUCTION BUDGET
CASH PRESSURE
- FIXED OVERHEAD RUNS $538K PER MONTH
- YEAR 1 SALARIED PAYROLL IS $620K
- VARIABLE LOAD REACHES 165% OF REVENUE
- PAYER ENROLLMENT, CREDENTIALING, AND INSPECTIONS CAN DELAY CASH
What hidden costs do founders miss when starting a surgical center?
The biggest misses in a Surgical Center budget are the costs outside the CAPEX calculator: credentialing delays, payer enrollment, staff training, accreditation prep, policy manuals, malpractice coverage, recruiting, inventory, emergency drugs, and cash reserves. If you want the owner-income angle, see How Much Does The Owner Of Surgical Center Make? but the real risk is working capital: fixed overhead is $538k per month before payroll, and Year 1 payroll base is $620k plus clinical ramp staffing. Line items like $10k monthly medical malpractice insurance, $25k regulatory compliance fees, $3k EHR subscription, $5k equipment maintenance contracts, and $35k sterilization services can derail cash fast.
Hidden start-up costs
- Credentialing delays slow first revenue
- Payer enrollment can take weeks
- Staff training adds launch cost
- Accreditation prep needs cash upfront
Cash flow items to model
- $10k monthly malpractice insurance
- $25k regulatory compliance fees
- $35k sterilization services
- $620k Year 1 payroll base
How do you fund a surgical center startup?
For a Surgical Center, fund the startup with a tight uses-and-sources plan: $3345M CAPEX, pre-opening expenses, working capital, reserves, and contingency. Put owner equity and physician-investor capital in first, then layer in equipment financing, tenant improvement allowances, bank debt, and a working capital line. Size debt to the Month 1 to Month 9 CAPEX draw, the break-even volume, and the reimbursement ramp, using Year 1 staffing of 2 surgeons, 1 anesthesiologist, 4 OR nurses, 3 surgical techs, and 3 recovery nurses plus a $4,500 average procedure price.
Uses
- $3345M CAPEX for buildout
- Pre-opening expenses before launch
- Working capital for early months
- Reserve and contingency funding
Sources
- Owner equity as core capital
- Physician-investor capital for alignment
- Equipment financing for major gear
- Bank debt plus working capital line
Calculate Fuding Needs
Startup cost summary
This table summarizes surgical center startup CAPEX and opening cash needs across facility, equipment, systems, and launch working capital.
| Cost Category | Base Estimate | Main Cost Driver | CAPEX Calculator |
|---|---|---|---|
| Facility Build-out/Renovation | $1,500,000 | Construction scope, MEP work, and finish quality | Yes |
| Operating Room Equipment | $800,000 | Procedure room count and equipment spec | Yes |
| Sterilization Equipment | $250,000 | Sterile processing capacity and equipment mix | Yes |
| Anesthesia Machines | $300,000 | Machine count, monitoring, and vendor pricing | Yes |
| Patient Recovery Area Furnishings | $150,000 | Recovery bay count and furniture spec | Yes |
| Opening Cash Buffer | $849,000 | Fixed overhead, payroll ramp, and variable cost load | No |
Surgical Center Core Five Startup Costs
Facility Build-Out Startup Expense
Build-Out Budget
Facility build-out is the biggest capital spending (CAPEX) item here: $15M from Month 1 to Month 6. It covers site selection, lease deposits, plans, permits, operating rooms, procedure rooms, recovery bays, sterile processing, HVAC, medical gas, plumbing, electrical, infection-control finishes, life-safety work, and inspection readiness. Start with $25k monthly lease and $4k utilities in Month 1.
Cost Inputs
Use vendor quotes and room count to price this scope. The key inputs are leased versus owned, shell condition, number of operating rooms, number of recovery bays, medical gas scope, and backup power needs. A rough shell with more rooms or full backup systems pushes the number up fast. Lock scope before permits, because redesigns add delay and cost.
Cost Control
Protect cash by fixing the layout early and matching the build to the actual case mix. A lighter outpatient mix needs less space and equipment than a broad multi-specialty plan. The main mistake is oversizing rooms or changing the plan after architectural work starts. Keep the lease, utilities, and build schedule aligned so Month 1 carry costs do not stack on top of rework.
