 Owner income$1.19M
Owner income$1.19MHow Much Weight Loss Center Owners Make: $0 To $460K By Year 3

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$1.19M  Net margin-181% / 69% / 256%
Net margin-181% / 69% / 256% Revenue for target pay$88k/mo
Revenue for target pay$88k/mo Business difficultyHard
Business difficultyHard


This five-year US model estimates weight loss center owner income from revenue, payroll, rent, marketing, program costs, and capacity use Using the provided assumptions, owner take-home before taxes, debt service, reserves, and distributions is negative in the first year, about $74,034 in Year 2, and about $460,755 in Year 3 This is business-owner planning, not tax, clinical, or legal advice
Owner income$1.19MNet margin-181% / 69% / 256%Revenue for target pay$88k/moBusiness difficultyHardWhat could your weight loss center pay you?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Actual owner income depends on revenue, margin, payroll, taxes, debt, and reinvestment. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to test the owner-income math in a Weight Loss Center model?
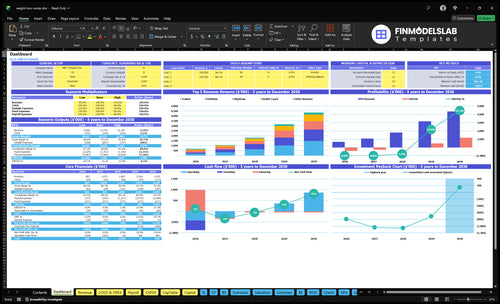
This Weight Loss Center Financial Model Template shows revenue, margin, payroll, overhead, cash before reserves, and owner take-home. Open it as the next planning step.
Owner-income model highlights
- Owner income output
- Revenue and margin charts
- Staffing and scenario inputs
How much revenue does a weight loss center need?
A Weight Loss Center needs about $1.45 million a year to support $150,000 in owner pay, or about $121,175 a month, before taxes, debt, and reserves. For $300,000 in owner pay, the target rises to about $1.62 million a year, or $135,204 a month. That sits on a Year 3 cost base of $1,145,600 a year in fixed overhead plus payroll, and the needed sales level shifts with service mix and visit volume.
Year 3 cost base
- $1,145,600 fixed overhead plus payroll
- 109% variable plus delivery costs
- $150,000 owner pay target
- $121,175 monthly revenue target
Higher owner pay
- $300,000 owner pay target
- $1.62 million annual revenue target
- $135,204 monthly revenue target
- Service mix changes the sales level
Can a weight loss center be profitable?
Yes, a Weight Loss Center can be profitable, but not automatically: the researched base case runs at about -$124,370 in Year 1 before taxes, debt, and reserves, then improves to $74,034 in Year 2 and $460,755 in Year 3; for demand context, see What Is The Current Growth Trend Of The Weight Loss Center?. The profit gap comes down to paid volume, repeat clients, premium programs, and tight payroll control.
Profit Reality
- Year 1: about -$124,370
- Year 2: about $74,034
- Year 3: about $460,755
- Before taxes, debt, and reserves
Main Levers
- Grow recurring client visits
- Sell premium service packages
- Control added manager payroll
- Treat founder labor as real cost
What weight loss center expenses reduce owner income most?
Payroll is the biggest hit to owner income at a Weight Loss Center, rising from $455,000 in Year 1 to $875,000 in Year 3 and $1,605,000 in Year 5; for the startup-cost context, see What Is The Estimated Cost To Open Your Weight Loss Center? Marketing is also heavy at 80% of revenue in Year 1 and 70% in Year 3, while rent runs $15,000/month inside $22,550/month fixed overhead. Smaller lines like lab testing, materials, supplements, and consumable supplies still cut cash before owner pay, so every dollar has to come from booked consultations and paying clients.
Payroll Pressure
- $455,000 payroll in Year 1
- $875,000 payroll in Year 3
- $1,605,000 payroll in Year 5
- Listed wage lines drive the rise
Other Cash Drags
- Marketing takes 80% of revenue in Year 1
- Marketing is still 70% in Year 3
- Rent is $15,000/month
- Fixed overhead is $22,550/month
What drives weight loss center owner income?
1
$82K/moClient Volume
More active clients fill the monthly schedule and drive the top line before staffing and rent hit take-home.
2
$75-$410Price Mix
A bigger share of higher-priced physician and health-coach visits lifts average revenue per client without the same visit count.
3
580/moVisit Flow
Repeat visits and program completion keep the calendar full and make revenue less dependent on new-client spikes.
4
$655KPayroll Load
Year 1 wages are the biggest cost block, so staffing faster than demand can wipe out owner profit.
5
8%-6%Marketing Cost
Acquisition spend falls from 8.0% to 6.0% of revenue, so better booking efficiency leaves more cash in the business.
