How To Open A Gynecology Clinic: 6 To 12 Month Launch Roadmap
Gynecology Clinic Bundle
You’re opening a clinical business, so the launch plan has to line up licensure, space, payer enrollment, staff, systems, and first patient flow before the doors open Use a 5-year planning period, with Year 1 built around 2 gynecologists, 1 nurse practitioner, 2 registered nurses, 3 medical assistants, and 1 sonographer Validate the launch sequence against capacity, collections, and cash runway before signing the lease
Time to Open12 monthsSetup windowLaunch Sequence8 stagesLicense firstKey BottleneckPayer delayEnrollment lagFirst Revenue StepBooked consultsBooking live
Launch timeline
This is a short web summary of the launch plan; the XLSX export contains the detailed Gantt Chart.
How long does it take to open a gynecology clinic?
For a Gynecology Clinic, the practical US planning range is 6 to 12 months. Legal setup, lease search, payer credentialing, buildout, inspections, EHR implementation, equipment delivery, and hiring can overlap, but they still set the launch order. Start payer enrollment and EHR setup before buildout ends, hire clinical staff before soft opening, and only open once insured and self-pay scheduling, intake, consent, billing, and provider coverage are live.
What drives the timeline
6 to 12 months is the planning range.
Lease and legal work start first.
Payer credentialing runs in parallel.
Buildout and inspections still gate launch.
What must be live first
EHR setup should finish early.
Hire staff before soft opening.
Test appointment templates before day one.
Open only with billing and coverage ready.
What launch mistakes delay a gynecology clinic opening?
The biggest launch mistake for a Gynecology Clinic is opening before payer contracts and billing setup are live, because cash collections can lag even when the schedule is full. Front-desk workflow, referral channels, clinical policies, untested EHR templates, and gaps in the provider schedule can slow opening too. For Year 1, plan around 2 gynecologists, 1 nurse practitioner, 2 registered nurses, 3 medical assistants, and 1 sonographer.
Common launch blockers
Open contracts before claims go out
Underbuild front-desk flow
Launch with weak referral sources
Skip EHR template testing
Readiness checks first
Keep malpractice coverage active
Document privacy and safety policies
Test insurance verification before day one
Stock exam rooms and test lab flow
How do you get first patients for a gynecology clinic?
If you want first patients fast, build local search, service pages, online scheduling, insurance directory listings, and referral ties before opening, and map startup spend with How Much Does It Cost To Open A Gynecology Clinic?. Then push first-available appointment slots for preventive exams, consultations, contraception visits, ultrasound visits if offered, insured visits, and self-pay visits, because booked visits drive first revenue.
Keep reviews compliant through post-visit workflows only, and remember collections depend on payer contracts, eligibility checks, coding, and claim submission. In the Year 1 model, patient acquisition is set at 30% of revenue, or about $4,127/month.
Fill the schedule
Launch local search presence early
Publish service pages before opening
Add online scheduling from day one
List insured and self-pay visits
Support collections
Join insurance directories
Build primary care referrals
Create reproductive health pages
Use compliant post-visit reviews
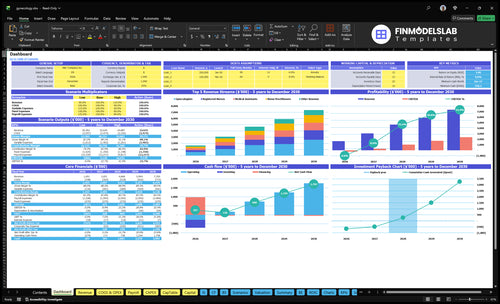
Gynecology Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Gynecology clinic opening checklist objective
Launch readiness checklist
Use this go-live approval checklist before opening the gynecology clinic.
1Regulatory clearance
Entity formation completeCritical
You need a legal entity before contracts, permits, and insurance bind.
