 Owner income$2.70M
Owner income$2.70MHow Much X-Ray Imaging Service Owners Make: $26M EBITDA

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$2.70M  Net margin63.6% to 75.9%
Net margin63.6% to 75.9% Revenue for target pay$4.07M
Revenue for target pay$4.07M Business difficultyHard
Business difficultyHard


An X-ray imaging service owner can plan around a $110k clinic director salary plus possible distributions from operating profit In the researched base model, the clinic produces $4067M in Year 1 revenue and $2588M in EBITDA, a 636% EBITDA margin Take-home is not the same as revenue or EBITDA because equipment financing, cash reserves, taxes, and reinvestment come first The biggest swing factors are paid exam volume, net collection per exam, read fees, technologist payroll, and fixed overhead
Owner income$2.70MNet margin63.6% to 75.9%Revenue for target pay$4.07MBusiness difficultyHardWant to test your X-ray owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to see the X-ray financial model?
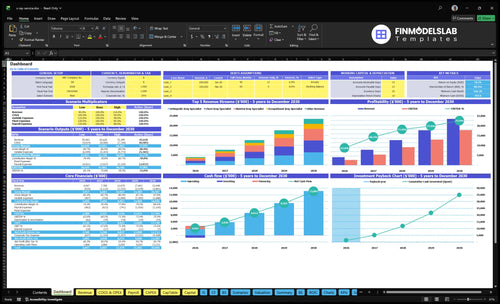
See X-Ray Imaging Service Financial Model Template for revenue, EBITDA, cash, payback, and owner income. The chart stress-tests revenue from $4,067M to $23,448M and EBITDA from $2,588M to $17,794M; open the model.
Owner-income model highlights
- Owner take-home output
- Revenue and EBITDA view
- Scenario tests by inputs
What profit margin does an x-ray imaging service make?
An X-Ray Imaging Service can make a strong margin if it keeps chairs full: with year 1 variable costs at 25% of revenue, the implied gross margin before fixed overhead is about 75%. On the provided numbers, EBITDA is $2.588 million on $4.067 million of revenue, or 63.6%, and year 5 is $17.794 million on $23.448 million, or 75.9%. For operating cost detail, see What Are Operating Costs For X-Ray Imaging Service?
Year 1 margin math
- 12% teleradiology interpretation
- 3% consumables
- 6% physician outreach
- 4% billing and collections
What moves owner take-home
- Utilization lifts margin fast
- Fixed cost spread matters most
- Payroll growth can compress EBITDA
- Reimbursement assumptions change cash
How many x-ray exams per day are needed to pay the owner?
For X-Ray Imaging Service, the owner gets paid only after the clinic clears break-even: about 545 paid exams per month at a $138 average collection, 25% variable costs, and $56,000 in monthly fixed payroll plus overhead. The daily target is simple: 545 ÷ actual operating days. Year 1 volume is about 2,458 paid exams per month and 29,496 per year, so the cushion for owner salary starts after fees, billing, marketing, and reserves are covered.
Break-even math
- 545 paid exams monthly at break-even
- $138 average collection per exam
- 25% variable costs
- $56,000 fixed payroll plus overhead
Owner pay trigger
- Divide monthly exams by operating days
- Use collected exams, not bookings
- Year 1 runs at 2,458 exams monthly
- Owner pay starts after all fixed costs
Does payer mix affect x-ray imaging service owner income?
Yes—payer mix can move owner income a lot for an X-Ray Imaging Service because the modeled source rates are service prices, not reimbursement guarantees. Year 1 average collection is about $138 per paid exam across chest, skeletal, pediatric, orthopedic, and occupational exams, but commercial insurance, Medicare, Medicaid, self-pay, employer contracts, and referral sources can change both collection levels and cash timing.
Income drivers
- Commercial often pays more.
- Medicaid can pull averages down.
- Self-pay changes cash timing.
- Employer contracts may trade price for volume.
Cash and break-even
- Lower collections raise break-even volume.
- Cash pay can ease working capital stress.
- Employer contracts can speed cash receipt.
- Lower price can still protect access.
Want to see the main X-ray income drivers?
1
2,458/moPaid Volume
More paid exams drive the biggest lift in Year 1 revenue, which is $4.067M.
2
$138Net Collections
A higher average collected amount per exam raises cash without adding more visits.
3
12%Teleradiology Fee
This direct read-cost cut comes off each exam, so lower fee pressure improves EBITDA fast.
4
$23K/moFacility Overhead
Fixed clinic overhead stays in place each month, so more volume is needed to spread it.
5
$85KTech Staffing
Lead technologist pay sets a core labor floor, and extra FTEs can squeeze take-home if volume lags.
