How To Open A Clinical Laboratory: 6 Gates To First Tests
You’re opening a regulated testing operation, not just renting lab space This launch plan covers Clinical Laboratory Improvement Amendments (CLIA) planning, facility setup, equipment, staffing, validation, specimen intake, referral readiness, and a 60-month model check for timing, hiring, revenue ramp, and cash runway
Time to Open6-12+ monthsSetup windowLaunch Sequence7 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepSigned clientClaims ready
Launch timeline
This short web timeline shows the main launch workstreams, and the XLSX export holds the detailed task-level Gantt chart.
Why test the Clinical Laboratory launch plan before opening?
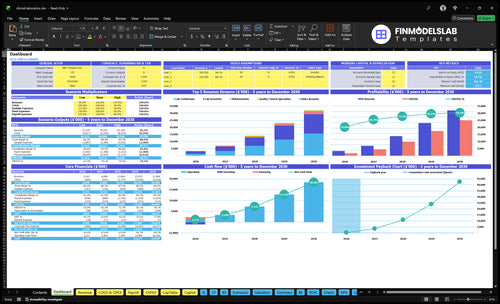
Before opening, the Clinical Laboratory Financial Model Template shows dashboard and model tabs for launch timing, revenue, staffing, runway, and break-even. Year 1 prices are $45 routine chemistry, $30 hematology, $120 specialized immunoassay, $180 infectious disease molecular, and $70 serology. The charts tie specimen volume, staffing, payer collections, equipment commitments, and runway. Open it.
Financial model highlights
Monthly overhead: $22,800
Variable costs: 19%
Scientists 65%; pathologists 50%
Phlebotomists 70%; techs 60%
Quality control 75%
Do I need CLIA to open a clinical lab?
Yes—if your Clinical Laboratory tests human specimens to diagnose, prevent, or treat disease, you need the right CLIA certificate before patient testing; see What Is The Current Growth Trend Of The Clinical Laboratory Business? for the market backdrop. CLIA means Clinical Laboratory Improvement Amendments, and the Centers for Medicare & Medicaid Services program covers 320,000+ US lab entities.
CLIA trigger
Test human samples for clinical use
Match certificate to test complexity
Cover waived, moderate, or high complexity
No patient testing before approval
Launch order
Set the test menu first
Confirm state licensing and accreditation
Verify director and staff credentials
Finish SOPs, validation, and reporting controls
How long does it take to open a clinical lab?
Clinical Laboratory openings usually take 6–12+ months in practice, and the clock depends on facility readiness, CLIA and state processing, lab director approval, equipment delivery, LIS implementation, validation studies, SOP completion, vendor setup, hiring, and training. Here’s the quick math: validation only closes cleanly when equipment, methods, personnel, QC procedures, and reporting workflows are ready, so go-live slips fast if the 9-person Year 1 team is not hired or scheduled early.
Main timing drivers
6–12+ months is the practical range
CLIA and state review take time
Equipment and LIS must arrive first
Validation waits on ready workflows
Go-live risk points
3 lab scientists must be scheduled
2 phlebotomists need training early
2 lab technicians support daily testing
1 QC specialist and 1 pathologist matter before launch
What clinical lab launch mistakes create the biggest risk?
The biggest launch risk in a Clinical Laboratory is opening before the basics are approved: accepting specimens too early, incomplete validation, weak QC logs, no lab director coverage, and untested LIS reporting. With 19% Year 1 variable costs and $22,800 in monthly fixed overhead before payroll, weak volume or billing delays can drain cash fast, so first accounts and payer setup need to be live before go-live.
Big launch traps
Don’t accept specimens before approval.
Finish the validation file first.
Keep QC logs complete and ready.
Cover lab director oversight on day one.
Go-live checks
Sign SOPs and calibrate equipment.
Train staff and test specimen labels.
Run courier flow and billing setup.
Lock referral commitments and first accounts.
Clinical Laboratory Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Verify clinical lab readiness before accepting specimens
Launch readiness checklist
Use this go-live approval checklist to confirm the clinical laboratory is ready before opening.
1Regulatory
CLIA scope filedCritical
No test should start until the CLIA scope matches the menu.
State lab license approvedCritical
State approval is a hard stop where a lab license is required.
Lab director appointedCritical
A named director is needed for oversight and signoff before launch.
2Facility
Power and storage readyHigh
Freezers, backup power, and utilities must support sample holding.
Analyzers installedCritical
Core analyzers must be installed before any patient sample runs.
Calibration records completeCritical
Missing calibration records can block release of first results.
3Validation
Methods validatedCritical
Validated methods are required before patient reporting starts.
QC records documentedCritical
Daily quality control proves the lab can hold result quality.
Result review workflow setHigh
A clear review path prevents unapproved or delayed reports.
4Staffing
Year 1 roster filledCritical
Launch staffing must cover Year 1 roles without open shifts.
Staff trained on SOPsCritical
Staff need the standard operating procedures before first specimens.
Coverage schedule postedHigh
Unstaffed hours raise turnaround risk and can stop intake.
5Specimens
Collection process testedCritical
Collection errors create bad samples and wasted capacity.
