How Much Does a Gynecology Clinic Owner Make? $407K–$452M
You’re estimating owner take-home from a US gynecology clinic, not an employed physician salary In the provided five-year model, gynecology clinic revenue grows from $165M in the first year to $735M in the mature year, with operating profit before owner taxes, reserves, and debt service rising from $407K to $452M
Owner income$407K to $4.52MNet margin25% to 62%Revenue for target pay$7.35MBusiness difficultyHard
What drives gynecology clinic income most?
1
Patient Volume
1.3K-5.3K/mo
More visits spread the $22.5K fixed base and staff time across more billable work, which lifts owner take-home fastest.
2
Collections
$102-$116
Each visit is worth about $102 to $116 collected, so cleaner claims and payer mix raise cash without adding rooms or staff.
3
Service Mix
$40-$330
The mix matters because prices run from $40 for medical assistant services to $330 for sonography, so higher-value visits lift revenue per slot.
4
Capacity
60%-90%
Higher capacity turns the same clinician payroll into more billable visits, so underused schedules drag income fast.
5
Labor Overhead
35%-40%
Payroll plus billing fees start near 40% and improve to 35%, and every point saved drops straight to EBITDA.
6
Fixed Costs
$22.5K/mo
Fixed costs are $22.5K a month before debt and reserves, so weak months cut owner cash even when demand is steady.
Want to test your clinic owner income?
Owner income calculator
Estimate owner take-home and the gap to target pay from revenue, margin, costs, reserves, and target pay.
!
Planning note: This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
Want to see the Gynecology Clinic forecast?
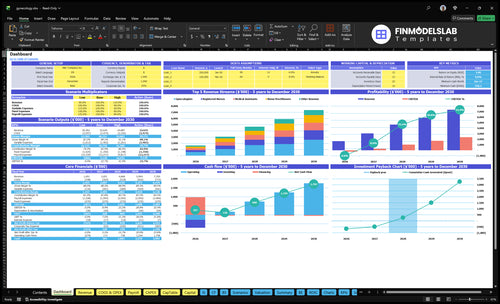
The Gynecology Clinic Financial Model Template shows patient volume, payer mix, staffing, expenses, debt, cash flow, and owner take-home; the dashboard tracks revenue from $165M to $735M and operating profit from $407K to $452M. Open the model.
Owner-income model highlights
Owner take-home scenarios
Revenue and margin flow
Assumptions change fast
What gynecology clinic operating costs reduce owner profit most?
At a Gynecology Clinic, payroll and revenue-linked costs cut owner profit most. If you’re sizing the numbers in How Much Does It Cost To Open A Gynecology Clinic?, the biggest hits are a $250K senior gynecologist, $200K staff gynecologist roles, and supplies and lab fees at 120% of revenue in year one and 105% in a mature year.
Biggest payroll hits
$250K senior gynecologist
$200K staff gynecologist roles
$120K clinic director
$45K receptionist/admin roles
Fixed overhead pressure
$22,500 fixed costs per month
$270K fixed costs per year
$12K rent per month
$3K malpractice and $2.5K EHR monthly
How do solo and multi-provider gynecology clinics compare?
A solo Gynecology Clinic depends on the owner-clinician’s own output, while a multi-provider clinic adds more visit capacity but also more management work. In the model here, staffing scales from 2 gynecologists and 1 nurse practitioner in year one to 5 gynecologists and 3 nurse practitioners in the mature year, with monthly visits rising from 1,348 to 5,271 and revenue from $165M to $735M. That growth also means more scheduling, supervision, billing, compliance, hiring, cash reserves, and a separate legal review of state ownership and professional entity rules.
Solo clinic
Runs on owner-clinician time
Revenue follows one schedule
Lower management load
Less capacity to scale
Multi-provider clinic
Scales visits from 1,348 to 5,271
Adds 3 nurse practitioners
Needs stronger billing and compliance
Needs more cash reserve planning
How much revenue does a gynecology clinic need for owner income?
The revenue target for a Gynecology Clinic comes from the owner-pay goal divided by the operating margin in the model. Here’s the quick math: $407K owner income needs about $165M in annual revenue at 247% margin in year 1, and $452M needs about $735M at 615% margin in the mature year.
