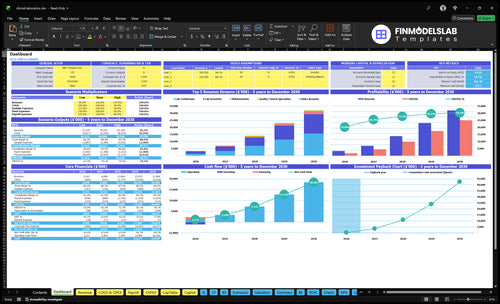
You’re not buying a fixed salary here you’re building cash flow from collected tests This five-year estimate separates $335M first-year revenue, 86% gross margin, payroll, fixed overhead, Clinical Laboratory Improvement Amendments (CLIA) compliance, reserves, owner salary, and distributions, but it is not tax advice
Owner income$1.74MNet margin73.7%Revenue for target pay$2.36MBusiness difficultyHard
Want to test your clinical lab owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: This is a researched planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Clinical Laboratory profit margin depends on whether you mean gross margin, operating margin, or owner income. In Year 1, the model points to 86% gross margin before fixed costs, while variable costs include 10% reagents and consumables, 4% sample collection and logistics, and about 5% more from commissions, referral fees, and usage-based software; see How Much Does It Cost To Open A Clinical Laboratory Business? for the setup side. Gross margin moves with reimbursement per test, reagent pricing, and the mix of routine chemistry, hematology, immunoassay, molecular, and serology.
Gross margin drivers
86% Year 1 gross margin baseline
10% reagents and consumables
4% sample collection and logistics
5% commissions, referrals, software
Operating margin pressure
Lab labor lowers operating margin
Analyzer leases add fixed cost
Quality control and denial rates hurt cash
Send-out testing can compress profit fast
How much does a clinical lab owner take home after expenses?
A Clinical Laboratory owner’s take-home starts with collected revenue, not gross charges; in this first-year model, $3.35M from 4,545 monthly tests leaves about $2.17M before reserves and owner-level items. Here’s the quick math: $3.35M × 81% after 14% COGS and 5% variable costs, minus $273.6k fixed overhead and $270k visible payroll; for market context, see What Is The Current Growth Trend Of The Clinical Laboratory Business?.
Model math
$3.35M collected annual revenue
4,545 tests per month
14% cost of goods sold
5% variable operating costs
Owner cash
$2.17M pre-reserve operating cash flow
Subtract debt and equipment financing
Reserve cash for working capital
Deduct owner pay, taxes, missing wages
Is a clinical laboratory profitable?
Clinical Laboratory can be highly profitable, but only if volume, reimbursement, collections, staffing, compliance, and equipment use stay tight. Under the stated assumptions, revenue rises from $335M in Year 1 to $3,198M in Year 5, so the model scales fast, but weak payor contracts or claim denials can break the math. If onboarding drags, analyzers sit idle, or qualified staff are short, profit gets squeezed fast.
What drives profit
Volume has to keep rising.
Collections must stay clean.
Reimbursement needs strong contracts.
Equipment use must stay high.
Main risks to watch
Claim denials cut cash fast.
Credentialing delays slow billing.
Staff shortages raise operating risk.
CLIA issues can stop operations.
Clinical Laboratory Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Want the six clinical lab income drivers?
1
Test Volume
4.5K/mo
More monthly tests spread fixed lab costs over more revenue, so take-home rises fast once capacity stays full.
2
Payor Mix
$6.1K/test
Better payer reimbursement lifts revenue per test, and even small rate gains flow straight into owner income.
3
Test Mix
$45-$200
Shifting work toward higher-priced panels and molecular tests raises gross profit without needing the same jump in headcount.
4
Test Cost
14%
Reagents, consumables, and logistics drive direct cost, so keeping them near 14% protects the 86% gross margin.
5
Overhead
$228K/mo
Rent, compliance, and payroll set the monthly cash burn, so lower overhead means faster profit and less funding pressure.
6
Collections
11 mo
Faster billing and cleaner collections improve cash timing, which matters when minimum cash lands in Month 3.
Clinical Laboratory Core Six Income Drivers
Test Volume and Capacity Utilization
Test Volume and Utilization
Test volume is the number of completed lab tests billed each month, and it only lifts owner income when staffing, quality control, and turnaround time hold. In this model, volume rises from 4,545 monthly tests in Year 1 to 37,479 in Year 5, about 8.3x growth. That matters because more accessions can spread fixed overhead over more tests.
Here’s the catch: higher volume helps only if reimbursement is real and collections come in. If pathologist capacity moves from 50% to 75% and lab scientist capacity from 65% to 85%, the lab can absorb more work. But weak payor mix, denials, or slow cash can still wipe out profit and owner draw.
