How Much Does a Dermatology Clinic Owner Make? $199M Year 1
A dermatology clinic owner can make about $169M in Year 1 operating profit before taxes, debt service, reserves, and distributions in this researched model If the owner also works as the lead dermatologist, the model adds a $300k clinical salary, bringing pre-tax owner cash to about $199M before reserves and debt The Year 1 operating margin is about 481% on $351M in net collections These are planning assumptions, not a guaranteed salary or tax-adjusted take-home amount
Owner income$199KNet margin44.1%Revenue for target pay$452KBusiness difficultyMedium
Want to test your dermatology clinic income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to see the Dermatology Clinic financial model?
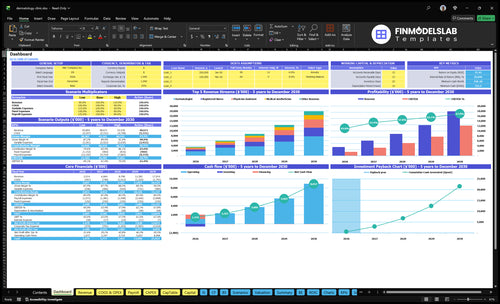
The Dermatology Clinic Financial Model Template shows owner-income planning support, not a promise of earnings, with dashboard charts, assumptions, revenue build-up, cost structure, staffing, debt, and scenarios.
Owner-income model highlights
Net collections and margin
Payroll and overhead charts
Monthly treatments and prices
Provider and capacity inputs
COGS, variable, fixed costs
Debt and scenarios
Cash before reserves
What costs reduce dermatology clinic owner income?
The biggest income drains in a Dermatology Clinic are labor and service cost: Year 1 wages are the largest reduction, COGS runs at 130% of revenue, variable costs at 70%, and fixed overhead is about $16k per month. For the launch-cost side, see How Much Does It Cost To Open And Launch Your Dermatology Clinic Business?—rent or mortgage, insurance, EHR, cleaning, office supplies, billing software, marketing, medical supplies, pharmaceuticals, cosmetic injectables, and skincare all cut operating profit before owner pay. Collections leakage from denials and patient balances is not quantified here, so model it separately.
Main cost drains
Clinical payroll is the biggest Year 1 hit.
COGS can reach 130% of revenue.
Variable costs run at 70%.
Fixed overhead is about $16k monthly.
Profit killers to track
Rent or mortgage reduces margin.
Insurance and EHR add fixed load.
Cleaning, supplies, and billing software matter.
Medical goods and marketing cut take-home too.
How much does a dermatology clinic owner make per year?
A Dermatology Clinic owner can make about $169M in Year 1 operating profit on $351M in net collections in the researched model; if the owner also works as lead dermatologist, the modeled $300k clinical salary is separate and not automatic. By Year 3, modeled revenue reaches $880M and operating profit reaches about $545M, so track What Is The Current Growth Trend Of Patient Engagement At Your Dermatology Clinic? because owner income depends on size, utilization, collections, service mix, debt, and reserves.
Modeled owner cash
Year 1 net collections: $351M
Year 1 operating profit: $169M
Clinical salary data: $300k
Pre-tax owner cash: $199M
Main income drivers
Provider utilization rate
Patient collections quality
Medical versus cosmetic mix
Debt and reserve needs
Does a dermatology clinic owner make more by adding providers?
Yes—if utilization and pricing hold, adding providers can make a Dermatology Clinic more profitable. In the source model, Year 1 with 2 dermatologists and 1 physician assistant at 60% capacity shows $351M revenue and $169M operating profit, while Year 3 with more staff at 78% capacity rises to $880M revenue and $545M operating profit.
Profit grows with scale
$169M to $545M operating profit
$351M to $880M revenue
60% to 78% capacity
More providers lifted output fast
What the model hides
Payroll rises with each hire
Supervision and compliance add load
Room and scheduling pressure increase
Working capital needs get bigger
Dermatology Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Want to see what drives dermatology clinic profit?