Year 1 math
$407K owner income
$165M annual revenue
247% margin used
1,348 visits per month
Mature year math
$452M owner income
$735M annual revenue
615% margin used
$102 to $116 per visit
Key Takeaways
Visits drive revenue, but capacity must keep up.
Collections lag billed work, so cash needs tracking.
More service mix can lift margins and costs.
Fixed costs and reserves set the break-even floor.
Compare low, base, and high owner-income cases
Owner income scenarios
Owner income shifts with visit volume, pricing, and staffing depth. The low case is ramp-up; the high case reflects a fuller schedule and stronger operating profit.
How ramp-up, scaled, and mature clinics change owner income.
Scenario
Low CaseRamp-up
Base CaseScaled
High CaseMature
Launch model
This is the ramp-up income path with first-year volume.
This is the modeled income path for a scaled clinic.
This is the stronger income path for a mature clinic.
Typical setup
It uses 1,348 visits a month, $165M revenue, a 247% margin, and $407K operating profit before taxes, reserves, and debt.
It uses 3,482 visits a month, $467M revenue, a 533% margin, and $249M operating profit.
It uses 5,271 visits a month, $735M revenue, a 615% margin, and $452M operating profit.
Cost drivers
Visit volume
staffing mix
pricing per visit
billing fees
supply and lab costs
Visit volume
provider count
pricing per visit
billing fees
labor utilization
Visit volume
provider capacity
pricing per visit
margin mix
fixed overhead
Owner income rangeBefore owner reserves
$407KRamp-up case
$249MScaled case
$452MMature case
Best fit
Use this to stress-test opening-month demand and early staffing.
Use this as the core planning case for staffing and cash flow.
Use this to test upside if demand and capacity both stay strong.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Gynecology Clinic Core Six Income Drivers
Patient Volume And Schedule Capacity
Patient Volume and Schedule Capacity
When patient volume rises, collected revenue rises before expense control helps. This model moves from 1,348 visits per month in year one to 5,271 visits per month in the mature year, or about 3.9x more volume. The provider plan also expands, with gynecologist capacity rising from 600% to 850% and nurse practitioner capacity from 650% to 900%.
That only pays if rooms, billing, staff, and care quality keep pace. No-shows and long appointment cycles cut revenue without cutting all fixed costs, so the owner can miss cash even when the schedule looks full. In a fee-for-service clinic, every empty slot is lost income that still leaves rent, payroll, and software to cover.
Track Visits, Not Just Bookings
Measure kept visits, no-show rate, visit length, room turns, and provider utilization each week. The useful inputs are booked visits, completed visits, average visit time, provider hours, rooms available, and billing lag. If kept visits trail booked visits, the schedule is not converting into cash, and owner pay drops even when demand looks strong.
Track booked versus completed visits.
Watch no-shows by provider.
Test shorter cycle times.
Match staffing to peak demand.
Here’s the quick math: more visits help only when the clinic can bill them and deliver them well. If capacity rises but follow-up is slow, claims lag, or care quality slips, revenue quality falls and fixed costs stay put. The owner should forecast cash from actual completed visits, not just open slots.
Provider Staffing And Productivity
Provider Staffing And Productivity
Provider staffing sets both revenue capacity and payroll burden. The model scales from 2 gynecologists, 1 nurse practitioner, 2 registered nurses, 3 medical assistants, and 1 sonographer to 5, 3, 6, 8, and 2. Physician pay already includes a $250K senior gynecologist and a $200K staff gynecologist, so each added clinician has to create enough billed work to cover salary, support staff, and slower ramp time.
Productivity is the key input here: the model uses 160 to 320 monthly treatments before capacity adjustments. If scheduling, supervision, and handoffs run cleanly, more staff can lift collected revenue and owner draw. If they do not, payroll grows faster than visits, and margin gets squeezed even when the clinic looks busy.
Measure Capacity Before You Hire
Track treatments per provider per month, booked hours, no-shows, and the gap between scheduled and completed visits. One clean check: if a new hire does not raise completed treatments enough to cover pay plus support labor, delay the hire or reduce hours.
Use monthly treatments as the core KPI.
Test handoff time between roles.
Watch payroll as a share of collections.
