Implantable Loop Recorder Owner Income: $157M Year 1 Proxy
Implantable Loop Recorder Services
You’re modeling owner income from an implantable loop recorder service, not a cardiologist paycheck Using the supplied first-year assumptions, the service produces $2139M in annual revenue and $1573M in operating profit before personal taxes, debt service, and optional reserves These are planning assumptions for revenue, costs, staffing, and capacity they are not tax, legal, coding, clinical, or reimbursement advice
Owner income$1.57M to $14.06MNet margin75.1% to 82.1%Revenue for target pay$21.39M to $171.02MBusiness difficultyHard
Want to test your own ILR owner pay?
Owner income calculator
Estimate owner take-home from monthly revenue, gross margin, staffing, overhead, reserves, and a target pay goal.
!
Planning note This is a researched planning estimate, not guaranteed salary, tax advice, or owner distribution advice.
How do you check owner income in the Implantable Loop Recorder Services model?
What is the implantable loop recorder service profit margin?
The base-case Year 1 operating margin for Implantable Loop Recorder Services is 735%, based on $1,573M operating profit on $2,139M revenue. For the KPI side, see What Are The 5 KPIs For Implantable Loop Recorder Services Business? Direct cost pressure starts at 145% of revenue, with 120% implantable device procurement and 25% disposable surgical kits, while variable expenses add another 55%. Year 5 margin rises to 822% as combined direct and variable costs fall to 164%, but reimbursement, denials, clinical labor, billing capture, and software fees can move owner cash fast.
Margin math
735% Year 1 operating margin
$1,573M profit on $2,139M revenue
145% direct cost pressure
55% variable expense load
Cash swing factors
822% Year 5 margin
Combined costs fall to 164%
Billing capture and denials matter
No reimbursement guarantee or coding instruction
How many implantable loop recorder patients are needed to pay the owner?
Implantable Loop Recorder Services needs about 17 procedures per month to cover the $115,250 monthly overhead before owner pay. Here’s the quick math: with $8,632 weighted realized revenue per procedure and about $6,906 contribution per procedure, break-even is $115,250 ÷ $6,906. If you add owner pay, put that amount into the numerator; active remote-monitoring patients need a separate model because the supplied data does not include a monitored census.
Break-even
$39,000 fixed overhead
$76,250 wages monthly
Total overhead: $115,250
Break-even: about 17 procedures
Owner pay and cash
Add owner pay to numerator
Revenue per procedure: $8,632
Contribution per procedure: $6,906
Model remote-monitoring patients separately
How much can an implantable loop recorder service owner make?
Under the supplied base case, an How To Launch Implantable Loop Recorder Services Business? owner shows a Year 1 operating profit proxy of $1.573M on $2.139M revenue, before personal taxes, debt service, reserves, and reinvestment. That is not salary or a guaranteed distribution; owner cash depends on volume, monitoring census, reimbursement, device costs, staffing, billing capture, and the owner’s clinical or management role.
Base Case
$2.139M Year 1 revenue
$1.573M operating profit proxy
2,065 realized procedures per month
73.5% implied operating margin
Year 5 Upside
$17.102M projected revenue
$14.055M operating profit proxy
1,497 realized procedures per month
82.2% implied operating margin
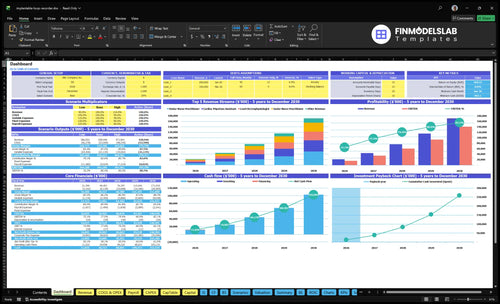
Implantable Loop Recorder Services Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Want to see the six ILR income drivers?
1
Procedure Volume
2,065/mo
At 2,065 realized procedures a month, volume is the main cash engine and it spreads fixed cost fast.
2
Payer Mix
$8K-$10.5K
Better reimbursement mix pushes more cases toward the top of the treatment price range and raises cash per case.
3
Staff Productivity
55%-85%
Higher capacity turns the year-1 $915K wage bill into more billable work and lifts take-home.
4
Device Costs
14.5%
Implant device procurement at 12.0% plus kits at 2.5% sets the direct-cost floor, so savings flow to EBITDA.
5
Billing Overhead
$468K/yr
Billing fees, monitoring data, and fixed overhead total about $468K a year, so weak collection hurts cash fast.
6
Active Monitors
High
More active monitored patients keep recurring fees coming in after the implant, which supports steadier income.
Implantable Loop Recorder Services Core Six Income Drivers
Monthly implantable loop recorder implants
Volume pays the bills
Monthly implant volume drives most revenue here, so utilization matters more than desk-level activity. With $39,000 in monthly fixed overhead and payroll, idle procedure time stays expensive fast. The model only works well once completed cases clear break-even, because every extra implant helps absorb fixed cost and improves operating leverage.