1
Provider Utilization
60%-90%
Moving from 60% in Year 1 toward 90% in Year 5 spreads fixed clinic costs over more completed visits.
2
Visit Value
$276-$306
A richer mix of dermatologist and laser visits lifts collections per completed visit without the same jump in overhead.
3
Net Collections
80%
Better payer mix and cleaner claims keep more of each dollar after the 13% COGS and 7% variable cost drag.
4
Clinical Payroll
$928K
Staffing is the biggest cost line in Year 1, so FTE mix and schedule discipline have a direct hit on owner take-home.
5
Fixed Overhead
$16K/mo
Rent, EHR, utilities, and other fixed costs stay in place, so unused rooms or equipment quickly cut margin.
6
Patient Demand
1.77K/mo
Retention, referrals, and lower acquisition cost keep the clinic closer to its monthly treatment ceiling.
Dermatology Clinic Core Six Income Drivers
Provider utilization and appointment volume
Provider Utilization and Visit Volume
When the clinic fills more of its schedule, collections rise because more completed visits and procedures get billed. Year 1 uses 60% capacity and produces about 1,062 completed visits and procedures a month; Year 3 at 78% and Year 5 at 90% would lift volume if reimbursement, staffing, and care quality hold.
Here’s the quick math: moving from 60% to 90% capacity is a 50% increase in utilization, so fixed overhead is spread across more billable work. The risk is overbooking. If waits, errors, or rushed visits rise, the clinic can lose repeat business and owner cash.
How to lift completed visits
Track completed visits, no-shows, room turns, and provider hours by day. Then test the levers that move throughput: tighter schedule templates, faster front desk check-in, better follow-up cadence, more room capacity, and no-show controls. One clean measure matters most: completed encounters per provider hour.
Watch no-shows by provider.
Measure room idle time.
Limit overbooking spikes.
Protect care quality first.
If volume rises without quality slipping, owner pay usually improves because the same fixed costs support more collections. If it doesn’t, extra slots just add friction and lower the value of each visit.
1
Average collections per visit and procedure mix
Average Collections per Visit and Procedure Mix
This driver is the cash collected per completed encounter. In Year 1, the model uses $350 for dermatologist visits, $280 for physician assistant visits, $180 for registered nurse services, $220 for medical aesthetician services, and $300 for laser technician services, for a weighted average of about $276 per visit or procedure.
Mix matters because higher-value, clinically appropriate visits lift revenue without adding as many slots. More dermatologist and laser work can raise owner pay, but only if demand, staffing, consent, and collections stay tight. Low-value mix drags margin. More expensive procedures need steady bookings and clean billing, or cash flow gets choppy. One line: better mix means more dollars per chair hour.
Track Mix by Service Type
Measure completed encounters by provider type, then multiply by collected price. Track dermatology, PA, RN, aesthetic, and laser separately so you can see which services pull the weighted average above $276. If one service is filling the schedule but collecting less, it is lowering owner income even when volume looks fine.
Track collected revenue per provider type.
Watch procedure mix each week.
Test demand before adding higher-price services.
Document consent and billing cleanly.
Skip unnecessary procedures.
Use the mix to forecast cash. If higher-priced services need extra staff time or slower consent, the revenue gain can be delayed. So the real test is not price alone; it is collected dollars per completed slot after labor and billing friction.
2
Payer mix and net collections rate
Payer Mix and Net Collections Rate
Payer mix changes how much billed work turns into cash and how fast it lands. In this model, listed prices are treated as collected revenue, so the owner must track denials, patient balances, and payment lag separately. Self-pay cosmetic visits often collect faster, while insurance work can drag cash and lower margin quality.
Here’s the quick math: better net collections raise distributions without adding visits. The key inputs are billed charges, payer mix by service line, denial rate, collection rate on patient responsibility, and days in receivables. Billing and practice management software fees run 30% of revenue in Year 1 and 25% in Year 5, so weak collections hit cash twice.
