How To Open A Genetic Counseling Center In 3 To 6 Months
A lean US genetic counseling practice can usually open in about 3 to 6 months if it starts telehealth-first, cash-pay or referral-led, and avoids waiting on payer revenue for launch The basic sequence is licensure and credential checks, clinical protocols, HIPAA-ready intake, lab workflow, scheduling, staffing, referral outreach, and soft opening In the researched planning assumptions, Year 1 starts with 1 lead genetic counselor, 6 genetic counselors, and 493 modeled monthly consults at capacity-adjusted volume The main bottleneck is qualified counselor availability plus payer or referral credentialing, so first revenue should come from documented cash-pay or referred consults while longer-channel relationships mature
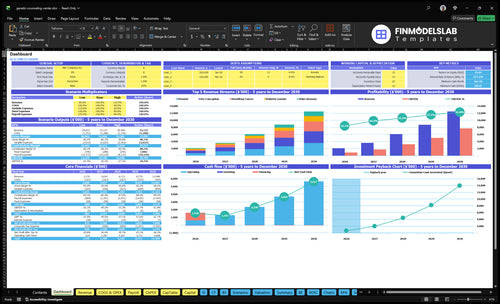
Time to Open3-6 monthsSetup windowLaunch Sequence5 stagesCompliance firstKey BottleneckLicense gateApproval pathFirst Revenue StepPaid consultsIntake ready
Launch timeline
This is the short web summary; the XLSX export holds the detailed Gantt Chart.
What mistakes cause genetic counseling launch risks?
Genetic Counseling launch risk spikes if you open before referral sources are active, assume insurance money starts right away, or hire too slowly for 7 clinical FTE in year 1. The safe move is a soft opening with one specialty focus, while every consult can move from referral to scheduling to intake to a secure visit, note, and follow-up without staff improvising.
Launch mistakes
Open before referrals are live
Count on instant insurance revenue
Underhire for 7 clinical FTE
Leave lab steps vague
Launch fixes
Lock informed consent first
Define test result delivery
Close HIPAA gaps early
Standardize family history intake
Do you need a license to open a genetic counseling practice?
Yes, Genetic Counseling may need state licensure before seeing patients, and for telehealth you must map the rule to the patient’s state, not just your office state. A non-clinical founder may own the practice in some structures, but clinical work should be delivered by qualified counselors; track credential readiness alongside What Is The Most Critical Indicator For Success In Your Genetic Counseling Business? because the U.S. Bureau of Labor Statistics reported $95,770 median annual pay for genetic counselors in May 2023 and 16% projected job growth from 2023 to 2033.
Check before launch
Verify each patient-state license rule
Screen American Board of Genetic Counseling certification
Document scope of service clearly
Secure malpractice coverage before bookings
Watch the bottleneck
Hire for prenatal counseling coverage
Cover hereditary cancer consults
Add pediatric and pre-conception capacity
Staff direct-to-consumer test interpretation
How do you get clients for a genetic counseling practice?
For a Genetic Counseling practice, the first clients usually come from medical referral pathways, not broad ads, and the first win is a booked consult with completed intake, family history, consent, and referral note workflow; see How Much Does It Cost To Open And Launch Your Genetic Counseling Business? for the launch side. Focus on women’s health practices, oncology groups, fertility clinics, pediatric specialists, and primary care groups with clear referral criteria. Build specialty pages for pre-conception, prenatal, hereditary cancer, direct-to-consumer interpretation, and pediatric genetics, with Year 1 prices of $350, $375, $400, $250, and $425.
Top referral paths
Women’s health practices send early cases
Oncology groups need hereditary cancer support
Fertility clinics drive pre-conception work
Primary care groups need clear criteria
Track from day one
Track referral source for every lead
Count booked consults, not just inquiries
Watch no-shows and follow-up needs
Send fast reports back to clinicians
Key Takeaways
Licensed counselors and compliance must be ready first.
Lab workflows need clear ordering and result rules.
Choose pricing and billing before the first consult.
Referral channels and telehealth systems drive early volume.
Licensed Clinical Capacity
Licensed Clinical Coverage
Clinical capacity is the first launch gate because no referral pipeline matters if there is no licensed counselor available to take the consult. A Year 1 plan with 1 lead genetic counselor and 6 genetic counselors only works if coverage is mapped by state, specialty, and schedule before opening.
The launch risk is simple: hire too late, or promise more states than the team can legally cover. Each service line — pre-conception, prenatal, hereditary cancer, direct-to-consumer interpretation, and pediatric genetics — needs a clear scope, documentation standard, and telehealth rules, or day-one booking slows and compliance gaps show up fast.
Cover Before You Market
Before launch, verify each counselor’s credential, licensure, and scope of practice, then build a coverage grid that shows who can serve which state and service line. That is the readiness check. If a new referral lands in a state without coverage, the visit should not be offered.
Check state-by-state licensure.
Map specialty to service line.
Test note templates and escalation rules.
Train on onboarding scripts first.
Hold back uncovered states.
1
Compliance And Privacy Systems
Day-One HIPAA Controls
If intake, consent, and record handling are not locked before launch, this business cannot safely open. Health Insurance Portability and Accountability Act (HIPAA) is the US privacy and security rule set for protected health information, and for genetic counseling it has to work on day one, not live in a policy binder. Private video visits, secure intake, medical record storage, and referral reporting all need to be ready before the first consult.
The weak point is usually consumer-grade forms or vague data sharing. That creates privacy risk, slows referrals, and makes payer or partner talks harder. Strong controls here also support malpractice coverage, since insurers and referral partners want to see clear access controls, consent language, record retention workflow, and staff training before they trust the operation.