Licensure and scope verifiedCritical
Provider scope has to match state rules for gynecologists, NPs, RNs, MAs, and sonographers.
Malpractice policy boundCritical
Coverage at the model's $3,000 monthly cost should be active before any patient visit.
HIPAA and OSHA files readyCritical
Privacy controls and workplace safety files need to be in place before opening.
2Clinical policy
Consent forms approvedHigh
Clear consent helps reduce disputes and supports safe care before first visits.
CLIA test need decidedHigh
In-office lab work may need CLIA certification, so decide before testing starts.
Clinical policies signed offHigh
Policies should cover escalation, privacy, room flow, and emergency handling.
3Clinic buildout
Exam rooms inspection readyCritical
Rooms must be clean, private, and ready for safe exams.
Ultrasound workflow testedHigh
Imaging flow must work before the first scan is booked.
Supplies and storage stockedHigh
Stock, sterile storage, and basic supplies should not stall visits.
Accessibility path clearedHigh
Patients need safe access before you open the doors.
4Systems and billing
EHR live and validatedCritical
The $2,500 monthly EHR needs tested notes, charts, and workflows.
Scheduling and reminders testedHigh
Booking and reminder flows keep no-shows and intake errors down.
Billing claims test passedCritical
Claims need to clear before you depend on first cash from payers.
Payer enrollment confirmedCritical
Without payer setup, revenue can lag even if visits start.
5Staffing and coverage
Coverage schedule setCritical
Every clinic day needs named coverage across providers and support staff.
Role scope matrix approvedHigh
Clear task lines help gynecologists, NPs, RNs, MAs, and sonographers work safely.
Training drills completedHigh
Staff should practice intake, triage, room turnover, and issue escalation.
6Cash and launch
Cash runway to Month 13Critical
The model's minimum cash point is Month 13, so funding has to cover that gap.
Breakeven Month 14 reviewedHigh
Breakeven at Month 14 means early volume still won't cover fixed costs.
Launch marketing readyMedium
The first patient flow needs clear outreach, booking prompts, and local visibility.
Go-live signoff approvedCritical
Do not open until contracts, policies, coverage, EHR, and claims tests are complete.
Which launch drivers matter most before opening?
1Licensing Compliance
License gate
State board, privacy, safety, consent, and lab rules must be in place before any patient care starts.
2Payer Billing
Claims live
Active payer setup and claim testing first, or insured visits can sit unpaid and need rework.
3Location Setup
6-12 mo
The room layout must support privacy, sterilization, and ultrasound flow before first patients.
4Staffing Coverage
9 staff
Year 1 staffing supports about 1,348 monthly visits, so hiring pace sets opening throughput.
5EHR Workflow
$2.5K/mo
Test booking, intake, claims, and reminders before launch so documentation stays clean and front-desk work stays light.
6Referral Engine
$4.1K/mo
At about $137,580 monthly revenue, 30% acquisition spend is roughly $4.1K to keep slots full.
Licensing And Compliance Readiness
Licensing Before Opening
Compliance is a launch gate, not back-office cleanup. Before the first patient, confirm state medical board rules, clinician licenses, ownership or supervision rules, malpractice coverage, privacy controls, workplace safety files, informed consent, patient records, and scope-of-practice rules. HIPAA means patient privacy and security rules, OSHA means workplace safety rules, and CLIA means lab testing rules.
If the clinic plans in-office tests, decide whether they trigger CLIA requirements before you open. One missing license, policy, or lab setup can push the launch date, block day-one visits, or force reschedules. No compliant clinical setup means no safe opening.
Clear the License File Early
Build a pre-open compliance file and assign one owner to each item. Verify licenses, supervision terms, malpractice policy, privacy controls, safety logs, and consent forms before staffing or marketing ramps up. Open only after the clinic can prove it is ready to treat patients safely.
Check license status and expiry dates.
Confirm supervision and ownership rules.
Decide if tests need CLIA.
Test records, consent, and privacy files.