6
55%-85%Referral Use
Better referral flow keeps capacity filled and protects revenue as the clinic scales.
X-Ray Imaging Service Core Six Income Drivers
Paid Exam Volume
Paid Exam Volume
Paid exam volume is the count of completed X-ray exams that turn into collected revenue. Here’s the quick math: volume rises from 2,458 paid exams per month in Year 1 to 12,292 in Year 5, about 5x. That spread helps cover rent, software, insurance, and payroll. But if denials, no-shows, or empty rooms stay high, owner pay stays thin even when prices look strong.
Raise Collected Exams
Track completed exams, denied claims, no-shows, and room utilization every week. Capacity in the model improves from 40% to 55% in several early services, then 70% to 85% by Year 5, so the real job is turning booked slots into collected exams. Tight scheduling, reminder calls, and cleaner payer work lift cash flow and make owner draws less fragile.
1
Payer Mix And Net Collections
Payer Mix And Net Collections
Net collections is the cash you actually keep per paid exam after payer discounts, denials, and slow pay. In this model, Year 1 pricing implies about $138 per paid exam, and Year 5 implies about $159. Here’s the quick math: at 2,458 monthly paid exams, every $1 move in average collected revenue shifts monthly revenue by about $2,458.
The mix matters because chest exams start at $120, skeletal at $150, pediatric at $180, orthopedic at $160, and occupational at $100. More low-price exams pull the average down, and slower insurance cash can force a bigger reserve even when the profit report looks fine, which can squeeze owner pay.
Track Collections by Exam Type
Measure collected revenue per paid exam by exam type and payer, then compare it to the $138 Year 1 and $159 Year 5 targets. Watch denial rate, days in receivables, and the share of $100 to $120 exams, because that mix drags the average down fastest.
Use clean claims, fast follow-up, and payer-by-payer reporting so cash comes in on time. If collections lag, hold more cash before taking draws, since delayed insurance money can raise working capital needs even when monthly profit is positive.
2
Radiologist Interpretation Cost
Radiologist Read Cost
Radiologist interpretation fee is the read cost per exam, usually modeled as a % of collected revenue. Here it starts at 120% in Year 1 and declines to 100% by Year 5, so read cost alone can erase margin before technologist pay, rent, and marketing. On $4.067M Year 1 revenue, each 1 percentage point change shifts annual profit by about $41k.
That pushes break-even exam volume up when fees rise and cuts owner distributions when collections don’t keep pace. Lower read rates help only if report turnaround and referral expectations still support exam volume; cheap reads that slow reports can hurt income more than they save.
Control Read Cost Without Losing Volume
Track read fee as % of collections, turnaround hours, and volume by referral source. The key test is simple: if a lower rate saves cash but delays reports, owner income can fall even with a better unit cost. The model’s move from 120% to 100% is a 20-point swing, or about $820k a year on $4.067M revenue.
Use written service levels, volume floors, and rate reviews tied to actual exam counts. One line to remember: fast reads protect volume; cheap reads protect margin.
3
Technologist Staffing Cost
Technologist Staffing Cost
Technologist staffing sets how many rooms you can keep open and how many exams you can finish on time. In the model, a lead radiologic technologist runs at $85k a year with 10 FTE in Years 1 to 3, then $170k with 20 FTE in Years 4 to 5. Total payroll rises from about $400k to $850k, so owner pay only works if exam volume grows with staffing.
Owner labor can lower early cash burn, but it is not durable compensation. If staffing grows faster than paid exams, margin drops fast and distributions stall, even when the schedule looks full.
Keep labor tied to paid exams
Measure FTEs, overtime hours, exams per shift, and no-show coverage each month. Use those inputs to forecast payroll before you add hours or open days.
- Track paid exams per FTE.
- Separate owner labor from salary.
- Flag overtime above plan.
- Hire only for filled rooms.
If owner time is doing the work in Year 1, model it as a cost, not free labor. That keeps break-even honest and protects take-home pay later.
4
Equipment And Facility Costs
Fixed facility burn
$23k in monthly overhead — rent, software, maintenance, utilities, insurance, and admin — hits before the first exam is collected. That means owner income depends on how fast exam volume covers a fixed base of $276k a year, before debt service or any draw. No volume, no margin cushion.
Startup cash also matters because the model needs $360k for two digital X-ray units, $250k for buildout and shielding, $45k for server infrastructure, plus other launch assets. The disclosed $748k minimum cash need in Month 2 shows how quickly facility spend can trap cash, even if pricing looks strong.