Scope Checks
Before you size the budget, answer these: leased or owned, shell condition, operating room count, recovery bay count, medical gas scope, and backup power needs. Those inputs drive the biggest swings in cost and timing, and they set whether the $15M base case is realistic or needs a reset.
- Leased or owned facility?
- What is the shell condition?
- How many ORs and bays?
- How much medical gas?
- Need backup power?
Surgical And Anesthesia Equipment Startup Expense
Room Gear
This bucket is the core room setup. Research points to $800k for operating room equipment from Month 3 to Month 7, plus $300k for anesthesia machines, $250k for sterilization gear, and $150k for recovery furnishings. That covers OR tables, lights, monitors, sterilizers, instrument washers, crash carts, and PACU items. Specialty mix drives the spec.
Cost Build
Build the estimate from unit counts, vendor quotes, and install timing. Use the number of ORs, anesthesia stations, sterilizers, and PACU bays, then multiply by unit price and delivery schedule. The timing matters too: sterilization runs Month 2 to Month 4 and recovery furnishings run Month 4 to Month 8. This is a major CAPEX line.
Cash Control
Keep savings tied to scope, not safety. Standardize equipment across rooms where the case mix allows, and phase purchases by opening month so cash follows install milestones. The common mistake is using one equipment list for orthopedics, ophthalmology, GI, pain, ENT, and multi-specialty cases. That can leave expensive gear idle or force last-minute buys.
Specialty Mix
Specialty mix changes the equipment map, so lock the case mix before ordering. Orthopedics, ophthalmology, GI, pain, ENT, and multi-specialty volumes all change what you buy and how much recovery support you need. Match the room build to confirmed procedure demand, not to a generic surgery-center template.
Instruments, Supplies, Pharmaceuticals, And Inventory Startup Expense
Inventory Mix
Keep reusable instruments separate from consumables. Build the line around procedure trays, disposable packs, sutures, gowns, drapes, infection-control supplies, emergency drugs, and implants where needed. The model uses 80% of Year 1 revenue for surgical supplies and 40% for pharmaceuticals, then drops to 60% and 30% by Year 5.
Budget Inputs
Estimate this cost from case mix, monthly volume, and vendor quotes. Use units × unit price for trays, meds, and implants, plus days of coverage for fast-moving stock. Implant-heavy specialties need more cash than lighter mixes, so one blanket ratio will miss the mark.
- Quote implants separately
- Track days of supply
- Update by specialty mix
Reduce Waste
Stock to the schedule, not to fear. Set par levels for consumables, rotate short-dated meds, and buy reusable trays only after the procedure mix is locked. The main mistake is overbuying implants and sterile packs before volume is real. That ties up cash and can expire on the shelf.
- Set par levels
- Rotate short-dated meds
- Avoid early overbuying
Cash Risk
This line sits inside startup cash, not just monthly expense. With higher implant use, inventory can swing hard with only a few cases, so watch vendor terms, consignment options, and replenishment lead times. The right target is enough stock to avoid delays, not a room full of dead cash.
Healthcare Technology And Billing Systems Startup Expense
EHR Setup
This is the setup bucket: $100k EHR implementation and $75k IT/network work, both from Month 1 to Month 3. It covers practice management, ASC EHR, scheduling, revenue cycle, claims clearinghouse, inventory tracking, cybersecurity, phones, computers, printers, and integrations. Treat it as one-time CAPEX, not software overhead.
Recurring Load
The recurring stack starts with a $3k monthly EHR subscription plus 15% of Year 1 revenue in transaction fees. That makes the cost model depend on procedure volume, not just software seats. If Year 1 revenue is still forming, the fee line can outrun the subscription fast.
Cost Control
Keep the build tight. Ask whether billing is in-house or outsourced before locking the stack, because Year 1 also carries a $60k billing specialist. Split vendor quotes into setup, subscription, and transaction fees, then phase noncritical integrations after go-live so you do not pay for tools the team cannot use on day one.
Billing Choice
Billing is a staffing decision, not just a software one. If you keep it internal, budget the $60k specialist; if you outsource, test that cost against the 15% transaction fee and claims flow. Make the call before Month 1 so software, staffing, and reimbursement work together.
