 Time to Open6 monthsOpening prep
Time to Open6 monthsOpening prepHow To Open A Veterinary Endoscopy Service With 6 Launch Workstreams

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6 monthsOpening prep  Launch Sequence8 stagesCompliance first
Launch Sequence8 stagesCompliance first Key BottleneckScope delayLead time
Key BottleneckScope delayLead time First Revenue StepScheduled caseReferral booked
First Revenue StepScheduled caseReferral booked


To start a veterinary endoscopy service, define the procedure scope, secure the endoscopy tower and scopes, set anesthesia and recovery workflows, train the clinical team, and build referral intake before scheduling cases The researched planning assumptions show a Year 1 launch with 55% surgeon capacity, 45% internal medicine capacity, and 60% endoscopy technician capacity, so the model expects ramp-up rather than full utilization on day one Launch usually takes several months, mainly because equipment availability, facility readiness, and clinician capability drive the schedule First revenue comes from a booked diagnostic or therapeutic endoscopy case, with pricing assumptions of $3,200 for surgeon-led procedures and $1,800 for internal medicine procedures in Year 1
Time to Open6 monthsOpening prepLaunch Sequence8 stagesCompliance firstKey BottleneckScope delayLead timeFirst Revenue StepScheduled caseReferral bookedLaunch timeline
This is a short web summary of the launch plan, and the XLSX export contains the detailed Gantt chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8
Licensing and compliance
- Define procedure scope
- Map permit needs
- File applications
- Approve SOP set
Equipment and facility
- Order endoscopy tower
- Receive scope inventory
- Install anesthesia gear
- Complete suite buildout
- Set recovery bay
Staffing and training
- Confirm core hires
- Staff technicians
- Train anesthesia team
- Train reprocessing
- Run team drills
Clinical workflow
- Set case criteria
- Build intake forms
- Set pricing sheet
- Configure records
- Dry run workflow
Referral marketing
- Map referral list
- Create outreach kit
- Book clinic visits
- Launch intake pipeline
Go-live readiness
- Confirm pilot cases
- Review pre-op steps
- Check records flow
- Hold launch briefing
- Approve go-live
Will the launch math hold up before opening day?
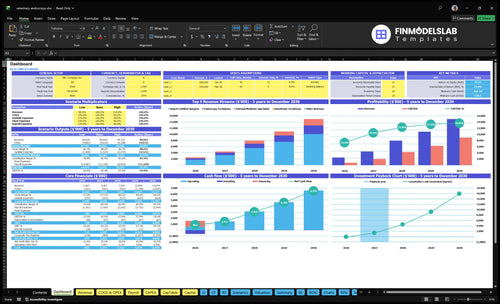
The Veterinary Endoscopy Service Financial Model Template maps revenue, costs, cash needs, assumptions, and break-even logic—open the model.
Financial model highlights
- 55/45/60 utilization test
- $3,200 surgeon-led pricing
- 85% consumables load
- 45% anesthesia supplies
- $18,900 monthly overhead
- Cash runway checks
- Flag slow referrals
- Spot staffing gaps
What do you need to start a veterinary endoscopy service?
To start a Veterinary Endoscopy Service, define the clinical scope first, then build the tower, scopes, imaging, anesthesia, reprocessing, recovery, records, pricing, and referral workflow around those cases; What Are The 5 Core KPIs For Veterinary Endoscopy Service? is the operating scorecard to track launch readiness. In Year 1, the staffing plan is 2 board-certified surgeons, 1 internal medicine specialist, 3 endoscopy technicians, 2 anesthesia technicians, and 1 consulting veterinarian, because uptime depends on trained workflow, not equipment alone.
Core setup
- Define accepted case types first
- Set up tower, scopes, imaging
- Add anesthesia and recovery areas
- Document records and reprocessing steps
Launch team
- 2 board-certified surgeons
- 1 internal medicine specialist
- 3 endoscopy technicians
- Revenue equals treatments × price
What launch mistakes should a veterinary endoscopy service avoid?
For a Veterinary Endoscopy Service, the biggest launch mistake is buying gear before the procedure scope is set. With $18,900/month in fixed overhead before payroll, weak referral flow hurts fast, so Year 1 utilization assumptions of 55%, 45%, or 60% can be too high.
