Open an Implantable Loop Recorder Service in 3–6 Months
You’re opening a cardiology service that needs clinical leadership, procedure access, device supply, remote monitoring, billing, and referrals ready before the first patient The launch plan uses a 5-year model period, with Year 1 planning assumptions of 10 clinical providers, $39,000 in monthly fixed overhead before wages, and staged validation before go-live
Time to Open6 monthsSetup windowLaunch Sequence8 stagesCompliance firstKey BottleneckPayer gateApproval pathFirst Revenue StepFirst implantMonitor enrolled
Launch timeline
Short web summary of the launch plan; the XLSX export holds the detailed Gantt Chart.
How long does it take to open an implantable loop recorder service?
For Implantable Loop Recorder Services, a practical launch takes 3–6 months. The usual drag comes from clinical leadership work, payer credentialing, facility access, vendor contracting, remote monitoring setup, staff training, billing tests, and referral activation. If payer enrollment or physician credentialing stalls, go-live slips; don’t start the first operating month until inventory, consent forms, charge capture, and follow-up scheduling are tested.
Launch blockers
Payer enrollment can delay go-live
Physician credentialing can slow access
EHR integration can delay alerts
Remote monitoring needs setup and testing
What must be ready
Device inventory must be in place
Consent forms must be tested
Charge capture must work cleanly
Model capacity from 10 to 43 providers
What do you need to start an implantable loop recorder service?
To start Implantable Loop Recorder Services, get legal and clinical readiness in place before marketing: licensed cardiology or electrophysiology leadership, medical director coverage, protocols, consent, payer enrollment, malpractice insurance, and tested monitoring workflows; this How To Launch Implantable Loop Recorder Services Business? guide fits that setup path. Don’t accept patients until remote monitoring, escalation rules, billing, and referral intake are tested end to end.
Clinical must-haves
Licensed cardiology or electrophysiology leadership
How do you get first patients for an implantable loop recorder service?
Start with the referral sources that already see rhythm-diagnosis need: cardiologists, electrophysiologists, primary care, neurology, stroke clinics, hospitals, and discharge follow-up paths. If you want the pipeline to move, build provider education around eligibility, intake steps, scheduling speed, monitoring follow-up, and report turnaround, and track the right handoff points with What Are The 5 KPIs For Implantable Loop Recorder Services Business?
Open referral channels
Target cardiology and electrophysiology first
Include primary care and neurology
Work stroke clinics and hospitals
Use discharge follow-up pathways
Make referrals convert
Explain eligibility and intake clearly
Speed up scheduling and follow-up
Assign 20 FTE Clinical Liaison Sales in Year 1
Watch referral-to-consult and implant-to-monitoring
First revenue comes from the scheduled implantation and the monitoring enrollment, so the first win is not volume alone, it’s clean handoffs. If intake scripts are unclear, referrals stall before the first case.
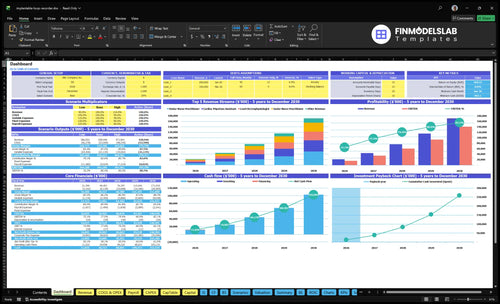
Implantable Loop Recorder Services Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm the ILR clinic is ready before accepting patients
Launch readiness checklist
Use this go-live approval checklist before opening implantable loop recorder services.
1Clinical
Physician licensing verifiedCritical
The implanting physician must be licensed before any procedure work starts.
Electrophysiology oversight boundHigh
Oversight must be in place so rhythm cases have clear clinical signoff.
Malpractice policy activeCritical
Model assumes $8,500 monthly malpractice cost, so coverage has to be active at launch.
2Site
ASC access contractedCritical
The model assumes $15,000 per month for procedure-room access.
Procedure room workflow clearedHigh
Room flow must fit implant steps, turnover, and monitoring handoff.
Sterile supply path readyHigh
Sterile kits have to arrive and restock cleanly before the first implant.
3Devices
Device vendor signedCritical
Device supply gaps would stop implants and remote follow-up.
Initial inventory on handCritical
Stock must cover the launch month so cases do not slip.
Monitoring alerts activeHigh
Remote monitoring has to send alerts and failures before go-live.
4Billing
HIPAA software activeCritical
The model carries a $3,200 monthly license, so access must be live.
CPT codes mappedHigh
Code setup must match implant and monitoring claims before billing starts.
Payer enrollment completeCritical
Claims cannot cash flow if payer enrollment is still pending.
5Team
Consent training completeHigh
Staff must know consent steps before they touch a patient.
Sterile workflow practicedHigh
Practice reduces delays and keeps the first procedure room safe.
Documentation workflow practicedHigh
Documentation must support claims, alerts, and follow-up notes.