Licensing, Accreditation, Insurance, And Readiness Startup Expense
Pre-open costs
This bucket is mostly pre-opening expense, not CAPEX. It covers state licensing, Medicare certification planning, accreditation prep, policies and procedures, legal formation, healthcare compliance counsel, insurance binders, credentialing, recruiting, training, and pre-opening payroll. Budget for $25k regulatory compliance fees and $10k a month for medical malpractice insurance before cases start.
Size the payroll
Start with headcount and months before opening. The model includes a $620k Year 1 salaried payroll base, plus a Center Director at $150k, Head OR Nurse at $100k, Administrative Manager at $80k, and clinical support staffing. That spend sits on top of compliance work and insurance before revenue begins.
Watch approval timing
Keep hiring tied to license, inspection, and payer milestones. If inspections or payer approvals slip, salary, compliance, and insurance burn keeps going with no procedure revenue. One clean rule: don't scale the team past readiness, but do ke ep core leaders in place so policies, credentialing, and mock surveys stay on track.
Ready the team
Readiness costs rise fast when the center is staffed too early. Plan the core team around credentialing, payer approval, and opening date, then add clinical support only when inspections and licenses are close. That keeps the pre-opening cash burn tied to launch progress, not to empty rooms.
Compare 3 Startup Cost Scenarios
Scenario Table
Startup cost moves with room count, specialty mix, recovery capacity, and cash reserve needs. Lean stays small, Base matches the model's core setup, and Full adds more equipment and working capital.
| Scenario | Lean Launchlean single-specialty | Base Launchbase multi-room | Full Launchfull multi-specialty |
|---|---|---|---|
| Launch model | A limited-room, single-specialty setup with a smaller build and tighter working capital. | A multi-room launch built around the model's core capex, timing, payroll, and overhead profile. | A heavier multi-specialty launch with more rooms, more recovery capacity, and a larger cash buffer. |
| Typical setup | Uses lighter equipment, lower inventory, and fewer staffed recovery areas. | Uses the researched $3.345M capex plan, Month 1 to Month 9 spend timing, and Year 1 salaried payroll of $620k. | Adds more equipment, more recovery space, larger inventory, and higher reserve needs. |
| Cost drivers |
|
|
|
| Planning rangeCAPEX only | $2.0M - $2.8MLowest cash need | $3.3M - $4.0MModel baseline | $4.5M - $6.0MHighest reserve |
| Best fit | Best for a narrow procedure mix, slower payer ramp, and one operating room. | Best for a balanced procedure mix, steady payer ramp, and a normal multi-room operating plan. | Best for broader procedure mix, faster payer ramp, and a higher operating room count. |
Planning note: These scenario ranges are researched planning assumptions from the model, not exact vendor quotes or guaranteed bids.
Related Products
- Surgical Center Porter's Five Forces Analysis
- Surgical Center BCG Matrix
- Surgical Center Business Model Canvas
- 7 Essential Surgical Center KPIs for Profitability
- Surgical Center Business Plan Template in Pre-Written Word
- How to Optimize Surgical Center Profitability with 7 Key Strategies
- Running Costs for a Surgical Center: A Monthly Financial Breakdown
- Surgical Center Financial Model Template in Excel
- How Much Does A Surgical Center Owner Make At $194M EBITDA?
- How to Open a Surgical Center: 12–24 Month Launch Roadmap
- How to Write a Surgical Center Business Plan in 7 Steps
- Surgical Center Marketing Mix
- Surgical Center Marketing Plan
- Surgical Center Business Proposal
- Surgical Center PESTEL Analysis
- Surgical Center Pitch Deck Example Editable PPTX
- Surgical Center Business SWOT Analysis
- Surgical Center Value Proposition Canvas
Frequently Asked Questions
Opening this surgical center requires a researched planning estimate of $3345 million in startup CAPEX before working capital The biggest items are $15 million for facility build-out, $800,000 for operating room equipment, and $300,000 for anesthesia machines Full capitalization should also cover pre-opening payroll, insurance, licensing readiness, and cash reserves