 Owner income$0–$136k
Owner income$0–$136kHow Much Does A VR Therapy Center Owner Make? 5-Year View

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$0–$136k  Net margin-157% to 307%
Net margin-157% to 307% Revenue for target pay$596k
Revenue for target pay$596k Business difficultyHard
Business difficultyHard


Key Takeaways
- Utilization drives revenue and speeds break-even.
- Session pricing caps revenue, but mix can lift it.
- Staffing is the biggest controllable margin cost.
- High software, marketing, and overhead pressure early profit.
Owner income$0–$136kNet margin-157% to 307%Revenue for target pay$596kBusiness difficultyHardWant to test your owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the VR Therapy Center model?
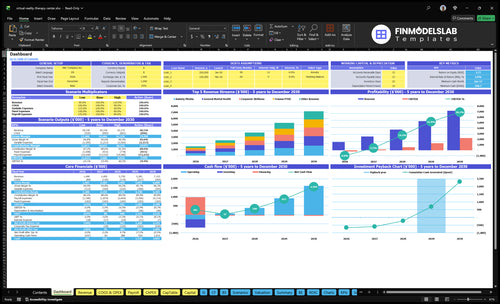
See the VR Therapy Center Financial Model Template for revenue, EBITDA, cash runway, break-even, payback, and owner take-home.
Owner-income model highlights
- Therapist, pricing, utilization tabs
- Payroll, fixed costs, capex
- Low, base, high cases
- $124k to $596k revenue
- EBITDA -$234k to $2198M
- Month 14 break-even
- 41-month payback
How much revenue can a VR therapy center make per month?
VR Therapy Center can bring in about $124k/month in Year 1 and about $596k/month by Year 5, and that is revenue, not profit or owner income. Year 1 session prices run about $175 to $200, then rise to $195 to $220 in Year 5. The actual booked count still moves with cancellations, intake speed, room availability, and referral flow, so the top line can swing fast.
Year 1 revenue drivers
- 12 therapists across five programs
- $124k/month model revenue
- $175 to $200 per session
- Booked sessions depend on intake speed
Year 5 scale factors
- $596k/month model revenue
- $195 to $220 per session
- Higher staffing supports more volume
- Room use and referrals cap growth
What affects VR therapy center profit margin?
VR Therapy Center margin comes down mostly to payroll, utilization, payer mix, and tech overhead; see How Much Does It Cost To Open A VR Therapy Center?. Here’s the quick math: Year 1 EBITDA margin is -157%, then 55% in Year 2 and 307% in Year 5, while recurring percentage costs fall from 135% of revenue to 92%. Fixed overhead starts at $15,250/month before payroll, and annual payroll rises from about $116M to $3165M, so full schedules and strong reimbursement matter most.
Margin drivers
- Payroll moves margin fastest.
- Utilization fills billable sessions.
- Payer mix changes collected revenue.
- Tech overhead cuts margin when high.
Key cost points
- Fixed overhead starts at $15,250/month.
- Year 1 EBITDA is -157%.
- Year 2 EBITDA reaches 55%.
- Year 5 EBITDA reaches 307%.
Can a VR therapy center owner make more by scaling locations or providers?
For a VR Therapy Center, scaling providers usually grows revenue faster than staying owner-operated, but it can shrink the founder’s near-term take-home because paid management replaces owner labor. This model uses a $120k Clinical Director, $95k Lead VR Therapists, and $80k General VR Therapists, plus admin, IT, and outreach staff; revenue rises from $149M to $715M over five years, while payroll rises from $116M to $3165M. So the owner makes more only when added provider capacity fills enough sessions to cover the heavier staff bill.
Owner-led cash
- Owner work keeps payroll lowest.
- Take-home stays highest near term.
- Growth depends on founder hours.
- Less management, less overhead.
Scaled provider model
- Clinical Director costs $120k.
- Lead VR Therapists cost $95k.
- General VR Therapists cost $80k.
- More staff lifts revenue fast.
Want the six main income drivers?
1
60%-70%Utilization
Year 1 fill rates at 60%-70% decide how much therapist time turns into revenue, and higher booked time lifts take-home fast.
2
$1.16MClinician Payroll
Year 1 clinician pay totals about $1.16M, so staffing is the biggest cash drag unless sessions stay full.
3
$175-$200Session Price
Year 1 session pricing sits in the $175-$200 range, so even small price gains flow straight into margin.
4
$15.25K/moOverhead
Fixed overhead runs about $15.25K a month, so empty slots hurt fast and full schedules help absorb rent, software, and support.
5
4.5%-3.0%Payer Mix
Better referrals and lower paid marketing can cut patient acquisition cost from 4.5% to 3.0% of revenue, which protects cash.