Lock The Workflow Before First Booking
Build the compliance path in the same order the patient moves: secure intake, consent capture, counselor review, visit, note storage, and referral report. Tie each step to the EMR setup and telehealth workflow so nothing sits in email or consumer chat tools. Here’s the quick rule: if staff can’t show where genetic information enters, who can see it, and where it is stored, the launch is not ready.
Publish privacy notices and consent language
Set role-based access controls
Define record retention and deletion steps
Train staff before first patient contact
Test private video visits end to end
Confirm malpractice coverage matches services
What this setup buys you is cleaner referrals and fewer partner questions. What it hides is time drag: if EMR setup or telehealth workflow slips, the opening date slips too, because the team still cannot handle protected health information safely from the first appointment.
2
Lab And Testing Workflow
Lab Workflow Readiness
Genetic counseling cannot open cleanly if test ordering and result flow are still vague. The launch risk is promising direct test ordering or result review before the team has a written route for physician-coordinated orders or lab referral only. Without that, day-one visits stall, follow-up gets missed, and referral partners lose confidence fast.
This workflow has to cover consent language, hereditary cancer panels, prenatal screening, pediatric result review, result delivery rules, and triggers for a follow-up visit. One clean path per test type matters more than broad marketing. If the lab side is not ready, opening slips because counseling, documentation, and patient handoff all depend on it.
Lock the Test Path
Build a written matrix for each of the 5 service lines: who can order, how results arrive, who reviews them, and when a follow-up visit is required. Tie each step to the EHR, consent form, and referral note before soft opening. That protects day one operations and keeps the team from improvising with families in real time.
Map order steps by test type.
Set result delivery rules.
Define follow-up triggers.
Test consent and documentation.
Confirm lab handoff timing.
Do not market test-related services until the ordering and reporting path is signed off. Otherwise, bookings can come in before the team can close the loop, which slows first revenue and weakens trust with patients and physicians.
3
Payment And Billing Setup
Payment Path and Billing Rules
Cash-pay pricing or insurance credentialing decides whether the practice can open on time. If you wait for payer approval, first revenue can slip even when counselors and telehealth are ready; a chosen opening path lets bookings start on day one with clear prices: $350 pre-conception, $375 prenatal, $400 hereditary cancer, $250 direct-to-consumer interpretation, and $425 pediatric genetics.
Set the fee schedule, refund policy, eligibility check, and documentation standards before launch. That cuts billing disputes and makes the first consult smoother, because clients know what they owe and staff know whether to collect cash, send a superbill, a visit summary clients can send to insurance, or submit a claim.
Lock the Billing Route Before You Market
Pick one opening path: cash-pay, employer/direct-pay, referral-based, or insurance credentialed. Then test the full workflow end to end: intake, price quote, consent, note template, superbill or claim flow, and payment capture. If insurance is part of the plan, start payer enrollment early so approval does not stall launch. One clean workflow beats four half-finished ones.
Confirm one opening payment path.
Document refund and eligibility rules.
Train staff on claim steps.
Test first-visit billing before launch.
4
Referral Pipeline
Referral Pipeline
If you open without trusted referral sources, you’ll rely on website traffic alone, and that usually brings weaker-fit cases and higher marketing waste. For this business, the referral network is the practical demand engine: it should be live before day one, tied to OB-GYN groups, oncology practices, fertility clinics, pediatric specialists, and primary care groups.
The readiness check is simple: a short list of active sources with referral criteria, a clear scheduling path, and report expectations. With the Year 1 staffing plan of 1 lead genetic counselor plus 6 genetic counselors, outreach only works if clinical capacity and lab workflow are already set, or you’ll create delays, missed follow-up, and thin first-month revenue.
Build the medical channel first
Before outreach, prepare a one-page referral guide, specialty-specific landing pages, secure referral intake, turnaround expectations, and sample consult reports. That gives physicians a clean handoff and tells them exactly when patients will be seen and how results will come back. In this model, the goal is not more traffic; it’s more trusted referrals that can book right away.
Use the launch gate as a test: can a new referral source send a patient, get the right intake path, and receive a report without manual scrambling? If not, delay the outreach push. The faster path is to verify state coverage, note templates, and lab/result flow first, then open the channel in a controlled way.
Confirm counselor coverage by state.
Map referral criteria by specialty.
Test secure intake before launch.
Set report turnaround expectations.
Track first referrals by source.
5
Telehealth And Operations Infrastructure
Telehealth Workflow
If the intake-to-visit workflow is clunky, you won’t open on time. Telehealth genetic counseling has to move smoothly from online scheduling to family history intake, consent capture, secure video visit, clinical note, follow-up reminder, billing handoff, and referral report. Until each step works end to end, every consult takes longer and counselor capacity drops.
The Year 1 model assumes telehealth platform fees at 30% of revenue and EHR/CRM per-user license costs at 20%, so admin time is not free. The real launch risk is manual drag: missed uploads, slow reminders, and messy follow-up queues. Those errors can delay first revenue, hurt patient trust, and force extra staffing before demand justifies it.
Test the Full Visit Path
Before soft opening, verify appointment types, reminder cadence, no-show rules, document upload, and the result follow-up queue. Test one full case from booking to report so staff know who does what, when the note closes, and where the billing handoff lands. One broken step can slow every consult.
Test online scheduling and intake.
Confirm consent capture on every visit.
Check secure video and note templates.
Assign follow-up queue ownership.
Set billing handoff timing.
If onboarding takes too long or the queue is manual, the team will spend day one on admin instead of counseling. That lowers utilization and makes the schedule look fuller than it is. Keep the workflow simple enough that a new counselor can start seeing patients with clean records on day one.