Track Capacity by Role
Measure tests per month, accession backlog, turnaround time, QC failure rate, and labor hours by role. Accessions means accepted specimens, so count every sample that makes it into production. If volume rises but turnaround slips, the lab can lose client trust and create rework, overtime, and cash pressure.
Use the Year 1 to Year 5 ramp as your staffing test: compare actual output with 4,545 to 37,479 monthly tests and check whether capacity stays inside target. Keep an eye on collections too, because more tests do not help owner income if reimbursement is weak or cash comes in late.
1
Payor Mix and Reimbursement
Payor Mix and Reimbursement
Collected revenue per accession is the cash a lab keeps for each completed test. With $278,875 in monthly revenue and 4,545 monthly tests, Year 1 collected revenue is about $61.36 per test. Medicare, commercial insurance, patient-pay, contracted accounts, and denied claims all change how much of that shows up as owner income.
This driver is about more than price. If medical necessity, credentialing, documentation, or claim timing slips, the lab can run tests and still wait on cash. That hurts payroll coverage, vendor payments, and owner draw. One clean claim beats a fast test with a slow or denied payment.
Track reimbursement by payer
Measure collected revenue per accession, denial rate, days in accounts receivable, and cash collected by payer type. Split Medicare, commercial, patient-pay, and contracted accounts so you can see which mix supports margin and which one only adds billing work. Use the same view for new contracts before you promise volume.
Test owner pay against cash, not billed charges. Tighten documentation, confirm credentialing before testing starts, and review denials weekly. If reimbursement drops or collections slow, revenue can still look fine on paper while actual take-home falls. Here’s the quick math: $278,875 ÷ 4,545 = $61.36 per test.
$61.36 collected per test
4,545 monthly tests
$278,875 monthly revenue
Track denials and cash timing
2
Test Menu Mix
Test Menu Mix
Your test menu mix drives both revenue and gross margin. In Year 1, prices range from $30 hematology tests to $180 infectious disease molecular tests, with $120 specialized immunoassay and $45 routine chemistry. The same test count can produce very different owner income depending on payer reimbursement, send-outs, labor, and quality control.
Higher price does not always mean higher profit. A complex assay can need more validation, equipment time, and compliance work, so its real margin can be lower than a cheaper, high-volume test. Revenue mix matters because it changes cash flow, fixed-cost absorption, and the amount left for owner pay.
Track Margin by Test Type
Measure tests by type, collected price per test, direct cost per test, and send-out rate. Compare hematology, chemistry, immunoassay, and molecular work on net margin, not just billed revenue. A $180 test that needs heavy QC can return less cash than a $45 in-house assay.
Track volume by test code.
Price against true cost.
Watch payer reimbursement.
Cut low-yield send-outs.
To improve owner income, push volume toward the assays with the best margin after labor, controls, and reimbursement. If a new menu item cannot cover validation and workflow time, it can lift top line but still reduce profit and delay owner draw.
3
Direct Testing Cost Control
Direct Testing Cost per Test
Direct testing cost sets gross margin before overhead. In Year 1, direct COGS is 14% of revenue, made up of 10% reagents and consumables plus 4% sample collection and logistics. By Year 5, that drops to 11%, so every clean point of savings stays in the lab and supports owner pay. Gross margin is still not net income, because payroll, rent, compliance, equipment, billing, reserves, and owner draw come later.
Here’s the quick math: lower per-test cost raises the share left after lab work is done. If reagent waste, reruns, send-outs, or direct lab labor drift up, margin shrinks fast even when volume grows. The key inputs are test mix, specimen volume, reagent use, logistics, and direct labor tied to each run.
Track Cost per Test by Assay
Measure COGS per test by test type, not just in total. Split the cost into reagents, consumables, specimen supplies, send-outs, and direct lab labor, then compare each assay against its collected price. Watch re-runs, controls, calibrators, and courier waste closely, because those small misses eat owner income before overhead even shows up.
Set a weekly review on the tests with the most spend. If volume rises but cost per test also rises, the business can look busy and still pay less. A tight target is moving from 14% direct COGS toward 11% over time, while keeping turnaround time and quality stable.
4
Staffing and Compliance Overhead
Staffing and Compliance Overhead
This driver is the cash cost of keeping the lab staffed and compliant. In Year 1, visible payroll already includes a $180k Lab Director and a $90k Senior Lab Scientist, while fixed overhead adds $228k/month. Owner pay gets squeezed fast unless test volume covers qualified labor, medical director oversight, quality systems, and required compliance work.
What this estimate hides is that CLIA compliance and accreditation fees are only $1k/month. The bigger risk is under-staffing or delaying training, proficiency testing, or admin work; that can slow turnaround, hurt collections, and force the owner to keep cash in the business instead of taking profit out.