Track Cash, Not Just Charges
Measure net collections by payer and by procedure, not just total revenue. Set a monthly target for cash collected versus charges posted, then watch where write-offs and delays start. If insurance claims age out or patient balances stay open, owner pay falls even when the schedule is full.
Denial rate by payer
Days sales outstanding
Patient balance collection rate
Cash by cosmetic versus insurance
Improve it by pushing fast-pay services, confirming coverage before the visit, and collecting patient responsibility up front when allowed. The goal is simple: higher cash per completed visit, lower lag, and less revenue leaking out before it reaches the owner.
3
Staffing leverage and clinical payroll
Clinical payroll leverage
In this clinic, owner income rises only if staffing turns into billable capacity. The listed wages total $1.175M a year, or about $97.9k per month, across the lead dermatologist, associate dermatologist, physician assistant, registered nurse, aesthetician, clinic manager, front desk, and billing specialist. If those hours do not drive completed visits and procedures, payroll eats margin and delays owner pay.
The key test is whether each hire lifts collections faster than it lifts wage cost. Clinical labor should increase room use and procedure volume; admin labor should cut no-shows, clean claims, and keep the schedule moving. If staffing comes in before demand, the same payroll is spread over fewer visits, so profit falls even when the calendar looks full.
Track pay against booked volume
Use visits per labor hour, utilization, and collections per encounter by role. Build the forecast one seat at a time, not as one lump payroll line, so you can see whether the dermatologist, associate, PA, RN, aesthetician, manager, front desk, or billing seat is paying for itself. If a role does not lift volume or cash, freeze the hire.
Measure visits per paid hour.
Hire after demand holds.
Cut empty admin time first.
4
Facility, equipment, and fixed-overhead utilization
Facility and equipment utilization
When rooms, staff, or devices sit idle, fixed overhead still lands. In this model, $16k per month or $192k per year is about 55% of Year 1 revenue, so weak utilization leaves less cash for owner pay even if demand exists.
This driver includes rent or mortgage, utilities, insurance, electronic health record (EHR), cleaning, office supplies, professional fees, and security. The key inputs are room hours, room count, staff coverage, device uptime, and service mix. Contribution margin means revenue left after variable costs; if a service does not clear that bar, more volume just fills space, not income.
Track room and device use
Measure booked versus used hours by exam room, provider, and device each week. A laser or cosmetic setup only helps when demand is real and collected revenue per session covers its variable cost and adds to the fixed load.
Track room hours used.
Separate service margin by type.
Test demand before adding devices.
Cut idle staff and room time.
Use those numbers to keep profitable services on the calendar first, then add equipment only when it improves cash flow and owner draw.
5
Patient demand, retention, and acquisition economics
Patient Acquisition Quality
Marketing and patient acquisition costs run at 40% of revenue in Year 1 and 30% in Year 5. The model also says Year 1 spend is about $1,405k on $351M of revenue, so demand quality matters as much as volume. Strong referrals, reputation, recall systems, and repeat cosmetic visits steady the schedule and support owner pay.
Here’s the catch: paid demand can look good on paper, but weak reimbursement, no-shows, or heavy follow-up work can cut cash. Track contribution margin by channel, not lead count. One clean rule: if a channel fills the calendar but drains cash, it is not helping income.
Track Channel Margin, Not Just Leads
Measure each source by collected revenue minus acquisition cost, no-show loss, and follow-up burden. Inputs that matter: new patients, repeat visits, cosmetic rebookings, reimbursement, denial rate, and time spent on follow-up. That shows which channels actually raise owner draw and which only buy activity.
Compare margin by source monthly.
Watch no-shows by appointment type.
Separate referrals from paid leads.
Price repeat cosmetic visits for cash.
Cut spend on weak channels fast.