6
Month 14Scale
Breakeven lands in Month 14, so owner income stays tight until the clinic reaches steady volume and the cost base is covered.
VR Therapy Center Core Six Income Drivers
Utilization
Booked Session Utilization
Utilization is the share of available VR therapy slots that get booked and kept. For this center, it drives revenue without raising rent: Year 1 utilization is 60% to 70%, and Year 5 rises to 83% to 90%. Higher booked volume spreads the $15,250 monthly fixed overhead and salaried clinician costs across more sessions, which lifts margin and owner pay.
Here’s the quick math: if session price stays flat, profit rises mainly when more of the calendar is filled. Weak utilization leaves the same fixed costs chasing fewer sessions and can push break-even past Month 14. The main inputs are booked sessions, cancellations, therapist availability, room use, and referral flow.
Keep Slots Filled
Track utilization by therapist, room, and program, not just center-wide. A tight target is the gap between scheduled and completed sessions, because no-shows and open slots both hit cash flow. If intake slows or cancellations spike, the owner’s draw gets squeezed fast.
The fix is operational, not financial. Tighten intake, keep provider calendars full, and match room schedules to demand so each hour earns before fixed payroll does.
- Booked slots ÷ available slots
- Cancellation and no-show rate
- Referral volume by source
- Provider hours used
- Same-week rebook rate
1
Average Session Revenue
Average Session Revenue
For a VR therapy center, average session revenue is the average dollars collected per booked hour. It sets the ceiling for top-line growth before labor and overhead. In Year 1, pricing runs from $175 for corporate wellness to $200 for trauma and PTSD sessions; by Year 5, that range rises to $195 to $220.
Monthly revenue = booked sessions × average session revenue. A shift from $175 to $200 lifts revenue by about 14% at the same volume. Price mix matters, because specialty programs, cash-pay packages, insurance contracts, and group formats can push the blended average up; lower-priced mix does the opposite and cuts what the owner can draw.
Raise Blended Session Price
Track realized revenue per session by program, not just posted rates. Split results across corporate wellness, trauma/PTSD, specialty work, group formats, and contract channels so you can see whether the blend is holding near plan. If the average slips, the fix is usually mix, package design, or pricing discipline, not more volume.
Use the higher end of the range on sessions that need more therapist time or specialty skill. One clear rule: more booked hours only help if the average price stays high enough to cover salaried clinician cost, room cost, and fixed overhead. If the mix shifts down, cash flow tightens fast even when the calendar stays full.
2
Clinician Staffing Cost
Clinician Payroll Cost
Therapist payroll is the biggest controllable margin lever because it sets the fixed cost base behind every booked session. The listed team mix is a $120k Clinical Director, 2 Lead VR Therapists at $95k each, and 8 General VR Therapists at $80k each, or $950k in base pay before benefits, taxes, and overtime. If volume is soft, that fixed load cuts owner draw fast.
Control Payroll per Session
Track payroll per session, not just headcount, and add staff only when booked hours justify it. If demand is uncertain, use contractors or productivity pay so labor moves with revenue. One clean rule: keep hiring tied to utilization and rebook rates, because unused clinician hours turn straight into margin drag.
- Track sessions per clinician weekly.
- Watch payroll as revenue percent.
- Use variable labor for spikes.
3
Technology And Facility Overhead
VR Tech and Facility Overhead
VR equipment, software, and build-out hit cash first and profit later. This center needs $455k upfront capex, including $75k for headsets and controllers, $120k for VR computers, $40k for network infrastructure, $90k for build-out, and $30k for initial software licenses. For the owner, that means less free cash early and a longer path to take-home pay.
The bigger drag is recurring tech cost. Software licensing and content royalties run at 60% of revenue in Year 1 and 37% by Year 5, so every $1 of sales leaves only $0.40 before other overhead in Year 1. Replacement cycles and privacy systems also cut distributable profit, so session volume has to rise fast just to keep owner draw stable.
Track Tech Burn Per Session
Measure tech cost per booked session, not just total spend. The key inputs are session volume, revenue, software royalty rate, device replacement timing, and privacy compliance cost. If volume is soft, 60% of revenue going to software in Year 1 can wipe out margin fast, so the owner should test pricing and utilization before adding more hardware.
Keep a monthly check on capex runway and device life. The quick test is simple: if software and content cost stay at 37% to 60% of revenue, the business needs enough gross profit after tech to cover payroll, rent, and the owner’s draw. Delay upgrades that do not improve session capacity or patient retention.