Track loaded labor per test
Measure total staffing and compliance cost per accession, not just wages. Divide director pay, scientist pay, and overhead by monthly test volume, then compare it to collected revenue per test. If volume rises but labor per test stays flat or climbs, owner income is still getting squeezed.
Build the schedule around required coverage for quality control, proficiency testing, training, and compliance admin. The clean test is simple: if a role or fee is mandatory to stay accredited, price and forecast it before you add more volume.
5
Billing Collections Performance
Billing Collections
Billing collections is the cash that comes in after coding, documentation, credentialing, denials, and patient balances are cleared. At $278,875 monthly revenue across 4,545 tests, collected revenue is about $61 per test; even with $335M Year 1 revenue, slow collections can still crush owner pay.
Track cash, not claims
Measure DSO, denial rate, credentialing lag, and patient collection rate by payer. Watch billed revenue and collected revenue side by side, because a healthy test count can still produce weak cash if claims sit unpaid. If collections can’t cover fixed overhead, direct costs, and owner pay, growth is just more receivables.
Review aged AR every week.
Fix missing docs before filing.
Chase denials within 48 hours.
Hold cash for payroll first.
Separate patient balances fast.
6
Clinical Laboratory Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Compare lean, base, and high clinical lab income scenarios
Owner income scenarios
Owner income changes fast in this lab because test volume, pricing, staffing, and fixed overhead move together. The low, base, and high cases show how much cash can stay in the business under different workload levels.
Lean, base, and high cases show how test volume and staffing change owner cash.
Scenario
Low CaseLean Case
Base CaseBase Case
High CaseHigh Case
Launch model
This is the lower earnings path with tighter volume and thinner cash left after payroll and lab overhead.
This is the modeled middle path with steadier volume and stronger cash generation.
This is the stronger earnings path with higher throughput and the most cash left before reserves.
Typical setup
The lab runs about 4,545 monthly tests, with roughly $335M revenue, 86% gross margin, and about $217M pre-reserve operating cash flow using visible payroll only.
The lab runs about 16,633 monthly tests, with roughly $1,389M revenue, 875% gross margin, and about $1,088M pre-reserve operating cash flow using visible payroll only.
The lab runs about 37,479 monthly tests, with roughly $3,198M revenue, 89% gross margin, and about $2,646M pre-reserve operating cash flow using visible payroll only.
Cost drivers
Lower test volume
early staffing
reagents and consumables
sample logistics
fixed lab overhead
Mid-range test volume
balanced price mix
staffing growth
reagent spend
compliance and support costs
Higher test volume
better price mix
more capacity use
stronger referral flow
scaling payroll
Owner income rangeBefore owner reserves
$200M - $230MIncome floor
$1.05B - $1.12BPlanning middle
$2.60B - $2.70BUpside case
Best fit
Use this to stress-test a slower launch or weaker payer mix.
Use this as the main planning case for budgeting and lender discussions.
Use this to test upside from faster volume growth and better lab utilization.
!
Planning note: These scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Reserve needs depend on billing lag, payroll size, supplies, and debt service The model shows $228k monthly fixed overhead before payroll, plus $270k visible annual payroll in Year 1 Since no reserve percentage is supplied, do not treat the $217M pre-reserve cash flow as fully distributable owner income
Break-even depends on collected revenue, not launch age In the first-year case, fixed overhead is $228k/month and visible payroll is $225k/month, so the lab needs enough gross profit to cover about $453k monthly before owner pay At an 81% contribution after direct and variable costs, the modeled break-even revenue is far below first-year revenue
Yes, the model includes a Lab Director at $180k per year from launch It also includes a Senior Lab Scientist at $90k per year and CLIA compliance and accreditation fees at $1k per month These costs protect quality, oversight, and compliance, so they should sit above owner distributions in the cash plan
Collections, reimbursement per test, staffing, and direct testing cost move distributions the most Year 1 uses 4,545 monthly tests, $6136 average collected revenue per test, 14% direct COGS, and 5% variable costs If claim denials rise or payor mix weakens, owner distributions can fall even when test volume looks healthy
The best role depends on whether the owner can manage operations without weakening compliance or sales An owner-operated lab may save leadership cost but adds execution risk A manager-run lab needs stronger payroll coverage, especially as staffing rises from 3 lab scientists in Year 1 to 15 in Year 5
About the author
Gregory Ford
Launch Planning Specialist
Gregory Ford is a launch planning specialist at Financial Models Lab who helps first-time entrepreneurs judge whether a business idea is financially realistic. He focuses on operating cost estimates and turns broad business questions into clear planning assumptions and practical next steps. Gregory writes about opening and running small businesses in a straightforward, easy-to-understand way.
Choosing a selection results in a full page refresh.