Document workplace safety steps.
1
Payer Credentialing And Billing Setup
Claims Ready Before Day One
Payer enrollment sets up first collections. For a gynecology clinic, that means getting Medicare, Medicaid where relevant, and commercial payer contracts active before the first visit so insured patients do not turn into delayed cash, rework, or self-pay friction.
Here’s the quick math: the Year 1 model assumes 40% billing and collections fees, so weak setup can hit cash hard right away. Claims testing should happen before opening week, or front-desk work, coding, and denials will slow down day-one operations.
Test The Full Billing Path
Build and test the full path before launch: provider credentialing, billing workflows, coding templates, eligibility checks, claim submission, denial routing, and patient payment policies. One clean test visit should run from intake to claim so the team sees where claims break, where the payer rejects data, and where staff need a script.
Verify payer status before booking
Load coding templates before first patients
Test eligibility checks in advance
Route denials to one owner
Set payment rules for self-pay cases
If payer contracts are not active at opening, even insured visits can stall. That creates cash lag, more manual follow-up, and a rough first impression for patients who expected normal insurance billing from day one.
2
Location And Exam-Room Setup
Location and Room Setup
For a gynecology clinic, the site and room layout are launch gates, not cosmetics. You need privacy, clear waiting-room flow, accessible entry, exam rooms, procedure readiness, storage, sterilization workflow, signage, and space for ultrasound if offered. If the layout is weak, opening day turns into delays, awkward patient movement, and a lower-trust first visit.
The operating cost load is already set at $12,000 monthly rent, $1,500 utilities, $1,000 cleaning, and $800 general office supplies. Here’s the quick math: the space must be ready before revenue starts, because vendor lead times on furniture, exam tables, medical supplies, ultrasound equipment, IT, and waste handling can push the first patient date back.
Lock the Floor Plan Early
Verify the room count, patient path, and storage plan before signing off on buildout. The founder should sequence furniture, exam tables, supplies, IT, and waste pickup in that order, since one late item can block opening-week flow. If ultrasound is part of day-one care, reserve the footprint and power needs now, not after the lease is signed.
Check privacy from lobby to exam room
Measure access for mobility needs
Test sterilization and storage flow
Confirm signage before first patients
Track lead times for all vendors
What this setup hides is timing risk: if any core item slips, staff may be ready but the clinic still cannot serve patients safely or smoothly. A clean room plan also reduces opening-week bottlenecks, which matters when the first visits shape trust and repeat use.
3
Clinical Staffing And Provider Coverage
Staffing and Coverage
Staffing is the gate that turns rooms into appointments. This plan assumes 2 gynecologists, 1 nurse practitioner, 2 registered nurses, 3 medical assistants, and 1 sonographer. At Year 1 utilization, that supports about 192 gynecologist visits, 130 nurse practitioner visits, 336 registered nurse services, 630 medical assistant services, and 60 sonography visits a month. If even one role starts late, the schedule breaks before the first patient walks in.
No coverage, no clean launch. For a gynecology clinic, staffing has to match compliance, service mix, room flow, patient intake, and documentation from day one. Thin coverage means longer waits, more canceled visits, and slower chart closure, which can hurt patient trust and early cash flow.
Build the schedule before hire dates slip
Lock the staffing map against room count and clinic hours before opening. Set each role’s start date, backup coverage, and training plan, then test a full patient day with intake, vitals, provider visits, sonography, and charting. If the test day needs overtime or skipped breaks, the launch plan is too tight.
Verify scope for each role.
Match staff to room blocks.
Train on intake and documentation.
Plan cross-coverage for absences.
One missing medical assistant can slow every room. That’s why the founder should confirm onboarding, policies, and handoffs before the first appointment is booked. Clean staffing up front is what keeps the clinic open on time and cuts day-one cancellations.