Accessioning process worksCritical
Accessioning must track every sample from intake to result.
Waste disposal arrangedHigh
Medical waste pickup must be in place before live sample work.
6Revenue
Billing setup approvedCritical
Billing must work before launch or cash collection will lag.
First referral channel setCritical
No first-volume channel means the lab opens without demand.
Cash runway reviewedCritical
The model shows a Month 3 cash low, so runway needs a hard check.
Want to see the six clinical lab launch drivers?
1Regulatory Approvals
6-12+ mo
Approval is the legal gate, and delays can stretch opening into a 6-12+ month window.
2Facility Setup
$22.8K/mo
Working space, analyzers, and the lab information system must be live before controlled sample runs.
3Test Validation
5 tests
A validated five-test start limits errors and speeds the first controlled patient reports.
4Qualified Staff
9 staff
Nine year-one staff members cover collection, testing, QC, and review without overextending shifts.
5Specimen Workflow
19% var
Clean intake, logistics, and vendors keep specimens moving and hold variable costs near 19%.
6Revenue Readiness
$30-$180
Signed providers, employers, and billing flows turn $30-$180 tests into opening revenue.
Regulatory Approvals
Approval Gate
This is the first gate before you can test patient samples. Opening on time depends on the right CLIA certificate, any required state license, a qualified lab director, complete personnel files, and written policies that match the test complexity you plan to run. If your planned menu exceeds the approved scope, go-live stops.
That also means validated methods have to line up with the approval scope. If the package is incomplete or mismatched, the launch usually shifts from full opening to a narrower, controlled specimen intake while you wait on approval.
Lock Scope Before Filing
Start with the exact test menu, then match it to the certificate type and permitted complexity. Build the compliance file set at the same time: leadership assignment, SOPs, personnel records, and validation plans. One line matters here: no approval, no specimen intake.
Define launch tests first.
Match scope to certificate.
File SOPs and staffing.
Hold intake until approval.
If the filing is weak, the bottleneck is usually a processing delay or a scope mismatch, not the lab floor. That can push back validation, delay first revenue, and leave staff ready before the lab is legally allowed to run the planned tests.
1
Facility, Equipment, And Systems
Lab Space, Equipment, and Systems
This driver decides whether the lab can receive, process, store, test, and report samples on day one. The readiness signal is simple: completed space, utilities, analyzers, benches, refrigeration, sample storage, LIS (laboratory information system) workflows, maintenance coverage, and a working reporting process.
If buildout slips or an analyzer arrives late, validation stops too. That can push opening, delay first revenue, and force staff to wait on idle equipment. Delayed delivery, failed interface testing, or no maintenance coverage are the main launch risks because they break the chain from specimen intake to result delivery.
Build, Install, and Test the Workflow
Plan the site as one connected system, not separate parts. Verify utilities, install equipment, calibrate analyzers, set up refrigeration and storage, then configure the LIS so orders route, results post, and downtime steps are clear. Validation needs working equipment and systems, so this sequence has to be finished before controlled test runs.
Confirm room, power, and utility readiness.
Track analyzer and bench delivery dates.
Test LIS routing before go-live.
Document downtime and repair contacts.
Assign maintenance coverage before opening.
What this setup hides: every missed handoff adds risk. If result routing fails or a critical unit has no service plan, the lab may open with partial capacity, slower turnaround, and more manual work. That raises staffing pressure, cash burn, and customer frustration right when reliability matters most.
2
Test Menu, Validation, And Quality Control
Test Menu, Validation, And QC
This driver sets what the lab can safely report on day one. A feasible initial test menu, completed method validation, signed SOPs, QC rules, and reference ranges where needed are what keep opening from slipping. If the menu is too wide before staff and systems are ready, validation drags out and patient reporting gets delayed.
Here’s the quick math: Year 1 price anchors are $30 hematology, $45 chemistry, $70 serology, $120 immunoassay, and $180 molecular. A narrow launch menu cuts risk and lets the team prove consistent performance before live reporting starts. One clean rule: no validation, no release.
Launch Menu and QC Checklist
Before opening, lock the first test list, document each validation, and train staff on result review. Set QC frequency in writing, then rehearse the full path from specimen receipt to final sign-out so the team can catch failures before patients are involved.
Pick only launch-ready tests.
Finish validation before go-live.
Sign SOPs and QC rules.
Train staff on review steps.
Use reference ranges where needed.
What this hides is timing risk: every extra assay adds validation work, QC checks, and training time. If the lab opens with a broad menu, first-day service can slow down, staff can miss review steps, and early results can be held back while the team fixes gaps.
3
Qualified Staffing
Qualified Staffing
Opening depends on whether the lab has enough trained coverage to receive, process, review, and release results on day one. The readiness signal is a lab director in place, staff trained on specimen flow, QA ownership assigned, and schedules matched to expected volume. If opening hours run past trained coverage, the lab can open late, move slower, or delay reporting.