6
$22.6K/moFixed Base
With fixed overhead at $22,550 a month, each extra dollar above break-even flows more cleanly to owner take-home.
Weight Loss Center Core Six Income Drivers
Active Client Volume
Active Client Volume
Paying active clients are the revenue engine here, not website traffic. In the model, monthly treatments, provider counts, and booked capacity drive revenue to $57,260/month in Year 1 and $150,239/month in Year 3.
Here’s the quick math: as utilization climbs from 550%–650% early to 650%–750% by Year 3 across roles, each filled slot spreads rent and payroll across more sales. Weak conversion or missed appointments cuts owner take-home fast because fixed costs keep running.
Fill Paid Slots, Not Traffic
Track active paying clients, monthly treatments delivered, no-show rate, and booked capacity by provider. If consult volume looks good but paid visits lag, the business is leaking income before it reaches the P&L. One clean metric: kept appointments per provider per month.
Use the model to test what happens when conversion slips or cancellations rise. A small drop in filled visits can leave rent, payroll, and clinical time underused, which hits cash flow fast. Protect owner income by rebooking fast, confirming visits, and watching capacity by role every week.
- $57,260 Year 1 monthly revenue
- $150,239 Year 3 monthly revenue
- 550%–650% early utilization
- 650%–750% Year 3 utilization
1
Average Revenue Per Client
Average Revenue Per Client
Average revenue per client is the mix-weighted price you collect from each active client. In year 1, one physician visit, one dietitian visit, one trainer session, one health coach session, and one coordinator session totals $785; by year 5, the same basket totals $905, a rise of $120 or about 15%.
This driver matters because higher revenue per client helps cover $22,550 in monthly fixed overhead and payroll. Premium programs, memberships, consultations, and product add-ons only help if clients buy and complete them; weak completion leaves billed capacity on the table and slows owner pay.
Price Mix and Attach Rate
Track average billed revenue per active client and the share of sales by service type. Here’s the quick math: average revenue per client = total service revenue ÷ active clients. If the mix shifts toward physician visits or add-ons, revenue rises; if clients stay on lower-priced sessions, it falls.
- Visits sold by service type
- Add-on attach rate
- Program completion rate
- Active client count
- Cancellations and reactivations
Set pricing by package, then check booked revenue each month. If onboarding or follow-up is weak, clients buy fewer sessions and average revenue drops even when lead flow looks fine. Price changes should show up in revenue fast, or the mix is too thin.
2
Retention And Recurring Revenue
Retention And Recurring Revenue
Retention matters because this model depends on repeat monthly treatments across physicians, dietitians, trainers, health coaches, and coordinators. More repeat visits make monthly revenue steadier and lift lifetime value, so the owner has less pressure to replace lost clients just to stay flat.
Here’s the quick math: if clients keep showing up, booked capacity stays full and take-home income improves. If follow-up slips, empty slots still carry rent and payroll. Monthly fixed overhead is $22,550, so weak retention can turn into cash strain fast even when top-line sales look okay.
Track Repeat Visits Closely
Measure retained active clients, completed visits, cancellations, and reactivations. Those four inputs tell you whether recurring revenue is real or just booked on paper.
Use a simple rule: if completions drop while cancellations rise, revenue quality weakens and owner pay gets less predictable. Better follow-up and rebooking protect monthly cash flow because each kept client reduces replacement pressure and helps spread fixed costs over more billed visits.
- Track active clients monthly.
- Watch visit completion rates.
- Flag cancelled appointments fast.
- Reactivate lapsed clients early.
3
Staffing And Owner Role
Staffing and Owner Role
Staffing is where profit becomes real, or gets eaten by founder labor. The model shows payroll of $455,000 in Year 1, $875,000 in Year 3, and $1,605,000 in Year 5, before any unlisted coordinator wage line. That is about $37.9k, $72.9k, and $133.8k per month, so every hire needs booked visits to pay for itself.
Owner-led sales or coaching can save cash, but the owner’s time still has a cost. Hiring providers, coaches, front desk, managers, and clinical oversight cuts founder workload, yet it pushes the break-even point higher. If staffing grows faster than paid client volume, take-home pay drops even when revenue looks busy.
Track Payroll Against Delivered Visits
Build staffing from booked treatments, not from wishful headcount. Track loaded pay (wage plus taxes and benefits) by role, owner hours, visits per provider, cancellations, and reactivations. If a role does not lift revenue, retention, or capacity enough to cover its cost, it is a cash drag, not a growth move.
- Track payroll dollars per booked visit.
- Separate owner labor from true profit.
- Measure utilization by role each month.
- Test part-time before full-time hires.
Use the owner for high-value sales, supervision, or missed-visit recovery only when that work raises booked volume or repeat visits. Otherwise, delegate admin first. The goal is simple: keep staffing tight enough that profit stays cash the business can actually pay out.
