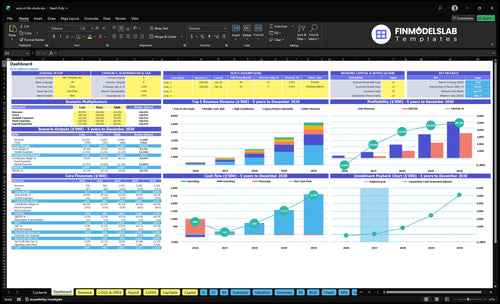
How Much Can An End-Of-Life Doula Owner Make With $338K Revenue
An end-of-life doula owner can model $95,000 of owner salary in the first year if the owner fills the Executive Director role Under the researched assumptions, first-year revenue is $337,920, but known costs produce about -$16,464 before taxes, reserves, admin salary details, and practitioner labor not priced in the data By Year 2, revenue rises to $866,880, with about $380,373 of known-cost profit before those same exclusions Treat these as planning assumptions, not promised earnings or tax advice
Owner income$95kNet margin-9% to 68%Revenue for target pay$867kBusiness difficultyHard
Want the six income drivers?
1
Price Mix
$60-$290
A $120 doula visit and a $250 legacy package push the same case into very different revenue, so mix matters.
2
Caseload
278-3.5K/mo
Monthly services start at 278 in Year 1 and reach about 3,478 by Year 5, which is the main growth engine.
3
Utilization
45%-85%
Capacity moves from 45% on the doula line to 85% on respite care, so better use of time lifts billable output.
4
Referral Flow
8%-6%
Digital marketing and referral outreach fall from 8% of revenue to 6%, so stronger partners protect margin and volume.
5
Staff Mix
$278K-$618K
Wage load climbs from about $278K in Year 1 to about $618K in Year 5, so owner delivery versus hired help changes take-home fast.
6
Overhead
$7.7K/mo
Fixed overhead is $7,650 a month before 8% COGS and 4% travel, so cash stays tight until volume is steady.
Want to test your owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only, not guaranteed salary, tax advice, or owner distribution advice.
Want to check owner income in the End-of-Life Doula Service model?
How much can an end-of-life doula owner make per year?
An End-of-Life Doula Service owner can model $95,000/year as an Executive Director salary in Year 1, but owner distributions are not supported because known-cost profit is about -$16,464 on $337,920 revenue. For setup context, see How Do I Launch An End-Of-Life Doula Service Business?; in Year 2, potential pre-tax profit rises to about $380,373 on $866,880 revenue, before reserves, taxes, admin pay details, and practitioner labor not listed.
Owner Pay
Use $95,000 salary, not guaranteed wage
Year 1 profit: -$16,464
Year 1 margin: about -4.9%
Skip distributions until reserves exist
Upside Case
Year 2 revenue: $866,880
Known-cost profit: $380,373
Pre-tax margin: about 43.9%
Capacity, referrals, and labor must hold
Can an end-of-life doula business scale?
Yes, the End-of-Life Doula Service can scale, but revenue scale is not the same as owner profit. In the model, headcount grows from 4 doulas in Year 1 to 30 in Year 5, while revenue climbs from $337,920 to $5,179,920 — about 15.3x. The catch is simple: true scale means replacing owner labor with trained coverage across legacy, vigil, bereavement, and respite work without letting payroll, training, scheduling, supervision, and quality control crush the margin.
Scale math
4 doulas drive $337,920 in Year 1
30 doulas drive $5,179,920 in Year 5
Revenue grows about 15.3x
Per-doula revenue rises from $84,480 to $172,664
Margin risk
Contractors add coverage fast
Pay and training lower margin
Scheduling and supervision add load
Quality control must stay tight
What should an end-of-life doula charge?
For an End-of-Life Doula Service, charge from source prices as planning rates, not universal US rates: $120 for support, $250 for legacy work, $150 for vigil coordination, $100 for bereavement coaching, and $60 for respite aide work in Year 1. If you’re mapping launch steps, see How Do I Launch An End-Of-Life Doula Service Business? and build packages that spell out hours, on-call access, travel, family meetings, deliverables, and affordability boundaries. By Year 5, the planning rates rise to $140, $290, $170, $120, and $80.
Year 1 rates
$120 end-of-life support
$250 legacy project work
$150 vigil coordination
$100 bereavement coaching
Year 5 rates
$140 end-of-life support
$290 legacy project work
$170 vigil coordination
$120 bereavement coaching
Price the package
Define hours up front
Set on-call access limits
State travel rules clearly
List family meetings included
Keep it clear
List each deliverable
Set affordability boundaries
Use rates as planning inputs
Don’t treat them as universal rates
Key Takeaways
Price scope carefully to protect hourly earnings.