Year 1 capacity
Year 1 modeled activity is 2,065 realized procedures per month after capacity assumptions, based on 2 lead electrophysiologists, 3 senior nurse practitioners, 2 cardiac physician assistants, 2 junior nurse practitioners, and 1 clinical procedure specialist. That staffing mix sets the ceiling for how many referrals can become completed implants.
What lifts revenue
More appropriate referrals, stronger authorization success, better scheduling capacity, and more completed procedures all raise revenue. Here’s the quick math: if any one step slips, the implant never turns into cash. The risk is simple too: idle provider time leaves the fixed overhead and payroll uncovered.
Year 5 load
Year 5 activity reaches 1,497 procedures per month. What this estimate hides is the timing gap: if volume softens before that level, the business still carries the same $39,000 monthly fixed base, so owner take-home swings hard with throughput.
Active ILR monitored patients
Recurring cash
Active monitored patients matter because remote follow-up can steady cash after the implant sale. The supplied model already includes remote monitoring data fees at 10% of revenue, so the real question is how many patients stay active, how many transmissions come through, and whether billing captures that work cleanly.
Editable inputs
Keep active monitored patients, retention, transmission volume, and monitoring revenue editable. That lets you test how a bigger census changes monthly revenue without locking in a fake per-patient number. It also shows whether the workflow can support the load before you count on the cash.
Workflow limits
The main constraints are billing capture, patient retention, transmission workflow, technician workload, and clinical review time. A larger census can help revenue, but if any one of those breaks, you get denials, labor strain, and slower collections instead of cleaner margin.
Cash flow effect
If collections and staffing keep pace, the expected effect is smoother monthly revenue than implant-only income. If not, a bigger active census can raise labor cost and denial risk fast, so the model should test staffing per transmission and review capacity before assuming the monitoring book is all upside.
ILR payer mix and reimbursement
Payer mix drives take-home
When your payer mix shifts, owner income moves fast. Year 1 weighted realized revenue per procedure is about $8,632, based on $17.825M monthly revenue divided by 2,065 realized procedures. Stated prices run $8,000-$9,500 in Year 1 and $9,000-$10,500 by Year 5 across provider roles. This is a planning assumption, not coding advice.
Model the real cash flow
Build the model with payer mix, reimbursement per implant, authorization success, denials, collections, and payment timing. Here’s the quick math: even a small per-case change can move margin hard because revenue per procedure is the main driver of owner take-home. One clean number is not enough.
Watch approvals first
Track authorization success before you open slots. A lower approval rate cuts realized procedures, then hits both implant revenue and follow-on monitoring revenue. Use payer-specific approval rates and denial rates to forecast cash, not booked cases. If collections lag, staffing and device buys still happen on time.
Small swings, big margin
At $8,632 realized revenue per procedure, a few hundred dollars more or less per implant can shift monthly margin materially. That’s why reimbursement, denials, and payment timing need reserves baked in from day one, especially when payer mix leans toward slower-paying plans.
Implantable loop recorder device cost
Margin Squeeze
Device and sterile supply costs hit gross profit on every implant. In Year 1, direct costs are 145% of revenue: 120% for the implantable device and 25% for disposable surgical kits. That means the case loses money before fixed overhead is even counted, so price, volume, and purchasing terms matter immediately.
Cost Build
Estimate this cost as units × unit price for the device, plus disposable kits, shipping, and waste. Use vendor quotes, expected implant volume, and days of stock on hand. Keep it separate from payroll, rent, and owner pay so you can see true per-case margin.
Use current vendor quotes.
Track kits per implant.
Count unused stock fast.
Lower Waste
Protect margin with better purchasing terms, tighter inventory control, and less kit waste. By Year 5, direct costs fall to 117% of revenue, with 100% device and 17% kits. Small savings move gross margin fast, but price increases or stale inventory can hit cash before reimbursement arrives.
Cash Risk
Model the implant cost separately from fixed overhead, payroll, and owner compensation. The effect is an immediate gross margin change, so a higher device price shows up right away in case economics, while unused inventory drains working capital before the related revenue is collected.
Implantable loop recorder staffing costs
Labor load
Owner take-home here is mostly a staffing story. The listed team adds up to about $5.64M in annual wages: $280,000 for the medical director, 20 lead cardiac technicians at $95,000 each, 20 clinical liaison roles at $85,000, 20 patient care coordinators at $60,000, $110,000 for operations, and 5 compliance officers at $90,000 each.
What it covers
This cost covers clinical labor, referral support, patient coordination, and compliance work tied to implantation and remote monitoring. Estimate it as headcount × salary, then add months of coverage and onboarding lag. In this case, the big inputs are 20 technicians, 20 liaison roles, 20 coordinators, and 5 compliance staff.
How to control it
Keep payroll tied to proven volume, not hopes. The fast mistake is adding sales headcount before referrals and monitoring census are stable; the other mistake is under-staffing monitoring, which hurts service quality. Early on, the owner should do more of the clinical work, then add hired labor only when case flow can carry it.