Year 1 staffing assumes 3 lab scientists, 2 phlebotomists, 2 lab technicians, 1 QC specialist, and 1 pathologist. Capacity starts at 65% for lab scientists, 70% for phlebotomists, 60% for technicians, 75% for QC, and 50% for pathologists, so the launch plan has to stay inside that coverage band or first-day service gets strained.
Staff to Coverage
Map every opening hour to a named person before go-live. The launch check is simple: who covers specimen intake, processing, QC review, and final sign-off when volume peaks? If one role is thin, shorten hours first, then scale them after training and schedules hold steady.
Confirm lab director assignment.
Document QA ownership.
Match schedules to expected volume.
Train specimen processing coverage.
Test handoffs before first patient samples.
This keeps day-one work inside the team’s real capacity, which lowers reporting delays and cuts the chance of a rushed opening. If the lab cannot cover all shifts with trained people, the safer move is a narrower launch window, not a fuller schedule.
4
Specimen Workflow And Vendors
Specimen Flow and Vendor Setup
Opening day depends on moving the first specimen from collection to a reported result without a break. If collection, labeling, transport, accessioning, storage, and turnaround-time steps are not wired together, even a licensed lab can stall at intake. The Year 1 model also assumes 10% for reagents and consumables and 4% for sample collection and logistics, so weak vendor control turns straight into missed runs and higher cash needs.
This workflow also covers vendor accounts, courier setup, supply par levels, specimen rejection rules, chain-of-custody where needed, waste disposal, reference lab relationships, and escalation steps. One clean handoff matters. Lost samples, stockouts, or unclear ownership can slow onboarding and force rework before the first billable result is ready.
Lock the Handoff Chain
Before opening, verify every handoff on one live specimen path: collection kit, label, pickup, receipt, accessioning, storage, and result release. Then test the exception path too: rejected specimen, late courier, short inventory, and after-hours escalation. If any step lacks an owner, the launch plan is too loose for day one.
Set par levels before go-live.
Open courier and vendor accounts early.
Write rejection rules and chain-of-custody.
Assign backup contacts for delays.
Track turnaround time from specimen receipt.
What this estimate hides: a small supply gap can block reporting even when staff and equipment are ready. Clean vendor setup reduces failed runs and makes customer onboarding smoother, because practices get faster, clearer feedback on every specimen.
5
Referral, Payer, And Revenue Readiness
Referral, Payer, And Revenue Readiness
No signed channel, no first specimen volume. This driver decides whether the lab opens with real orders or sits on ready staff and idle equipment. You need signed provider relationships, employer accounts, direct-pay flow, billing workflow, and payer enrollment where it applies before day one revenue can start.
At a $30 to $180 price range per test, even small delays in referral setup push back cash flow fast. The launch risk is not just sales; it is whether the lab can confirm pricing, route claims or cash-pay orders, and deliver results cleanly enough to keep the first accounts active.
Map the money path before the first draw
Set the account path first. Define the test menu by customer need, confirm pricing, and write the onboarding script before outreach starts. Then test result delivery, billing steps, and claim or cash-pay handling with one pilot account so the team knows what happens from order to payment.
Secure opening-month volume targets.
Check payer enrollment timing where needed.
Review referral payments for compliance.
Keep referral and sales costs near 3%.
Watch the cash gap. If claims are not ready, revenue slows even when specimens arrive. If referral scripts are weak, the practice may order once and stop. The goal is simple: first volume, first clean bill, and no delay between collection, report delivery, and collections.
Yes, ownership and medical oversight are different issues A non-physician may own a lab, but the operation still needs qualified leadership, including a lab director that fits the CLIA scope and state rules Plan around Year 1 staffing of 3 lab scientists, 2 phlebotomists, 2 lab technicians, 1 QC specialist, and 1 pathologist
Plan for 6–12+ months before accepting patient samples The timeline depends on CLIA and state approvals, facility readiness, equipment installation, LIS setup, validation, SOPs, and staff training If validation or lab director approval slips, the opening date usually slips too, even if rent and payroll have already started
Maybe, depending on test complexity, payer needs, state rules, and customer expectations CLIA is the core federal requirement for most human diagnostic testing, but accreditation can be part of market access or compliance strategy Treat it as a launch gate if referral partners, payers, or your chosen test menu require it
The common delays are approval timing, incomplete validation, equipment delivery, LIS interface problems, missing SOPs, and unfilled qualified roles The model assumes fixed overhead of $22,800 per month before payroll, so every delay matters Build the opening plan around dependencies, not just a target go-live date
Secure committed specimen sources before opening Start with physician practices, clinics, urgent care centers, employer testing accounts, direct-pay testing, or payer-ready claims Use the first test menu to sell clearly: Year 1 pricing assumptions range from $30 for hematology to $180 for infectious disease molecular testing
About the author
George Lawson
Small Business Advisor
George Lawson is a small business advisor at Financial Models Lab who focuses on startup cost planning for local business owners preparing to launch. He studies common expenses, revenue drivers, and launch requirements to help turn a business idea into a basic, workable plan. George also writes about pricing and profitability basics in a practical, plain-spoken way, with a focus on helping readers make smarter decisions before they open their doors.
Choosing a selection results in a full page refresh.