Capacity drives revenue, but quality limits growth.
Referrals lower marketing spend, not payment risk.
Hold reserves after overhead, COGS, and travel.
Compare low, base, and high owner-income scenarios
Owner income scenarios
Owner income moves fast here because service volume, staffing, and referral flow scale together. Year 1 can stay thin, while mature-year capacity lifts profit sharply.
Low, base, and high planning cases for owner income.
Scenario
Low CaseLow Case
Base CaseBase Case
High CaseHigh Case
Launch model
This is the lean Year 1 case with the smallest service load and negative known-cost profit.
This is the modeled Year 2 case with stronger volume, more capacity, and a positive owner result.
This is the mature Year 5 case with the highest capacity, revenue, and owner result.
Typical setup
Year 1-like setup: $337,920 revenue from 278 monthly paid services, 8% COGS, 12% variable costs, $91,800 fixed overhead, and $195,000 known payroll.
Year 2-like setup: $866,880 revenue with more provider capacity and about $380,373 known-cost profit before exclusions.
Mature-year setup: $5,179,920 revenue with the full capacity build-out and about $3,829,333 known-cost profit before exclusions.
Cost drivers
278 monthly paid services
8% COGS
12% variable costs
$91,800 fixed overhead
$195,000 payroll
Year 2 revenue scale
broader capacity
higher staffing
referral flow
price steps
Year 5 revenue scale
full capacity build-out
larger staff mix
price increases
lower unit cost
Owner income rangeBefore owner reserves
-$16,464Low Case Range
$380,373Base Case Range
$3,829,333High Case Range
Best fit
Use this to stress-test cash needs if referrals ramp slowly or staffing stays underused.
Use this for the most likely planning case if referral flow and capacity build as modeled.
Use this to test upside if capacity stays full and demand keeps pace with the year-5 build-out.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
End-of-Life Doula Service Core Six Income Drivers
Package Price And Service Mix
Package Price and Service Mix
In Year 1, package prices run from $60 for respite support to $250 for legacy project work, and the weighted paid service revenue is about $101 per service. By Year 5, the range moves to $80 to $290 and weighted revenue rises to $124, about a 23% lift. That higher average ticket is what raises gross profit and owner pay when the scope stays tight.
The risk is underpricing on-call time, family communication, travel, and emotional labor. If those pieces are bundled for free, a premium package can still earn low margins. One clean rule: price the package by included touchpoints and response windows, not by the headline service name alone.
Price the Full Scope
Weighted revenue is the mix-adjusted average price, or sum(price × mix). That matters because more legacy and planning work lifts cash per client faster than low-priced support hours, but only if delivery time is controlled. If scope creeps, owner income falls even when booked sales look strong.
Use a simple mix sheet to measure this driver: service type, list price, hours spent, travel, after-hours calls, and who delivered it. Compare booked revenue to actual time each month. If one service line takes more unpaid work than expected, raise the fee or narrow the scope before it cuts into take-home income.
Track paid services by type
Log on-call minutes
Count travel and family calls
Review margin by package
Reset scope before renewal
Monthly Paid Services And Caseload
Monthly Caseload Capacity
278 paid services a month in Year 1 and 3,478 in Year 5 means revenue rises fast when capacity stays full. At the disclosed totals, monthly revenue moves from $28,160 to $431,660, so volume is the main top-line engine. If scheduling outruns care coordination, quality slips, referrals soften, and owner pay gets hit.
The doula line shows the same pattern: 108 monthly services at 45% capacity versus 1,440 at 80% capacity. That is a big scale-up, but it only helps income if handoffs, family calls, and follow-up stay tight. More bookings only help when the team can absorb them without burning out.
Track Capacity Before You Push Volume
Measure paid services by role, then compare them with monthly capacity and coordination time. The key inputs are available practitioners, max services per month, utilization, and service mix. Here’s the quick math: 278 × about $101 per service equals $28,160; 3,478 × about $124 equals $431,660.
Track services per doula monthly
Watch scheduling lag and call load
Protect care quality above growth
If utilization rises without enough admin support, unpaid prep and coordination grow, and take-home profit falls even when revenue looks strong. The clean test is whether each added service still clears travel, documentation, and supervision costs.