Better demand quality lifts utilization and improves cash timing, which matters in a fee-for-service clinic. If a channel fills slots but creates denials or long follow-up chains, it can hurt profit even when topline revenue grows.
6
Dermatology Clinic Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Compare low, base, and high dermatology clinic owner income scenarios
Owner income scenarios
Owner income shifts fast here because revenue depends on provider count, visit volume, and procedure mix, while payroll is the biggest cost. The same clinic can swing from thin to strong cash as capacity fills.
Low, base, and high cases show how staffing and capacity change owner cash.
Scenario
Low CaseLow Case
Base CaseBase Case
High CaseHigh Case
Launch model
This is the lower earnings path, where Year 1 cash is strained by payroll, supplies, and fixed overhead.
This is the modeled path, where the owner also works as lead dermatologist and takes cash after clinic profit.
This is the stronger earnings path, where a larger Year 3 team lifts cash after the same core overhead.
Typical setup
Year 1 runs 2 dermatologists, 1 physician assistant, 2 registered nurses, 1 medical aesthetician, and 1 laser technician at 60% capacity, with $16k monthly fixed overhead and about 20% combined COGS and variable costs.
Year 1 keeps the same 7-provider setup, adds the lead dermatologist salary, and runs about $3.5M of annual revenue against roughly 20% combined COGS and variable costs plus $16k monthly fixed overhead.
Year 3 scales to 3 dermatologists, 2 physician assistants, 4 registered nurses, 2 medical aestheticians, and 2 laser technicians at 78% capacity, with annual revenue near $8.8M and payroll rising with FTEs.
Cost drivers
20% combined COGS and variable costs
$16k monthly fixed overhead
no owner clinical draw
staffing burn
reserve build not included
20% combined COGS and variable costs
$16k monthly fixed overhead
owner lead salary included
payroll grows with staffing
reserve build not included
78% capacity
12 providers
payroll scales with FTEs
17.8% combined COGS and variable costs
$16k fixed overhead
Owner income rangeBefore owner reserves
$169kLow range
$199kBase range
$575kHigh range
Best fit
Use this to test a slower start with tight cash and no extra owner draw.
Use this as the core case for planning owner cash in a stable opening year.
Use this to test upside if the clinic fills schedules and adds staff without losing margin.
!
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
This model shows about $169M in Year 1 operating profit on $351M in net collections, a 481% margin If the owner also works as the lead dermatologist, the model adds a $300k salary That creates about $199M in pre-tax owner cash before debt, reserves, taxes, and reinvestment
Owner income becomes more stable when provider utilization, collections, and staffing are repeatable In this model, capacity rises from 60% in Year 1 to 78% in Year 3 and 90% in Year 5 The practical milestone is not time alone it’s steady completed visits, fewer collection delays, and payroll that matches demand
Not necessarily, but ownership rules and clinical supervision requirements vary by state and structure, so get legal advice Financially, the model separates business profit from clinical pay If the owner fills the lead dermatologist role, the model includes a $300k salary if not, that cash may need to go to an employed physician
Provider utilization, collections per visit, payroll, and overhead drive owner take-home most Year 1 revenue is built from 1,062 completed monthly visits and procedures at about $276 average collections Costs include 130% COGS, 70% variable expenses, $16k monthly fixed overhead, and $9275k in wages
Start with target pay, then test whether collections can support it after costs and reserves With Year 1 contribution margin of 800%, $192k fixed costs, and $6275k non-owner payroll, a $300k owner pay target needs about $140M in collections before debt and reserves Build reserves before treating all profit as distributable cash
About the author
Brian Fox
Local Business Observer
Brian Fox writes for Financial Models Lab with a focus on simple cash flow planning for early-stage founders turning a service idea into a real business. As a local business observer, he explains business costs in plain language and uses startup budget examples to show how revenue, expenses, and profit fit together. His practical, realistic style helps readers understand the numbers behind starting small and building with clarity.
Choosing a selection results in a full page refresh.