 Owner income$140k
Owner income$140kHow Much Does a Veterinary Clinic Owner Make? $140K Pay Plan

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$140k  Net margin-50% to 40%
Net margin-50% to 40% Revenue for target pay$349k
Revenue for target pay$349k Business difficultyHard
Business difficultyHard


A veterinary clinic owner can plan around $140,000 in modeled annual lead veterinarian pay before taxes, with extra take-home only if the clinic has cash left after payroll, overhead, debt service, and reserves In the researched model, annual clinic revenue grows from about $462,180 in the first year to about $304 million in the fifth year Direct variable costs run from 145% of revenue early to 120% at maturity, before payroll and fixed costs These are planning assumptions, not promised salary or required distributions
Owner income$140kNet margin-50% to 40%Revenue for target pay$349kBusiness difficultyHardWant to test your clinic owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to see owner income in the Veterinary Clinic model?
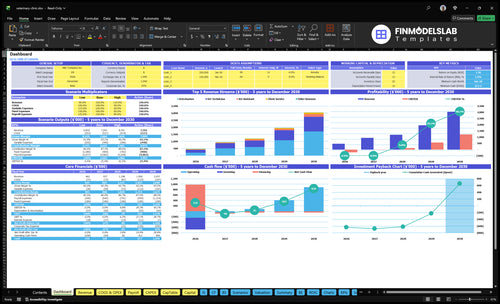
The dashboard shows owner-income outputs, revenue, margin, payroll, fixed costs, and cash reserves in the Veterinary Clinic Financial Model Template—open it to check the assumptions.
Owner-income model highlights
- Owner salary and distributions
- Revenue, margin, and costs
- Scenario tables and reinvestment
Does a veterinary clinic owner make more as the lead veterinarian?
In a Veterinary Clinic, the owner often makes more as the lead veterinarian early on, because their clinical work helps cover the $140,000 lead-veterinarian pay and cuts dependence on a hired doctor. An owner-manager may need a $110,000 associate sooner, which raises payroll and capacity risk, while a 1-to-4 veterinarian model can lift profit potential if recruiting, scheduling, and quality control hold up. Lifestyle only improves if delegation works.
Owner as lead vet
- Supports $140,000 pay with clinical work
- Reduces hired-doctor dependence
- More direct production, less management time
- Works best in the early model
Growth tradeoffs
- $110,000 associate can be needed earlier
- Raises payroll and capacity risk
- Scales from 1 to 4 veterinarians
- Scheduling and training get harder
How much revenue does a veterinary clinic need to pay the owner?
If your Veterinary Clinic needs to pay the owner $140,000, start with about $180,000 in fixed overhead and then add clinical payroll and direct costs; in this model, $462,180 in first-year revenue can support a small owner-led clinic only if volume, staffing, and reserves stay tight. Here’s the quick math: owner pay is not a fixed number, because rent, debt, service mix, and the reserve policy all move the target. Add a $110,000 associate veterinarian and the revenue capacity goes up, but break-even rises too.
Owner pay drivers
- $140,000 target owner pay
- $180,000 fixed overhead
- Clinical payroll adds to break-even
- Rent and debt change the target
Break-even reality
- $462,180 first-year revenue baseline
- Works only with tight volume control
- $110,000 associate raises capacity and cost
- Capacity shifts from 650% to 850%
How much can a veterinary clinic owner take home?
A Veterinary Clinic owner can model $140,000 in lead veterinarian pay before taxes, but distributions come only after expenses, debt service, and reserves; use What Is The Most Important Indicator For The Success Of Your Veterinary Clinic? to keep salary, clinic profit, and cash distributions separate. At $462,180 first-year revenue, cash must cover 145% variable costs, $180,000 fixed overhead, payroll, inventory, and reinvestment, so revenue is not income.
Owner Pay
- Model salary: $140,000 before taxes
- Pay distributions after reserves
- Separate salary from clinic profit
- Track debt service before draws
Cash Check
- Year 1 revenue: $462,180
- Fixed overhead: $180,000/year
- Year 5 revenue: about $304 million
- Show monthly cash after reserves
Which drivers move owner income most?
1
$140KOwner Production
The lead veterinarian sets the core billable load, so owner take-home moves most when doctor time stays full and productive.
2
150-190/moVisit Volume
More monthly treatments per veterinarian lift revenue fast, and the jump from 150 to 190 per month is a big income swing.
3
$180-$220Invoice Value
Higher doctor pricing and richer service mix push each visit to earn more without needing the same jump in patient count.
4
$110KPayroll Mix
Associate veterinarians and technician leverage can grow output, but owner take-home drops if payroll rises faster than visits.
5
12%-15%Direct Costs
Pharmaceuticals, supplies, lab fees, and card fees eat into gross profit, so even small savings flow straight to profit.
6
$15K/moFixed Overhead
Rent, utilities, software, marketing, and other fixed costs must be covered before owner take-home turns healthy.