Overhead, Travel, And Reserves
Overhead, Travel, And Reserves
Take-home here depends on keeping the post-sale cost stack tight. Fixed overhead is $7,650 a month, made up of $3,500 rent, $1,200 liability insurance, $600 software, $450 telecom, $1,500 accounting and legal, and $400 utilities. At $28,160 in Year 1 monthly revenue, that overhead alone is about 27% before taxes, owner pay, or reserves.
Here’s the quick math: 8% COGS plus 12% variable costs leaves 80% before overhead, or about $22,528 on Year 1 revenue. After fixed overhead, about $14,878 remains for owner pay, tax, and reserves. Travel and referral gaps can push cash lower fast, so reserve discipline matters before any distribution.
Track Cost Run-Rate Before Paying Yourself
Measure overhead, travel, and reserves as a monthly cash test, not a year-end cleanup. Keep a simple dashboard with fixed overhead, travel per client, variable cost %, and days of cash on hand. If travel or staffing ramp-up lifts the 12% variable line, owner pay should wait until the reserve target is funded.
Watch overhead against monthly revenue.
Cap travel inside the variable bucket.
Hold reserves before distributions.
Hours Per Client And Utilization
Utilization And Billable Hours
Utilization is the share of available service time that becomes paid work. In Year 1, the model assumes 45% for end-of-life doulas, 30% for legacy specialists, 40% for vigil coordinators, 35% for bereavement coaches, and 50% for respite aides. That means a paid hour can take 2.2 to 3.3 total hours once prep, travel, documentation, family calls, and on-call time are included.
That gap cuts effective hourly earnings fast. If unpaid time is not built into pricing, gross margin shrinks, cash flow gets tighter, and owner pay gets squeezed even when bookings look healthy. One line says it plainly: busy does not mean profitable.
Price The Unpaid Time
Track paid hours, unpaid hours, and utilization by role every month. Break out prep, travel, charting, family calls, and on-call windows so you can see which services really earn. If one role sits near 30% utilization, it needs a higher rate, a minimum booking length, or a fee for travel and calls to protect take-home income.
Measure paid vs total hours.
Separate each service role.
Price travel and on-call time.
Watch burnout before it hits margin.
Forecast owner pay from actual hours.
Here’s the quick math: at 45% utilization, only 55% of capacity is non-billable; at 30%, it jumps to 70%. If scheduling fills faster than care coordination, revenue rises on paper but profit slips in real life. The fix is tighter scope, cleaner time logs, and fees that match the work, not just the visit.
Owner Delivery Versus Contractor Delivery
Owner Delivery vs Contractor Delivery
Owner delivery protects margin because the work is paid by the owner’s own labor, but it caps capacity. This model grows from 12 total service roles in Year 1 to 80 in Year 5, so the real question is whether added contractor revenue is bigger than contractor pay, onboarding, supervision, and scheduling gaps.
Here’s the quick math: more contractor or associate coverage can expand paid services across doula, legacy, vigil, bereavement, and respite lines, but only if care quality holds. Separate owner labor replacement from true profit gain; if a new client only replaces work the owner would have done, take-home income may not improve.
Measure Net Gain per Service Role
Track paid services per role, contractor pay, onboarding time, supervision hours, and fill rate for each line. The inputs that matter are service capacity, utilization, and the gap between billed revenue and delivery cost. If contractor coverage raises volume but leaves schedule holes, the extra revenue can disappear fast.
Test each role on net contribution after delivery costs, not just top-line revenue. A simple check is whether the added role creates more cash than the owner’s own delivery time would have generated. If care coordination slips or response times widen, the model can grow revenue and still weaken owner pay.
Referral Strength And Client Acquisition
Referral Strength And Client Acquisition
Referrals can lower paid marketing pressure and steady demand, but only if they turn into private-pay clients. In this model, digital marketing plus referral outreach runs at 8% of revenue in Year 1 and falls to 6% by Year 5, so every point of referral lift can help profit and owner pay.
The main inputs are referral leads, conversion rate, service price, and case timing. Sources may include elder care partners, funeral homes, senior living contacts, and hospice-adjacent relationships. Here’s the catch: trust and timing drive conversion, and referrals do not guarantee reimbursement, so strong lead flow still needs fast follow-up and clear private-pay terms.
Measure Referral Quality, Not Just Volume
Track referrals received, consult-to-client conversion, and revenue per referral source. If one partner sends many names but few paid cases, that channel is noise. The real metric is cash collected per source after outreach cost, not just introductions.
Set source targets by channel and review them monthly. If referral outreach stays near 8% of revenue in Year 1, it needs enough closed cases to protect margin; if it drifts above plan, owner draw gets squeezed fast. Tight intake scripts, fast response times, and simple private-pay pricing improve conversion without adding much overhead.