4
EHR And Patient Workflow
EHR Workflow Test
If the clinic opens before the EHR works end to end, day one gets messy fast. The system must handle booking, intake, insurance checks, reminders, lab and ultrasound notes, coding, consent, and claims before the first patient walks in. The modeled subscription is $2,500 per month, so this is a launch cost, not an afterthought.
Test one full visit from online booking to claim submission before opening week. If any step breaks, expect slower checkout, more front-desk work, and billing errors that delay cash. Clean documentation is the real launch gate here.
Pre-Launch System Run
Build the workflow in the same order staff will use it: appointment templates, patient portal, intake forms, verification, reminders, visit notes, coding templates, consent, and claims. Use one test chart for a preventive visit and one for a procedure or ultrasound visit, so you catch gaps in documentation and billing rules before patients do.
Confirm room-by-room visit flow.
Test insurance verification timing.
Check claim fields and coding.
Verify lab and ultrasound documentation.
Train front desk on exceptions.
If setup slips, opening can still happen on paper, but not in practice. Staff will spend the first week fixing tickets instead of moving patients through the visit, and that raises stress, wait times, and denied claims.
5
Referral And Patient Acquisition Engine
Booked Visits First
Demand generation has to create booked visits before opening day, not just awareness. The model puts Year 1 acquisition marketing at 30% of revenue, and the planning figure shown is $4,127 per month at about $137,580 in monthly revenue. If local search, directory listings, referral outreach, and online booking are not live, the clinic opens with empty slots and weak day-one cash flow.
Pre-Launch Demand Setup
Set up the booking path before staff see the first patient. Verify the Google Business Profile, insurance directory data, service pages, and online scheduling, then test that a patient can move from search to appointment without a phone call. One clean scheduling flow matters more than broad awareness.
Confirm physician referral outreach.
Line up primary care relationships.
Test compliant review request steps.
Match spend to booked appointments.
If these channels are late or broken, the front desk spends day one chasing calls instead of filling the calendar, and early visits for preventive exams, consultations, contraception care, and ultrasound services slip past the opening window.
Start with the legal and clinical gates first: entity setup, state medical board rules, licensed clinicians, malpractice coverage, and patient privacy policies Then run lease, EHR, payer credentialing, staffing, and marketing in parallel The planning case uses a 6 to 12 month launch window and a Year 1 team of 2 gynecologists, 1 nurse practitioner, and 6 other clinical staff
Plan on 6 to 12 months for a US gynecology clinic because payer credentialing, buildout, inspections, and hiring often control the date The work can overlap, but the clinic should not open before provider schedules, EHR workflows, claims testing, and exam rooms are ready A soft opening helps test patient intake and billing before full volume
You need properly licensed clinicians, and state rules decide ownership, supervision, and scope of practice The model assumes 2 gynecologists in Year 1, supported by 1 nurse practitioner, 2 registered nurses, 3 medical assistants, and 1 sonographer If advanced-practice providers handle visits, confirm supervision, prescribing, documentation, and billing rules before launch
The common delays are payer enrollment, facility buildout, clinical hiring, EHR configuration, and incomplete compliance files Opening before insurance contracts are active can slow collections even when appointments are booked Build readiness around the first revenue path: consultations, preventive exams, contraception visits, sonography if offered, and clean claims submission
Check whether launch capacity, staffing, and fixed commitments fit the ramp In Year 1, modeled capacity is about 1,348 monthly visits and about $137,580 in monthly revenue Known monthly fixed items include $12,000 rent, $2,500 EHR, and $3,000 malpractice The real test is cash runway during credentialing and early collections
About the author
Ava Mitchell
Business Plan Writer
Ava Mitchell is a business plan writer at Financial Models Lab who helps early-stage founders choose realistic business ideas with founder-friendly numbers. She explains startup planning in plain English, with a focus on operating expense planning and on breaking down revenue, expenses, and profit so founders can make practical real-world decisions.
Choosing a selection results in a full page refresh.