Veterinary Clinic Core Six Income Drivers
Owner Clinical Production
Owner Clinical Production
Owner clinical production is the fastest way to support early take-home because it drives both revenue and payroll replacement. The model uses $140,000 for lead veterinarian pay, and veterinarian capacity ranges from 650% to 850% productive time. Productive time covers exams, diagnostics, surgeries, care plans, and case management.
Management work does not bill directly, so it has to be scheduled on purpose. If the owner leaves exam rooms too soon, the clinic may need a $110,000 associate veterinarian before volume can cover it. That cuts cash flow and delays owner pay.
Protect Billable Doctor Time
Track how many hours the owner spends on billable care versus management each week. Here’s the quick math: every hour moved from direct care to nonbillable admin raises the chance that paid doctor support is needed sooner, which lowers margin and owner draw. Keep handoffs clean so exams, diagnostics, and surgery stay with the owner until volume can justify a hire.
- Track owner billable hours weekly
- Schedule admin blocks, not gaps
- Watch associate hire timing closely
- Measure handoff loss in visits
If owner production stays high, the clinic keeps more revenue in-house and supports higher early take-home. If management time starts crowding out exam rooms, payroll grows before cash does, and profit gets thinner fast.
1
Appointment Volume And Utilization
Appointment Volume And Utilization
Appointment volume turns clinic capacity into cash. In this model, veterinarian monthly treatments rise from 150 to 190, technician treatments from 200 to 240, and client service interactions from 400 to 480. That lifts revenue only when rooms, staffing, and follow-up work can keep up. If waits, overtime, missed callbacks, or weak rebooking show up, the extra slots can raise stress faster than owner income.
What this means for take-home pay is simple: filled slots improve profit when they use spare capacity, but they hurt profit when they force overtime or create bottlenecks. Wellness care, urgent cases, follow-ups, and repeat visits all help utilization, but the clinic still has to protect service quality. If the team can’t handle the flow, more appointments can mean more labor cost and lower cash left for the owner.
Track utilization by role
Measure doctor slots, tech slots, and front-desk interactions separately, then compare booked volume with actual completions. Here’s the quick check: if treatments go up but waits and overtime rise too, the clinic is overbooked, not more productive.
- Track rebooking after each visit.
- Watch missed callbacks daily.
- Flag overtime by week.
- Split wellness, urgent, and follow-up demand.
- Adjust schedules before burnout starts.
The best schedule fills capacity without breaking the support team. If the clinic can hold 190 veterinarian treatments and 480 client interactions without churn, owner income usually improves; if not, the extra volume just pushes cost and stress higher.
2
Average Invoice And Service Mix
Average Invoice and Service Mix
Average invoice is the cash you collect per visit. If veterinarian pricing moves from $180 to $220, revenue per visit rises 22.2%; technician pricing from $60 to $80 rises 33.3%; assistant pricing from $15 to $19 rises 26.7%. A richer mix of wellness, vaccines, diagnostics, dental care, surgery, pharmacy, and chronic-care follow-up can lift gross profit and owner pay when care plans are complete.
Track Mix, Not Just Visits
Measure average invoice by provider type and by service line each month. The quick rule: more diagnostics, dental, surgery, and chronic-care follow-up should raise invoice more than low-price visits. Ethical care still leads, so revenue growth should come from clear recommendations, compliance, and approved diagnostics, not unnecessary services or hidden add-ons.
- Track invoice per visit weekly.
- Split results by service line.
- Review declined estimates monthly.
3
Payroll Leverage And Staffing Efficiency
Payroll Leverage
Payroll is the biggest owner-income lever after revenue. Wages in the model span $35,000 for an assistant, $45,000 for a technician, $60,000 for a head technician, $110,000 for an associate veterinarian, and $140,000 for a lead veterinarian. When staffing moves from 1 to 4 veterinarians and 2 to 5 technicians, margin rises only if each doctor gets enough trained support to stay billable.
The tradeoff is blunt: too little labor cuts care, slows rooms, and hurts retention; too much labor drags profit. If a doctor is doing tasks a technician or assistant can do safely and legally, owner pay leaks into low-value work. Protect care first, then push routine work down the ladder.
Staff to the Billable Hour
Measure doctor time, technician coverage, overtime, and unpaid admin work each week. Track the ratio of support staff to veterinarians, then compare it with exam-room waits, rebook rates, and client complaints. If waits rise or callbacks slip, the team is too thin; if payroll grows faster than visits, staffing is too heavy.
- Map tasks by role and legality.
- Shift routine work to technicians.
- Hire before bottlenecks break care.
- Trim overtime before cutting heads.
Forecast payroll by doctor count, not by gut feel. A clinic with fewer support staff can look cheap on paper, but it usually loses billable capacity and owner draw. The goal is enough trained help so each veterinarian keeps moving from exam to diagnosis to procedure without dead time.
