 Owner income$1.58M
Owner income$1.58MHow Much Does a Veterinary Hospital Owner Make on $364M Year 1 Revenue

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$1.58M  Net margin43.5%
Net margin43.5% Revenue for target pay$3.64M
Revenue for target pay$3.64M Business difficultyHard
Business difficultyHard


Key Takeaways
- More visits spread overhead and lift owner income.
- Higher-acuity mix raises revenue, but adds real costs.
- Doctor productivity drives profit after payroll and support.
- Fixed overhead is $44k monthly before debt.
Owner income$1.58MNet margin43.5%Revenue for target pay$3.64MBusiness difficultyHardWant to test your own owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice. Actual owner income will move with revenue, margin, payroll, debt, taxes, and reserve choices.
Want to check owner income in the Veterinary Hospital model?
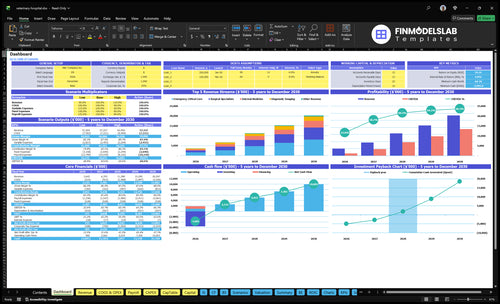
Yes—the Veterinary Hospital Financial Model Template dashboard shows the revenue build, payroll, medical supplies, equipment, debt service, reserves, and owner pay. It charts annual revenue from $364M to $2030M, with cost lines for pharmaceuticals, surgical disposables, lab testing, maintenance, lease, insurance, utilities, software, marketing, cleaning, security, and support wages; open it to test owner cash.
Owner-income model highlights
- Owner cash take-home
- Revenue and cost build
- Scenario cash tests
How much revenue does a veterinary hospital need to pay the owner?
There isn’t one fixed revenue number for a Veterinary Hospital. Use this: required revenue = fixed costs + support payroll + doctor payroll + debt service + reserves + target owner pay, then divide by gross margin after COGS and variable costs; with $528k fixed overhead, $840k support payroll, and 190% direct and variable costs, break-even before owner pay and unlisted doctor payroll is about $169M. At $364M first-year revenue, that leaves about $158M before missing cash claims, and the real driver is appointment volume, average transaction charge, and doctor capacity.
Core math
- Use a revenue formula, not a fixed threshold
- Include owner pay last in the stack
- Listed fixed overhead: $528k
- Listed support payroll: $840k
What drives the answer
- Direct and variable costs: 190%
- Break-even before owner pay: about $169M
- First-year revenue shown: $364M
- Watch appointment volume and doctor capacity
How much can a veterinary hospital owner take home?
A Veterinary Hospital owner’s first-year listed-cost cash flow is about $158M before unlisted doctor payroll, debt, reserves, taxes, and reinvestment, so actual take-home can be much lower; track the operating driver behind that gap in What Is The Most Critical Metric To Measure The Success Of Your Veterinary Hospital?. If the owner also works as a veterinarian, clinical wages can be paid for replacing a hired doctor, but that wage is separate from profit distributions.
Owner Pay
- Start with $158M listed-cost cash flow
- Subtract unlisted doctor payroll
- Separate clinical wages from profit
- Model Hospital Director pay at $180k
Take-Home Limits
- Deduct debt service before draws
- Hold reserves inside the hospital
- Treat retained earnings as cash kept
- Hiring employee specialists cuts owner take-home
What veterinary hospital operating costs affect owner income most?
Owner income in a Veterinary Hospital gets hit most by doctor payroll, technician staffing, and supply costs like specialized pharmaceuticals and surgical implants; for the startup cost context, see How Much Does It Cost To Open A Veterinary Hospital?. Here’s the quick math: first-year COGS is 140%, with pharmaceuticals at 80% and implants/disposables at 60%, while variable expense adds another 50% from lab testing and equipment maintenance.
Top cost levers
- Doctor payroll drives the biggest load
- Technician staffing moves labor fast
- Pharmaceuticals carry 80% COGS
- Surgical implants and disposables hit 60%
Income pressure points
- Lab testing and maintenance add 50% variable expense
- Fixed overhead is $44k per month
- Support payroll is $840k in year one
- Each 1 point of cost on $364M revenue is about $364k cash flow
Want to see the main income drivers?
1
50%-90%Appointment Volume
More booked cases and higher capacity use push revenue up and spread fixed costs over more work, so owner take-home rises after reserves.
2
$800-$4.8KPrice Mix
A bigger share of higher-charge services lifts average revenue per visit, which adds cash without needing the same jump in volume.
3
9-25 FTEDoctor Productivity
When each clinician handles more billable work, payroll goes further and more revenue flows through to take-home before taxes.
4
$1.5M-$2.1MSurgery Mix
Surgery and imaging carry the highest ticket sizes, so mix shifts here move revenue and owner cash faster than routine care.
5
14%-12%Cost Control
Keeping pharmaceuticals, implants, and lab costs tight protects margin directly, and each point saved shows up in owner take-home after reserves.