Match staffing to booked demand, not hope.
Service Mix And Procedure Revenue
Service Mix And Procedure Revenue
Service mix changes take-home pay because higher-price visits and procedure-heavy services do not carry the same margin. In the model, mature-year prices run from $45 for medical assistant work to $330 for sonography, with gynecologist at $280, nurse practitioner at $170, and registered nurse at $90. If sonography rises from 60 to 204 visits per month, that line alone moves from $19,800 to $67,320 in monthly revenue.
Track Margin by Service Line
Measure each service by price, volume, supply cost, lab fee, labor time, and reimbursement cap. Procedure-heavy revenue can help cash flow, but only if the spread after variable costs stays positive. A sonography visit at $330 looks strong until staffing, equipment, and consumables are loaded in. One clean test: compare revenue per hour across roles, then shift schedule time to the highest margin services.
Track visits by role monthly.
Load all direct costs per service.
Watch denial and reimbursement delays.
Fixed Costs, Risk Costs, And Reserves
Fixed Costs And Cash Floor
$22,500 a month in fixed costs is the clinic’s cash floor before owner pay starts. That equals $270,000 a year, with $12,000 rent, $3,000 malpractice insurance, $2,500 EHR software, and $5,000 for utilities, cleaning, IT support, office supplies, and business insurance.
Here’s the quick math: if collections dip, this monthly nut still has to be paid. Debt service and reserves can tighten cash even when they do not show up in operating expenses, so owner distributions depend on cash after fixed costs, not just booked profit.
Track The Cash Floor
Build the forecast around fixed costs, then test how many collected visits are needed to cover them. The key inputs are monthly rent, malpractice, EHR, utilities, and debt payments, plus a reserve target for slow collections or claim delays.
Track fixed cost burn monthly.
Separate debt service from profit.
Hold cash for reserves.
Stress test lower visit volume.
If collections slip or payer delays stretch out, owner income drops fast because these costs do not flex with patient volume. The clinic only starts paying the owner after it clears the $22,500 monthly base and keeps enough cash for reserves.
Payer Mix And Collections
Payer Mix And Collections
Payer mix changes how much billed work turns into cash. Here, sticker prices range from $250 to $280 for gynecologist visits, $150 to $170 for nurse practitioner visits, and $300 to $330 for sonography, but blended collected revenue is only about $102 per visit in year one and $116 in a mature year.
That gap hits owner pay fast. Deductibles, denials, patient balances, and claim timing can pull cash below model revenue, so the real question is collections per completed visit. At 1,348 monthly visits, cash is about $137,496 at $102 per visit or $156,368 at $116.
Track cash per visit
Build the calculator around average collected revenue per visit, not charges. Track completed visits, collected cash, denial rate, patient balances, and days to cash by payer. If one payer pays slower or rejects more claims, take-home drops even when the schedule stays full.
Test front-end collection work and claim follow-up often. One clean metric is collected cash ÷ completed visits. If that number slips, fixed payroll and rent still land, and owner distributions get squeezed.
Labor, Billing, And Admin Overhead
Labor, billing, and admin overhead
Labor here means receptionist/admin support, billing and collections, patient acquisition marketing, and the clinic director layer. In this model, admin staffing rises from 20 FTE to 40 FTE at $45K each, so payroll goes from $900K to $1.8M a year. The director stays at 10 FTE at $120K, so the real question is whether that extra overhead protects collections and patient flow enough to pay for itself.
Cutting staff blindly can backfire. Billing and collections fees fall from 40% to 35% of revenue, and patient acquisition marketing falls from 30% to 25%, but denial work, prior authorizations, scheduling, and patient balances still decide how much booked revenue turns into cash. If those tasks slip, owner take-home drops even when booked visits look strong.
Track collections, not just headcount
Watch cash collected per booked visit, denial rate, prior auth turnaround, days in accounts receivable, and patient balance collection rate. Those are the controls that show whether admin labor is earning its keep. If staffing rises but collections lag, the clinic is paying for more people without getting more cash.
Stress-test any hiring plan against the fee drops from 40% to 35% and 30% to 25%. The gain only works if the team keeps claims clean, schedules full, and collects balances on time. One weak front desk or billing process can erase a lot of owner profit.