4
Payer Mix And Referrals
Payer Mix And Referrals
Payer mix is the split between employer programs, physician referrals, veterans programs, schools, clinics, direct-to-consumer patients, and insurance vs cash pay. It changes both session volume and how much revenue actually lands in the bank. In Year 1, patient acquisition marketing can run at 45% of revenue; by Year 5, that drops to 30% if referrals do more of the work.
Strong referral channels lower paid ads, so gross margin and owner pay improve. Insurance-heavy volume can still fill the calendar, but it may add billing friction and slower collections, which hurts cash flow even when reported revenue looks fine. One clean line: more referrals usually mean less cash burned to book the same session.
Shift Toward Referral-Led Volume
Track revenue and booked sessions by channel every month, then compare marketing spend to revenue and cash collected. The key question is simple: which channel brings the best mix of fill rate, margin, and fast payment? If one source drives volume but drags collections, it can weaken profit and the owner’s draw.
- Track source mix monthly
- Watch marketing as % revenue
- Measure cash collection lag
- Compare fill rate by channel
Test channel mix, not just headcount. Push physician, veteran, school, clinic, and employer referrals where fit is strongest, and use direct-to-consumer only where paid acquisition still pencils out. A practical target is to move marketing from 45% of revenue toward 30% as referral volume rises.
5
Owner Role Or Scale
Owner Role vs. Scale
Owner-operated income can look higher early because the founder replaces paid labor, but only if the owner is licensed and can carry the clinical load. In this model, the owner’s take-home is what’s left after sessions, support, and overhead; if workload gets too heavy, revenue can rise while burnout and missed visits cap profit fast.
Managed scale is cleaner: this model starts with a $120,000 Clinical Director from launch month, then adds providers to raise capacity. That can grow revenue, but management, admin, IT, marketing, and supervision costs rise with each hire, so margin only improves if session volume keeps pace.
Track licensed hours, not just revenue
Measure booked sessions, provider utilization, and payroll as a share of revenue. The quick math is simple: owner pay improves when added clinician hours lift revenue faster than the $120,000 director cost and extra support costs. If the founder is also the clinician, track whether that labor is creating profit or just replacing a salary.
- Track sessions per licensed hour
- Separate owner labor from profit
- Test hire timing against volume
- Forecast supervision and admin load
6
Compare low, base, and high VR therapy center owner income scenarios
Owner income scenarios
Owner income changes fast here because Year 1 is loss-making, Year 2 reaches breakeven territory, and mature volume can support much larger draws.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | Utilization ramps slowly and Year 1 stays in EBITDA loss, so owner pay stays paused. | Operations reach Month 14 breakeven and Year 2 EBITDA turns positive, allowing a cautious owner draw after reserves. | Higher utilization and mature staffing lift Year 5 EBITDA to $2.198M, creating the strongest owner pay path. |
| Typical setup | The center opens with full fixed overhead, heavy therapist staffing, and slower patient flow before reserves are rebuilt. | Therapist count, treatment volume, and blended pricing reach the modeled base case while fixed costs stay covered. | The clinic runs near capacity across all service lines, with pricing and volume up and fixed overhead spread across more treatments. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | No owner distributionNo draw | Cautious owner drawCautious draw | Strong owner drawStrong draw |
| Best fit | Use this to stress-test survival if bookings lag and cash stays tight. | Use this for a steady operating plan with limited distributions until cash is safe. | Use this to test upside if demand, staffing, and capacity all stay on track. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- VR Therapy Center Porter's Five Forces Analysis
- VR Therapy Center BCG Matrix
- VR Therapy Center Business Model Canvas
- 7 Critical KPIs to Measure VR Therapy Center Performance
- VR Therapy Center Business Plan Template in Pre-Written Word
- 7 Strategies to Increase VR Therapy Center Profitability
- How Much Does It Cost To Run A VR Therapy Center Monthly?
- VR Therapy Center Startup Costs: $455K CAPEX Plus $269K Cash Need
- VR Therapy Center Financial Model Template in Excel
- How To Open A VR Therapy Center In 4-9 Months With First Patients
- How to Write a Business Plan for a VR Therapy Center
- VR Therapy Center Marketing Mix
- VR Therapy Center Marketing Plan
- VR Therapy Center Business Proposal
- VR Therapy Center PESTEL Analysis
- VR Therapy Center Pitch Deck Example Editable PPTX
- VR Therapy Center Business SWOT Analysis
- VR Therapy Center Value Proposition Canvas
Frequently Asked Questions
The model reaches break-even in Month 14 That timing depends on reaching about $124k monthly revenue in Year 1, then growing toward $208k monthly revenue in Year 2 The biggest swing factors are clinician utilization, payroll timing, payer mix, and whether startup cash covers the $269k minimum cash point