Scale after proof
The income impact is medium to high because owner take-home swings with hired labor versus owner-performed work. The risk rises fast if onboarding is slow, sales payroll outruns volume, or monitoring coverage falls behind. The strongest margin setup is simple: prove volume first, then staff the service around it.
ILR billing capture and service overhead
Billing drag
Year 1 cash is tight when 45% of revenue goes to medical billing and RCM, plus 10% to remote monitoring data fees. That means more than half of top line is gone before fixed overhead, so claims, collections, and authorization work decide whether billed revenue becomes usable cash.
Monthly base
The fixed overhead base is $39,000 per month. It includes $15,000 facility lease ASC access, $8,500 malpractice insurance, $3,200 HIPAA compliant software license, $5,000 administrative office rent, $4,500 professional marketing services, and $2,800 IT security and support.
$39,000 monthly run rate
Use one-month quotes
Multiply by 12 for Year 1
Control the burn
Keep costs tight by delaying extra office space, software add-ons, and marketing spend until billing is stable. The common mistake is scaling remote monitoring before collections are clean. If authorization gaps or denials slow cash, fixed costs hit harder because they do not flex with volume.
Cash risks
The main financial pressure points are authorization gaps, denials, delayed collections, software costs, and compliance workload. Those issues slow cash conversion, so owner take-home depends on how fast revenue gets collected, not just how much gets billed.
Implantable Loop Recorder Services Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Compare low, base, and high ILR owner-income scenarios
Owner income scenarios
Owner income moves with procedure volume, collections, device cost, staffing, and overhead. The model's Year 1 base case is strong, but ramp timing still matters.
Low, base, and high owner income cases for implantable loop recorder services.
Scenario
Low CaseRamp risk
Base CaseBase plan
High CaseScale case
Launch model
Owner income stays under pressure if volume starts slow and collections run below plan.
Owner income tracks the model's expected operating run rate with steady procedure flow and solid margins.
Owner income climbs when capacity, reimbursement, billing capture, and purchasing terms all improve.
Typical setup
Fewer implant and monitoring procedures, softer payer mix, higher device and billing costs, and more reserve pressure keep cash flow tight.
Year 1 revenue of $21.39 million, about 2,065 realized procedures per month, 20.0% combined direct and variable costs, $915,000 wages, and $468,000 fixed overhead support a strong profit base.
Higher procedure throughput, stronger collections, better payer mix, lower device costs, and leaner overhead push margins above the base case.
Cost drivers
Lower implant volume
weaker collections
higher device cost
slower billing capture
heavier staffing
Planned procedure volume
modeled reimbursement
steady payer mix
controlled staffing
stable overhead
Higher capacity use
better reimbursement
stronger billing capture
lower device cost
leaner overhead
Owner income rangeBefore owner reserves
$8,000,000 - $12,000,000Downside band
$14,000,000 - $16,500,000Expected band
$18,000,000 - $24,000,000Upside band
Best fit
Use this to stress-test a slow ramp, tighter reimbursement, and higher-than-planned operating drag.
Use this as the core operating case for budgeting, hiring, and cash planning.
Use this to test upside from tighter operations and better contract terms once the service line is scaled.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
The supplied model shows $1573M in Year 1 operating profit before personal taxes, debt service, reserves, and reinvestment That comes from $2139M in revenue, 200% combined direct and variable costs, $915,000 in wages, and $468,000 in fixed overhead Actual distributions depend on collections, payer mix, and reserve policy
Using Year 1 assumptions, break-even before owner pay is about 17 procedures per month The math is $115,250 in monthly payroll and fixed overhead divided by about $6,906 contribution per procedure The model’s Year 1 realized capacity is 2065 procedures per month, but that assumes referrals, authorization, staffing, and billing all work
You don’t need one in the model, but an existing cardiology practice can lower risk by sharing referrals, rent, staff, and admin systems A standalone service carries $468,000 in annual fixed overhead before payroll It also needs enough volume to cover facility access, malpractice, software, marketing, IT support, and patient coordination
The biggest drivers are implant volume, monitored patient census, reimbursement, device cost, staffing, and billing capture In Year 1, direct costs are 145% of revenue and billing plus monitoring data fees add 55% A small change in collections or device procurement can move owner cash because revenue is modeled at $2139M
Start with operating profit, then subtract reserves, debt service, reinvestment, and personal taxes outside the business model Don’t treat the full $1573M Year 1 operating profit as automatic take-home Build a target-pay case, a reserve case, and a lower-collections case so distributions don’t starve inventory, staffing, or monitoring operations
About the author
Kevin West
Startup Cost Researcher
Kevin West is a startup cost researcher at Financial Models Lab who writes practical guides for people planning their first business. He focuses on break-even planning and on comparing business ideas by cost and effort, with an emphasis on realistic small business planning for founders with limited capital. His work connects business ideas to realistic startup budgets.
Choosing a selection results in a full page refresh.