4
Marketing Efficiency
Marketing Efficiency
Marketing efficiency is the share of spend that turns into booked consultations and paying clients. In this model, client acquisition marketing is 80% of revenue in Year 1, 70% in Year 3, and 60% in Year 5, or about $54,970, $126,201, and $261,111 a year. If leads do not book and close, ad spend pulls down owner pay fast.
What matters is referral mix, lead quality, close rate, and local competition. Here’s the quick math: more booked consults at the same spend lift revenue and help cover staff and rent; weak conversion leaves the owner funding traffic that never reaches the schedule.
Track booked consults, not clicks
Track cost per booked consult, consult-to-client close rate, and where each lead came from. If one channel brings cheap clicks but few bookings, cut it. If referrals close better than ads, shift spend there. The goal is simple: every dollar of marketing should create enough paying visits to cover delivery costs and leave profit for the owner.
Also watch cancellations and no-shows. A booked consult that never happens is dead spend, and a low show rate can erase margin even when lead volume looks strong. When competition is tight, the business may need better targeting, better follow-up, or higher-priced packages to keep marketing from eating take-home income.
5
Fixed Overhead Utilization
Fixed Overhead Load
Fixed overhead is the bill you owe before sales can help you. Here, it is $22,550 a month: $15,000 rent, $2,500 utilities, $1,500 maintenance, $1,000 malpractice insurance, $800 software, plus admin costs. If capacity is not full, that cost hits owner pay fast.
The pressure eases only when gross profit covers those fixed costs with cash left over. Fixed overhead equals 394% of first-year revenue, 150% of Year 3 revenue, and 62% of Year 5 revenue. So even when sales grow, high rent can still erase take-home if volume and pricing do not rise together.
Track Coverage, Not Just Sales
Measure monthly revenue, gross profit, and fixed-cost coverage first. Coverage means the gross profit left to pay rent and overhead. If that cushion is thin, owner income stays weak even when the schedule looks busy.
- Track revenue versus $22,550 fixed costs.
- Watch empty slots by provider.
- Fill schedules with repeat visits.
- Test rent against local demand.
- Cut admin waste before adding staff.
When overhead is this heavy, every unused treatment slot matters. Better retention spreads rent across more visits, which protects cash flow and makes owner pay more stable.
6
Compare low, base, and high owner-income scenarios
Owner income scenarios
Owner income changes fast here because payroll, fixed overhead, and treatment volume ramp at different speeds. The low case stays under pressure; the base and high cases show what scale can do.
| Scenario | Low CaseLower earnings | Base CaseModeled case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the early-ramp case where the center runs below full use and owner income stays negative. | This is the modeled growth case where the center reaches steady use and turns meaningfully profitable. | This is the stronger scale case where the center runs near mature capacity and owner income climbs fast. |
| Typical setup | First-year revenue is $687,120 with heavy listed payroll of $455,000, fixed overhead of $270,600, and operating income of -$124,370 before owner draws. | Year 3 revenue reaches $1,802,868 with operating income of $460,755 before taxes, debt, reserves, and distributions. | Year 5 revenue reaches $4,351,848 with operating income of $2,071,526 before taxes, debt, reserves, and distributions. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | -$124,370Downside plan | $460,755Core plan | $2,071,526Upside plan |
| Best fit | Use this to stress test the launch period if patient volume and staffing efficiency lag. | Use this as the core planning case for budgeting, hiring, and cash needs. | Use this to test upside if demand holds, staffing scales, and capacity stays full. |
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. All figures are before taxes, debt, reserves, and owner distributions.
Related Products
- Weight Loss Center Porter's Five Forces Analysis
- Weight Loss Center BCG Matrix
- Weight Loss Center Business Model Canvas
- 7 Financial KPIs to Scale Your Weight Loss Center
- Weight Loss Center Business Plan Template in Pre-Written Word
- Increase Weight Loss Center Profitability: 7 Actionable Strategies
- How Much Does It Cost To Run A Weight Loss Center Monthly?
- Weight Loss Center Startup Costs: $448K CAPEX Planning Guide
- Weight Loss Center Financial Model Template in Excel
- How To Open A Weight Loss Center In 3–6 Months With Launch Steps
- How to Write a Weight Loss Center Business Plan (7 Steps)
- Weight Loss Center Marketing Mix
- Weight Loss Center Marketing Plan
- Weight Loss Center Business Proposal
- Weight Loss Center PESTEL Analysis
- Weight Loss Center Pitch Deck Example Editable PPTX
- Weight Loss Center Business SWOT Analysis
- Weight Loss Center Value Proposition Canvas
Frequently Asked Questions
The model shows no safe first-year owner pay from operating profit because income is about -$124,370 before taxes, debt, and reserves Year 2 improves to about $74,034, and Year 3 reaches about $460,755 Those figures are planning outputs, not guaranteed salary or distributable cash