Protect cash before pay
Build the model around the month, not the year. Track rent, licenses, maintenance, utilities, insurance, admin, debt service, and replacement reserves separately so distributions start only after those claims are covered. If you pay out too early, owner income gets hit by a later cash squeeze. That’s the real risk.
Use a simple gate: projected cash, not booked profit, must stay above the $748k Month 2 need plus any debt payment. Then test how many exams per month are needed to absorb the $23k fixed burn. Faster utilization helps, but underused rooms make this cost base hard to carry.
5
Referral Pipeline Utilization
Referral Pipeline Utilization
This driver is how referrals turn equipment time into paid exams. Track referral volume, conversion rate, occupational exam volume, and scheduling speed; stronger provider access and employer accounts raise throughput. In this model, physician outreach and marketing run at 60% of revenue in Year 1, then ease to 40% by Year 5, so the pipeline has to do more of the work early.
Occupational exams add 360 monthly paid exams in Year 1 and 1,800 in Year 5. If referrals stall, rooms stay open but underfilled, and fixed costs like rent and payroll still hit the owner’s take-home. The quick math is simple: more converted referrals mean more collected exams, better margin spread, and more cash left for owner pay.
Measure and tighten referral flow
Watch the full funnel: referrals received, appointments booked, show rate, and paid exams. Also track turnaround time for reports, because fast delivery helps keep provider trust and repeat volume. If conversion drops, high fixed costs get stranded fast.
- Speed up booking and same-day slots.
- Grow employer and provider accounts.
- Review lost referrals by source.
- Test outreach spend against paid exams.
Use the Year 1 marketing budget at 60% of revenue to build the funnel, then expect better efficiency as it falls toward 40% by Year 5. That only works if each outreach dollar produces more completed exams, not just more calls and emails. The owner earns more when referral conversion rises faster than support costs.
6
Compare lean, base, and high X-ray owner income scenarios
Owner income scenario table
Owner income moves with exam volume, pricing, and how well fixed clinic costs get spread. The low, base, and high cases show how much cash can reach the owner after reserves.
| Scenario | Low CaseVolume risk | Base CasePayer risk | High CaseFixed-cost leverage |
|---|---|---|---|
| Launch model | Low Case keeps earnings near Year 1 output, with 2,458 monthly paid exams, $4.067 million revenue, and $2.588 million EBITDA. | Base Case reflects Year 3 scale, with 7,100 monthly paid exams, $12.670 million revenue, and $9.116 million EBITDA. | High Case reflects Year 5 scale, with 12,292 monthly paid exams, $23.448 million revenue, and $17.794 million EBITDA. |
| Typical setup | The clinic runs with one-site volume, lower utilization, and enough fixed cost to leave the owner with salary plus only small distributions. | The clinic is running at steady utilization, the core service mix is established, and owner pay comes from salary plus regular distributions after reserves. | The clinic reaches fuller capacity, spreads rent and software across more exams, and has room for larger owner distributions. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $110k salary onlyIncome floor | $110k plus distributionsCore case | $110k plus larger distributionsUpside case |
| Best fit | Use this to stress-test a slow start, weak referral flow, or a payer mix that delays cash. | Use this as the most likely plan if referrals stay steady and the clinic keeps its Year 3 pace. | Use this to test upside if demand stays strong and fixed costs get absorbed by more exams. |
Planning note: These ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- X-Ray Imaging Service Porter's Five Forces Analysis
- X-Ray Imaging Service BCG Matrix
- X-Ray Imaging Service Business Model Canvas
- What Are The 5 KPIs For X-Ray Imaging Service?
- X-Ray Imaging Service Business Plan Template in Pre-Written Word
- How Increase X-Ray Imaging Service Profits?
- What Are Operating Costs For X-Ray Imaging Service?
- How Much It Costs To Start An X-Ray Imaging Service: $748K Cash Need
- X-Ray Imaging Service Financial Model Template in Excel
- How To Open An X-Ray Imaging Service In 6 To 12 Months
- How To Write X-Ray Imaging Service Business Plan?
- X-Ray Imaging Service Marketing Mix
- X-Ray Imaging Service Marketing Plan
- X-Ray Imaging Service Business Proposal
- X-Ray Imaging Service PESTEL Analysis
- X-Ray Imaging Service Pitch Deck Example Editable PPTX
- X-Ray Imaging Service Business SWOT Analysis
- X-Ray Imaging Service Value Proposition Canvas
Frequently Asked Questions
The model shows a minimum cash need of $748k, with the lowest point in Month 2 That cash sits on top of major capex, including $360k for two digital X-ray units and $250k for buildout and shielding Keep reserves separate from owner pay because early claims timing, equipment payments, and staffing can absorb cash fast