6
$1.37MFixed Burden
Lease, insurance, software, and support payroll set the cash floor, so lean overhead is what protects owner take-home in early months.
Veterinary Hospital Core Six Income Drivers
Appointment Volume and Capacity
Appointment Volume and Capacity
More completed visits and procedures spread fixed overhead across more revenue, so owner pay rises only when volume grows faster than staffing and room limits. The model uses monthly treatments per clinical FTE, price, and capacity. First-year capacity is about 500% for surgery and anesthesiology, 550% for internal medicine, and 600% for imaging and emergency care.
Mature-year capacity reaches 800% to 900%, but that only helps if doctor availability, exam rooms, technicians, and emergency flow keep up. Overbooking can cut care quality, slow throughput, and damage client trust, which hits repeat demand and profit. If volume rises without control, the owner sees less take-home income, not more.
Track Capacity by Service Line
Watch treatments per clinical FTE by service line, plus room use, tech coverage, and handoff delays. The best signal is whether completed visits rise without longer wait times or missed follow-ups. Here’s the quick math: more completed cases at the same fixed overhead improves margin, but only if staffing and cycle time stay inside safe limits.
- Track bookings, completions, no-shows.
- Cap slots when care slows.
- Staff for peak emergency flow.
- Test price against case mix.
Use service-specific caps, not one hospital-wide target. Surgery, internal medicine, imaging, and emergency care have different capacity ceilings, so the same slot count can be safe in one line and risky in another. If quality slips, the revenue boost can turn into refunds, churn, and lower owner draw.
1
Average Transaction Charge and Service Mix
Average Charge and Service Mix
If your case mix shifts from basic diagnostics to surgery, emergency care, pharmacy, and chronic care, revenue per visit climbs fast. In year one, prices in the mix run from $700 for anesthesiology to $4,000 for surgical specialists; in mature years, that range moves to $850 to $4,800. The catch: higher-acuity cases also raise staffing, inventory, and liability cost.
So the real driver is not just visit count, but average transaction charge and which services make up that charge. Use care plans, clear estimates, and follow-up compliance to keep demand ethical. Don’t push unnecessary procedures. One high-complexity case can lift owner income, but only if gross margin stays ahead of added clinical cost.
Measure Mix, Then Price It Right
Track visits by service line, average charge, estimate acceptance, and recheck compliance. That shows whether revenue is coming from lower-yield work or from surgery and specialty care. Here’s the quick math: if the mix shifts toward services priced near $4,800 instead of $700, top line rises, but only if cost per case does not outrun the margin.
Build forecasts by case type, not just total visits. Include doctor time, technician time, supplies, and follow-up work, because those are the costs that move with acuity. If staffing or inventory is tight, a richer service mix can still hurt cash flow even when revenue looks strong on paper.
- Track charge by service line.
- Watch estimate acceptance rate.
- Price higher acuity fairly.
- Match staff to case mix.
2
Doctor Productivity and Payroll Efficiency
Clinical FTE Productivity
Owner income rises when each clinical FTE (full-time equivalent) produces enough revenue to cover doctor wages, support labor, and overhead. In this model, clinical staffing grows from 9 in year one to 25 in the mature year across five service lines, so the hospital must keep output per doctor high as the team expands.
The inputs are clinical FTEs, production per doctor, support staffing, and the compensation method. Support staff also scales from 8 veterinary technicians and 4 client service representatives to 20 and 10. If hired-doctor payroll is not modeled separately, any distribution number is only a cash-flow ceiling, not true owner take-home pay.
Model Doctor Payroll Separately
Track revenue and margin per clinical FTE by service line, then compare it with doctor payroll and support labor. Here’s the quick test: if headcount grows faster than collected revenue, owner pay gets squeezed fast. One clean rule: more doctors only help when production per doctor stays ahead of wage cost.
Build the forecast with hired-doctor compensation as a separate line from owner draw, then stress test the ramp from 9 to 25 clinical FTEs and from 12 to 30 support staff. If a slow hiring month or weak case volume cuts productivity, the model should show it before you promise distributions.
3
Surgery, Diagnostics, and Medical Complexity
Complex Care Revenue Mix
Complex care drives the hospital’s revenue mix. In this model, first-year surgical revenue is about $960k and emergency care about $162M; by mature year, surgery reaches $608M and emergency care about $808M. Higher-acuity cases can lift the average transaction charge, but they also raise cost and risk.
Profit only improves when utilization is high enough to cover trained staff, equipment, anesthesia protocols, inventory controls, and liability coverage. If those cases stay thin, the extra revenue can look strong while owner take-home drops after direct labor and overhead.
Measure mix before you add complexity
Track the monthly share of surgery, imaging, emergency, internal medicine, and anesthesiology. Pair that with case count, average transaction charge, and utilization. Here’s the quick math: revenue = volume × price. If price rises but slots do not fill, added staffing and compliance cost can wipe out the gain.
- Track case mix by service line.
- Watch doctor and room utilization.
- Price for anesthesia and inventory load.
- Test contribution after direct costs.