4
Medical COGS, Lab, Pharmacy, And Supplies
Medical COGS Control
This driver is the clinic’s spend on drugs, vaccines, supplies, outside labs, and card fees tied to each invoice. In the model, pharmaceuticals and vaccines move from 50% to 40% of revenue, medical supplies from 30% to 25%, external lab fees from 40% to 30%, and payment processing stays at 25%. Lower COGS lifts gross margin, so more cash is left for owner pay.
The main inputs are visit volume, service mix, purchase price, lab pricing, inventory turns, expired meds, surgical packs, and charge capture. What this estimate hides: stockouts, waste, and underbilling can wipe out the gain fast. On $304 million revenue, even a 1-point improvement is material; the disclosed model estimate says that saves about $30,373 before taxes.
Tighten Cost per Visit
Track cost by visit type, not just total spend. Watch drug use by doctor, outside lab price lists, and surgical pack standardization. One clean rule: every visit should close with the right charge, the right SKU, and the right lab code.
- Track inventory t urns weekly.
- Review expired meds monthly.
- Audit charges before billing.
- Reprice outside lab panels.
- Standardize surgical packs.
If pharmacy or lab cost trends drift above plan, tighten purchasing, renegotiate fees, or revise protocols before you cut care. The goal is steady gross margin, not fewer tests or lower clinical quality.
5
Fixed Overhead, Equipment, Debt, And Reserves
Fixed Overhead Hits Owner Pay
Fixed overhead is the monthly cost that shows up whether the clinic is busy or slow. Here’s the quick math: $8,500 rent + $1,200 utilities + $950 insurance + $700 software + $1,500 marketing + $600 cleaning and office supplies + $800 maintenance + $750 professional fees = $15,000 per month.
This cost load lowers distributable cash, even when profit looks fine on paper. Equipment leases, loan payments, repairs, and reserves sit below the simple profit view, so owner take-home can shrink fast when cash gets tied up in debt, maintenance, hiring, or inventory.
Track Cash, Not Just Profit
Build a monthly cash view that separates fixed overhead, debt service, and reserve funding. Track rent, utilities, software, marketing, maintenance, and professional fees against the $15,000 baseline, then add lease payments and loan principal so you see what is left for owner pay.
Test the pressure points early: if repairs, new equipment, or slow collections rise, owner draws should fall before vendor bills do. One clean rule helps: do not treat paper profit as spendable cash until debt, reserves, and replacement costs are covered.
6
Compare low, base, and mature veterinary clinic owner-income scenarios
Owner income scenarios
Owner income stays tight at launch, then improves as utilization rises and fixed costs spread. Break-even lands in month 25, so booked doctor hours are the main swing factor.
| Scenario | Low CaseCash-tight | Base CaseBalanced | High CaseScale-dependent |
|---|---|---|---|
| Launch model | Owner income is thin because the clinic is still ramping with one veterinarian and early utilization. | Owner income turns steadier as the clinic reaches two veterinarians and a more normal patient flow. | Owner income climbs fast once the clinic reaches four veterinarians and a mature schedule. |
| Typical setup | One veterinarian, two vet technicians, one vet assistant, one client service rep, and one practice manager run at 65% veterinarian capacity. | Two veterinarians, three vet technicians, one vet assistant, one client service rep, and one practice manager run at 75% veterinarian capacity. | Four veterinarians, five vet technicians, three vet assistants, three client service reps, and one practice manager run at 85% veterinarian capacity. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $0 - $140,000Cash-tight case | $117,000 - $250,000Balanced case | $573,000 - $1,219,000Scale-up case |
| Best fit | Use this to test a slow opening where payroll and rent stay tight before the clinic fully ramps. | Use this for a normal opening path that gets past break-even and starts funding owner take-home. | Use this to test the upside if the clinic fills doctor time fast and absorbs the larger staffing load. |
Planning note: These ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Veterinary Clinic Porter's Five Forces Analysis
- Veterinary Clinic BCG Matrix
- Veterinary Clinic Business Model Canvas
- 7 Essential KPIs to Track for Veterinary Clinic Growth
- Veterinary Clinic Business Plan Template in Pre-Written Word
- 7 Financial Strategies to Increase Veterinary Clinic Profitability
- Analyzing The Monthly Running Costs of a Veterinary Clinic
- Veterinary Clinic Startup Costs: $650K Base Opening Budget
- Veterinary Clinic Financial Model Template in Excel
- How to Open a Veterinary Clinic: 3-Month Buildout Launch Plan
- How to Write a Veterinary Clinic Business Plan: 7 Actionable Steps
- Veterinary Clinic Marketing Mix
- Veterinary Clinic Marketing Plan
- Veterinary Clinic Business Proposal
- Veterinary Clinic PESTEL Analysis
- Veterinary Clinic Pitch Deck Example Editable PPTX
- Veterinary Clinic Business SWOT Analysis
- Veterinary Clinic Value Proposition Canvas
Frequently Asked Questions
The model uses $140,000 in annual lead veterinarian pay before taxes Extra distributions depend on cash left after 120% to 145% direct variable costs, $15,000 monthly fixed overhead, payroll, debt service, and reserves Treat salary and distributions separately, because accounting profit does not always mean spendable cash