Alert triage drills passedHigh
Triage rules need to route urgent rhythm alerts without delay.
6Go-live
Referral intake testedCritical
Referrals are the first revenue step, so intake must work end to end.
Scheduling flow liveHigh
Patients need a clean path from referral to procedure slot.
Escalation pathway setHigh
Escalation rules must route urgent alerts before launch.
Launch cash coveredCritical
The model shows $903k minimum cash in Month 1, so launch needs that buffer.
Go-live signoff completeCritical
Final signoff should confirm compliance, billing, staff, and supply readiness.
Which six drivers decide launch readiness?
1Clinical Leadership
10 providers
A licensed lead and written protocols keep the 10-provider team safe and aligned.
2Procedure Room Readiness
3-6 mo
Confirmed room access starts the $39K monthly fixed burn, so empty slots get expensive fast.
3Device Vendor Setup
120% rev
Vendor supply and lot tracking cut implant delays and protect gross margin on early cases.
4Remote Monitoring
200% var
Tested alerts and owner review keep monitoring from becoming the top bottleneck.
5Payer Billing
45% rev
Credentialing and clean claims decide whether first procedures become cash or denials.
6Referral Intake
207 slots
Referrals and intake rules fill the 207 monthly slots and keep utilization from stalling.
Clinical Leadership and Protocols
Clinical Governance First
Clinical governance is the first launch gate for implantable loop recorder services. You need a licensed cardiology or electrophysiology lead with written rules before the first case, or you can open with procedures ready but no physician-led monitoring standards. That raises risk in patient selection, consent, orders, and escalation. The modeled Medical Director load is 10 FTE and $280,000 a year, about $23,333 per month.
The launch work here is not just approval. It includes patient selection criteria, consent language, procedure orders, complication response, alert escalation, report review, and follow-up standards. One clear rule set makes first cases safer and the notes cleaner, which matters for billing, handoffs, and referral trust. Without that, day-one work becomes reactive and the team spends time fixing gaps instead of serving patients.
Write the Protocols Before Scheduling
Before booking patients, verify that the physician lead has signed off on the full workflow and that staff know who owns each step. The minimum set is simple: screen the right patients, get consent right, write the procedure order, define what counts as an alert, and set who reviews reports and follow-up. That keeps the first cases on track.
Here’s the quick check: if any one of these is missing, the launch is not really ready.
Patient selection rules
Consent and order templates
Complication response steps
Alert escalation ownership
Report review timing
Follow-up standards
1
Procedure Room Readiness
Procedure Room Readiness
No room means no implant, so this is the hard gate for opening on time. Readiness means confirmed procedure room or ASC access, with sterile supplies, disposable kits, infection control, documentation, recovery steps, and emergency response all set before the first patient is booked.
The modeled room cost is $15,000 per month, so delays here hit cash and launch timing fast. If trained clinical staff or device supply is missing, same-day flow breaks and early cases get canceled. One clean room workflow matters more than a full schedule on paper.
Test the room flow first
Before opening, run one full walk-through from check-in to discharge. Confirm who opens kits, who documents, who watches recovery, and who handles emergency steps. Same-day patient flow should be clear before you schedule the first procedure.
Verify sterile supplies and disposable kits.
Confirm trained staff coverage.
Match device delivery to booked cases.
Set recovery and discharge steps.
Test documentation before day one.
The launch risk is simple: if you book patients before the room workflow is tested, you can’t implant reliably and cancellations rise. A ready room gives predictable first-day throughput and fewer avoidable delays.
2
Device Vendor and Inventory Setup
Device Vendor and Inventory Setup
Opening on time depends on having devices in hand before the first referral lands. For implantable loop recorder services, the readiness signal is a signed vendor agreement, launch inventory, rep training, and a working replenishment process, because no implant can be booked if supply is not cleared and tracked.
The Year 1 model assumes implantable device procurement at 120% of revenue and disposable surgical kits at 25%. That makes supply terms a cash and margin issue, not just a logistics task. Missed lot tracking, weak storage controls, or no replacement rule can push cases out, raise cancellation risk, and weaken gross margin control.
Lock supply before you open
Start with the vendor agreement, consignment review, and launch stock count. Then test the full chain: ordering, receiving, lot tracking, storage, and same-day device release. If the device tracker is not live, you do not have launch-ready inventory.
Assign one owner for replenishment and one backup for shortages. Confirm launch-day availability for the first booked cases, and set replacement rules in writing so a damaged or missing unit does not stall the schedule. One clean line: if the device is not on the shelf, the patient does not get imaged.
Verify signed vendor terms.
Count launch inventory.
Train reps on ordering rules.
Document lot and serial tracking.
Set storage and replacement controls.
3
Remote Monitoring Operations
Remote Monitoring Operations
Remote monitoring is the service, not a back-office add-on. You can’t open on time if enrolled patients, tested transmissions, alert triage, provider review, patient communication, documentation, and follow-up scheduling are not working before the first implant.