Keep estimates and collections tight, because complex care helps cash flow only when booked cases become completed and paid work. If utilization misses plan, hold owner draws conservative until the margin clears the added cost.
4
Medical Supply, Pharmacy, and Lab Cost Control
Supply and Lab Cost Control
Veterinary COGS hit owner cash first. In year one, specialized pharmaceuticals at 80% of revenue and implants and disposables at 60% already total 140% COGS; add 30% for lab testing and external diagnostics and 20% for equipment maintenance, and take-home pay depends on pricing, mix, and control.
The driver includes case count, average charge, drug and implant cost per procedure, lab pass-through, and shrink. Here’s the quick math: revenue per case minus these direct costs funds profit and owner pay. The mature-year benchmark still shows 160% combined COGS and variable costs, so weak purchasing or underpricing can wipe out cash fast.
Track Cost per Case
Measure direct cost share by service line, then test inventory turns, vendor terms, and spoilage. Watch drug cost per case, implant cost per surgery, and what clients are billed for outside lab tests. If the estimate is low, fix the price before the next case, not after month-end.
- Track shrink weekly.
- Review vendor terms monthly.
- Match price to usage.
- Never cut needed care.
5
Fixed Costs, Financing, and Reinvestment
Fixed Overhead and Owner Draw
This driver is the hospital’s monthly fixed cost load before debt, reserves, and reinvestment. The disclosed run rate is $44k per month or $528k per year, and the biggest line is the $25k facility lease. The rest includes $5k malpractice insurance, $4k utilities, $3k property insurance, $25k software, $2k marketing, $15k cleaning, and $1k security.
Here’s the quick math: fixed overhead comes out of operating profit before the owner can pay themselves. If monthly operating profit is $120k, fixed costs leave $76k before loan payments, cash reserves, and reinvestment. If case volume falls, this burden stays flat, so owner income drops fast even when revenue still looks healthy.
Track the Cash Waterfall
Build a monthly bridge from revenue to distributable cash. Track fixed overhead, then subtract debt service, reserve builds, and reinvestment separately so you can see what is left for the owner. The key input is whether treatment volume and pricing can cover the $44k base load without squeezing pay.
- Watch lease renewals first.
- Forecast software and utilities monthly.
- Set reserve targets before draw.
- Review fixed cost per case.
6
Scenario objective: compare lean, base, and high veterinary hospital owner income outcomes
Owner income scenarios
Owner income swings hard here because launch-month ramp, specialist staffing, and heavy fixed costs can absorb cash before the hospital reaches mature volume. The gap between early use and full capacity drives how much the owner can draw.
| Scenario | Low CaseRamp pressure | Base CaseCore plan | High CaseUpside case |
|---|---|---|---|
| Launch model | The low case keeps owner income tight during the launch ramp. | The base case models the middle path for owner income once operations stabilize. | The high case reflects stronger volume and a larger owner draw once the hospital matures. |
| Typical setup | Year 1 runs at a heavy ramp, with 500% to 600% capacity, 190% COGS plus variable costs, $840k support payroll, and $528k fixed overhead before doctor pay, debt, reserves, and taxes. | The business runs at mid-model scale, with revenue around $1129M and 174% COGS plus variable costs, so owner pay depends on keeping staffing, overhead, and reserves in line. | The mature path uses about $2030M revenue with 160% COGS plus variable costs, which supports more owner income if debt and reserves stay covered. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Thin or negative drawEarly ramp cash | Mid-model draw capacityStable owner draw | Higher draw capacityMature upside |
| Best fit | Use this to stress-test launch months, reserve needs, and whether the owner can avoid taking distributions early. | Use this as the planning case for budgeting, lender talks, and owner pay policy. | Use this to test upside staffing, reinvestment, and how much cash the owner can keep after reserves. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Veterinary Hospital Porter's Five Forces Analysis
- Veterinary Hospital BCG Matrix
- Veterinary Hospital Business Model Canvas
- Tracking 7 Core Financial Metrics for a Veterinary Hospital
- Veterinary Hospital Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Veterinary Hospital Profitability
- How to Manage the Monthly Running Costs of a Veterinary Hospital
- Veterinary Hospital Startup Costs: $133K Monthly Readiness Before Launch
- Veterinary Hospital Financial Model Template in Excel
- How To Open A Veterinary Hospital: 6–12+ Month Launch Roadmap
- How to Write a Veterinary Hospital Business Plan in 7 Steps
- Veterinary Hospital Marketing Mix
- Veterinary Hospital Marketing Plan
- Veterinary Hospital Business Proposal
- Veterinary Hospital PESTEL Analysis
- Veterinary Hospital Pitch Deck Example Editable PPTX
- Veterinary Hospital Business SWOT Analysis
- Veterinary Hospital Value Proposition Canvas
Frequently Asked Questions
In the researched first-year model, revenue is about $364M and listed-cost cash flow is about $158M before doctor payroll, debt service, reserves, and taxes That is not guaranteed take-home Actual owner income depends on whether the owner works clinically, hires specialists, keeps cash in reserves, or reinvests in equipment