Go-live gates
- Set scope before buying equipment.
- Train intake, prep, and monitoring.
- Test recovery and discharge flow.
- Run cleaning and documentation without confusion.
Common launch misses
- Do not undertrain staff.
- Plan anesthesia and recovery tightly.
- Use clear case selection rules.
- Build referral intake before go-live.
How long does it take to launch a veterinary endoscopy service?
A Veterinary Endoscopy Service usually takes several months to launch, because the opening date moves with equipment ordering, install, facility changes, anesthesia protocols, staff training, and referral readiness. Do not schedule a public launch until the tower, scopes, reprocessing supplies, recovery workflow, and medical record templates are usable. Year 1 should assume ramp-up capacity, not full load, at 55% surgeon, 45% internal medicine, and 60% technician utilization.
Launch timing
- Order equipment first
- Set anesthesia protocols early
- Train staff before opening
- Build referral intake before launch
What slows it down
- Late vendor support delays opening
- Unclear case criteria slows flow
- Unused templates create bottlenecks
- Referral readiness affects day one
Confirm the service is safe, staffed, compliant, and model-ready before go-live
Launch readiness checklist
Use this go-live approval checklist before opening a veterinary endoscopy service.
Compliance
- Board compliance confirmedCritical
State veterinary board rules must be clear before any procedure can start.
- Facility use approvedCritical
The site must allow clinical use before buildout and equipment spend.
- Liability policy activeCritical
Professional liability coverage is listed at $2,500 per month, so it should be bound first.
Suite
- Procedure room completedCritical
The procedure room must be ready before first animal intake.
- Recovery bay readyHigh
A safe recovery space helps reduce post-anesthesia risk after endoscopy.
- Reprocessing flow validatedCritical
Scope cleaning and sterilization must work before any patient is booked.
Equipment
- Endoscope inventory installedCritical
The HD camera system and rigid and flexible scopes must pass setup tests.
- Anesthesia systems testedCritical
Anesthesia workstations and monitoring need a clean pre-opening test.
- Consumable supply stockedHigh
Kits and supplies should cover first cases and avoid launch delays.
Staff
- Surgeon coverage scheduledCritical
Year 1 assumes 55% surgeon capacity, so coverage must match the opening plan.
- Anesthesia team trainedCritical
Anesthesia staffing is a go-live gate because cases depend on safe sedation support.
- Tech roles assignedHigh
Technicians must cover prep, scope handling, and recovery without confusion.
Referrals
- Referral intake liveCritical
A working intake path is needed before specialists can receive cases.
- Pricing and estimates setHigh
Prices must be clear so referring clinics and owners can approve care fast.
- Discharge workflow testedHigh
Discha rge notes and follow-up steps must work before the first case.
Finance
- Cash runway covers launchCritical
Minimum cash is $519k in Month 4, so launch needs enough runway for setup and early losses.
- First-case criteria definedCritical
Do not open until scope, reprocessing, anesthesia support, and vendor backup are clear.
- Go-live signoff completeCritical
Final signoff should confirm staffing, tools, flow, and the first revenue path are ready.
Which launch drivers matter most?
1Procedure Scope
Service menuA written service menu keeps first cases aligned with staffing, pricing, and referral expectations.
2Equipment Readiness
InstalledInstalled, tested gear with backup support prevents first-day downtime and lost referral trust.
3Clinical Staffing
9 staffRole-based training keeps one trained person from becoming the whole workflow and reduces cancellations.
4Anesthesia Recovery
2 techsA tested intake-to-discharge flow reduces unsafe handoffs and protects patient safety on day one.
5Referral Pipeline
5% revReferral intake and follow-up turn clinical readiness into booked cases and faster first revenue.
6Scheduling Ramp
Month 2 BEA conservative ramp model shows whether slots, prices, and cash cover fixed overhead by month 2.
Procedure Scope
Scope First
Launch scope decides whether the clinic can open on time or gets stuck with the wrong tools, the wrong staff mix, and confused referrals. Pick the first diagnostic service menu before buying scopes, then phase more procedures only after the workflow holds. Use planning buckets like gastrointestinal endoscopy, rhinoscopy, and bronchoscopy as launch categories, not clinical promises.