Here’s the key risk: implants can start before there is reliable alert ownership. That creates missed events, delayed follow-up, and weak clinical trust on day one. The Year 1 model carries $3,200 per month for HIPAA-compliant software and 10% of revenue for remote monitoring data fees, with 20 FTE trained cardiac technicians needed to keep the flow moving.
Launch-Ready Monitoring Setup
Test the full loop before opening: enrollment, transmission checks, alert routing, physician review, patient outreach, charting, and follow-up booking. If any step is manual or unclear, first-day volume will pile up fast and the team will miss billable follow-up.
Build the work in this order: enroll the patient, confirm data reaches the platform, assign alert ownership, document the review path, and schedule the next touchpoint. One clean workflow beats a busy but unowned queue.
Verify alert ownership before first implant.
Train 20 FTE technicians on triage rules.
Budget $3,200 monthly for compliant software.
Track data fees at 10% of revenue.
Test follow-up scheduling before launch day.
4
Payer Credentialing and Billing Workflow
Billing Readiness
For implantable loop recorder services, the first case only turns into cash if payer enrollment, credentialed physicians, and prior authorization are active before the procedure. If you open with cases scheduled but billing setup still pending, you can do the work and still wait on payment. That pushes first-month revenue out and raises denial risk.
This workflow also needs CPT code setup, charge capture, documentation standards, claims review, and denial tracking. The Year 1 model assumes medical billing and revenue cycle management fees at 45% of revenue, so weak billing control hits margin fast. Completed clinical notes and monitoring records are not optional; they are the proof that supports the claim.
Credential Before First Cases
Before opening, verify each payer file, each physician credential, and each authorization step in the exact order claims will flow. Test one clean case from order to charge to claim to payment, then fix gaps in documentation and coding before volume starts. If approvals are missing, don’t start procedures just to “see what happens.”
Confirm active payer enrollment.
Map each CPT code.
Assign claim review ownership.
Track denials from day one.
Require complete notes before billing.
No active approval means no clean first claim. The main bottleneck is doing cases before the payer file is live, because that creates avoidable denials and slows cash when the clinic is trying to prove day-one readiness.
5
Referral Pipeline and Patient Intake
Referral Readiness
Opening on time is only half the job if no patients are lined up. Active referral relationships with cardiology, electrophysiology, primary care, neurology, stroke clinics, hospitals, and discharge teams are what turn a ready clinic into a working one. If this pipeline is weak, you can have staff, room time, and equipment in place but still start with zero qualified patients.
The launch work includes provider education, intake scripts, eligibility screening, scheduling rules, insurance checks, and post-referral feedback. The Year 1 plan assumes 20 FTE in Clinical Liaison Sales and $4,500 per month for professional marketing services, so referral setup is a core operating input, not a soft add-on.
Map Day-One Referral Flow
Before opening, confirm who can send patients, who screens them, and who books them. Write the handoff rules for each source, then test them with a dry run so a referral can move from provider to scheduled visit without delays, missing insurance checks, or unclear eligibility.
Use one intake path for every source so staff do not improvise. One clean process is what protects first implants, because a ready clinic with no intake discipline will still run below capacity and miss early revenue.
Start with licensed cardiology or electrophysiology leadership, then build the procedure room, device supply, remote monitoring workflow, payer setup, and referrals The researched launch window is commonly 3–6 months The Year 1 model assumes 10 clinical providers and about 207 monthly treatment slots, so validate demand before scaling
Plan on 3–6 months before opening to patients The slowest items are usually payer credentialing, physician setup, vendor contracting, remote monitoring workflow, and referral activation The model runs over 5 years, but opening month should focus on safe first implants, clean documentation, and follow-up monitoring
The model includes Facility Lease ASC Access at $15,000 per month, so procedure access is a core launch assumption Whether the service uses an ambulatory surgery center, office procedure room, or hospital pathway depends on clinical leadership and payer requirements Do not schedule implants until room workflow, supplies, and emergency procedures are ready
Common delays include incomplete payer enrollment, missing device inventory, untested monitoring software, unclear alert triage, and weak documentation rules The model includes HIPAA-compliant software at $3,200 per month and remote monitoring data fees at 10% of revenue If onboarding takes longer than expected, first revenue can slip
The first billable step is a scheduled ILR implantation with proper documentation and enrollment into follow-up remote monitoring Year 1 treatment prices in the model range from $8,000 to $9,500, depending on provider type Cash collection still depends on payer approvals, charge capture, and claims review
About the author
Daniel Brooks
Practical Business Analyst
Daniel Brooks is a practical business analyst at Financial Models Lab, where he writes about small business budgeting and estimating what a new business can realistically earn. He creates clear, beginner-friendly content for people planning to open a physical location, with a focus on realistic assumptions, break-even explanations, and what it really takes to get a business off the ground.
Choosing a selection results in a full page refresh.