The readiness signal is simple: a written menu with case selection, estimate ranges, staff roles, and referral instructions. If that document is missing, day-one scheduling gets messy and unsuitable first cases will slow the team down.
Build the menu before the gear
Start with the cases you can support cleanly, then match equipment to that scope. Buying scopes before demand is clear is a cash trap, because the wrong setup can sit idle while you still need time, training, and referral volume to fill the schedule. One clean rule: scope the service, then buy the scope.
Document who handles intake, who reviews case fit, and what the referral partner needs to send. That keeps first cases aligned with staffing and avoids day-one delays from unclear approval paths, weak estimates, or last-minute protocol changes.
- List launch procedures first.
- Set estimate ranges upfront.
- Assign staff by role.
- Write referral instructions now.
- Phase extras after workflow stabilizes.
1
Equipment And Vendor Readiness
Equipment and Vendor Readiness
Veterinary endoscopy only opens on time if the tower, scopes, imaging setup, and reprocessing supplies are installed and tested before day one. This is a launch dependency, not a shopping list. If the image fails or a needed consumable is missing, the first procedure can slip, and referral trust drops fast.
The Year 1 model carries 3% of revenue for equipment maintenance and tech support, so opening cash must cover setup, repair access, and vendor response. One bad scope can shut down a procedure block, so confirm repair options and backup support before you book cases.
Test Before You Book
Before marketing procedures, verify tower compatibility, scope count, imaging calibration, reprocessing supplies, installation dates, and who handles maintenance and repairs. Document the vendor contact path for same-day support and a backup plan for missing consumables. The test is simple: run a full mock case and see if every part works without waiting on a part or a call back.
- Test tower, scope, and imaging together.
- Stock reprocessing and case-day consumables.
- Confirm repair and backup support.
- Assign one owner for vendor follow-up.
If any item fails the mock case, delay launch rather than take the first referral with partial setup. That avoids downtime, protects day-one capacity, and keeps referring veterinarians confident the service can handle booked cases.
2
Clinical Staffing And Training
Clinical Staffing And Training
Opening a veterinary endoscopy service on time depends on whether the team can run a safe case flow on day one. The Year 1 plan assumes 2 board certified surgeons, 1 internal medicine specialist, 3 endoscopy technicians, 2 anesthesia technicians, and 1 consulting veterinarian, but local rules and credentials vary, so staffing must match the site’s actual requirements.
The real launch risk is training only one person on the full workflow. Day-one readiness needs role-based training for procedure support, anesthesia coordination, reprocessing, recovery, records, and client communication. If that handoff chain is weak, cancellations rise and the service cannot accept cases safely from the start.
Train the whole workflow
Before opening, verify who can cover each step and who backs them up. The goal is not universal certification; it is role-based readiness so no single employee becomes the bottleneck. One trained person can stall scheduling, delay cases, and force avoidable reschedules.
Use a simple launch check: procedure support, anesthesia coordination, reprocessing, recovery, records, and client communication. If each role is trained and documented, the clinic can start cases safely and keep the first weeks from turning into a stop-start ramp.
- Train backups for every role
- Document day-one responsibilities
- Test handoffs before first case
- Confirm local credential rules
3
Anesthesia, Recovery, And Patient Safety
Anesthesia and Recovery Readiness
Endoscopy opens on time only if the anesthesia and recovery flow is ready before marketing starts. With 2 anesthesia technicians in Year 1, the clinic needs a clear intake-to-discharge path, or the handoff from procedure to recovery becomes the first-day choke point. At the modeled $600 anesthesia price and 45% anesthesia/pharmaceutical supply cost, each case carries about $270 of variable supply expense.
Launch tasks include pre-procedure screening, monitoring, staffing, recovery space, emergency prep, discharge instructions, and documentation standards under veterinary judgment. If that work is not tested before opening, the clinic can be “open” on paper but still unable to safely move patients through day one without delays, cancellations, or a rough owner experience.
Test The Handoff Before Day One
Build the workflow in order: screen, monitor, recover, discharge, document. Write who does each step, what equipment is used, and what triggers escalation, then run a mock case from intake to discharge. The readiness signal is simple: a tested patient flow from intake to discharge with no unclear handoff and no missing supply or staff gap.
- Assign recovery watch before opening.
- Verify emergency supplies and contact steps.
- Use discharge sheets every time.
- Document vitals and handoff timing.
If recovery staffing or documentation is thin, appointments stretch, turnover slows, and marketing can outpace safe capacity. That delays first revenue even when the procedure room is ready.
4
Referral Pipeline
Referral Pipeline
Referral flow is what turns a ready clinic into booked cases on day one. If primary veterinarians, emergency clinics, internal medicine contacts, rescue organizations, and existing clinic clients are not already warmed up, the schedule can stay empty even when the equipment and staff are ready.
Year 1 outreach is modeled at 5% of revenue, so this is a planned launch cost, not a nice-to-have. The main risk is strong clinical setup with no case flow, which delays first revenue and leaves procedure slots underused.
Build Intake Before Outreach
Set the referral intake process before you market. That means owner contact steps, referral forms, required records, estimate process, turnaround expectations, and post-case communication. Keep it simple enough that a referring clinic can send a case without chasing answers.
One clean workflow beats a big outreach list. Test it with a few sample cases and confirm who follows up, when owners hear back, and how fast records are reviewed. If follow-up timing slips, referrals cool off and opening-day capacity gets wasted.
- List eligible cases in plain terms.
- Standardize records before first outreach.
- Set response timing for every referral.
- Track source for each booked case.
5
Scheduling, Pricing, And Revenue Ramp
Scheduling And Revenue Ramp
This driver matters because the clinic only earns when procedure slots match clinician time, anesthesia coverage, recovery, and reprocessing capacity. If the schedule is built before those handoffs are tested, the first cases get delayed, staff sit idle, and the $18,900/month fixed overhead starts burning cash before revenue catches up.
The launch model should separate $3,200 surgeon-led cases, $1,800 internal medicine cases, $450 technician-supported services, $600 anesthesia, and $250 consulting, then test them against 55% surgeon, 45% internal medicine, and 60% technician utilization. One weak assumption here can make day-one demand look healthy while cash still runs tight.
Set The First-Day Slot Grid
Build the first schedule from real blocks, not hope: confirm the room, the clinician calendar, anesthesia staffing, recovery space, reprocessing turn times, and case triage rules. Then test a conservative volume plan that shows ramp-up, cash runway, and the breakeven path before you book marketing or referrals. One clean schedule beats a crowded, fragile one.
- Map case slots to staff.
- Match anesthesia to every case.
- Block recovery and reprocessing.
- Test conservative monthly volume.
- Track cash against fixed overhead.
6
Related Products
- Veterinary Endoscopy Service Porter's Five Forces Analysis
- Veterinary Endoscopy Service BCG Matrix
- Veterinary Endoscopy Service Business Model Canvas
- What Are The 5 Core KPIs For Veterinary Endoscopy Service?
- Veterinary Endoscopy Business Plan Template in Pre-Written Word
- How Increase Veterinary Endoscopy Service Profits?
- What Does It Cost To Run Veterinary Endoscopy Service?
- Veterinary Endoscopy Startup Costs: $118M Opening Budget
- Veterinary Endoscopy Service Financial Model Template in Excel
- Veterinary Endoscopy Service Owner Income: $788K Year 1 EBITDA
- How To Write A Business Plan For Veterinary Endoscopy Service?
- Veterinary Endoscopy Service Marketing Mix
- Veterinary Endoscopy Service Marketing Plan
- Veterinary Endoscopy Service Business Proposal
- Veterinary Endoscopy Service PESTEL Analysis
- Veterinary Endoscopy Service Pitch Deck Example Editable PPTX
- Veterinary Endoscopy Service Business SWOT Analysis
- Veterinary Endoscopy Service Value Proposition Canvas
Frequently Asked Questions
Start by defining the procedure scope, then match equipment, staff, anesthesia, recovery, pricing, and referral intake to that scope The Year 1 model assumes 2 board certified surgeons, 1 internal medicine specialist, and 3 endoscopy technicians It also assumes early utilization of 55% for surgeons and 45% for internal medicine, so ramp-up matters