IV Ketamine Therapy Clinic Owner Income: $215M Revenue Model
IV Ketamine Therapy Clinic Bundle
Key Takeaways
Volume drives revenue, so chair utilization matters most.
Collected revenue per treatment shapes cash more than price.
Fixed overhead stays high, so reserves protect distributions.
Staffing and retention protect capacity and income.
Owner income$34kNet margin2.6%Revenue for target pay$1.33MBusiness difficultyHard
Want to test your owner draw?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay for an IV ketamine therapy clinic.
!
Planning note: This is a researched planning estimate only, not guaranteed salary, tax advice, or owner distribution advice.
Want the full IV Ketamine Therapy Clinic model?
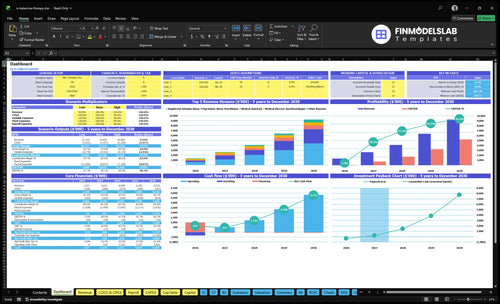
The IV Ketamine Therapy Clinic Financial Model Template shows dashboard, assumptions, revenue, staffing, expenses, break-even, cash flow, and owner pay; treatments run 400 to 470, revenue $44,750 to $52,255, fixed overhead is $19,000.
Model highlights
Owner draw timing
Revenue sensitivity charts
Debt and reserves
How many ketamine infusions per month to make money?
For an IV Ketamine Therapy Clinic, the listed scenario break-even is about 162 infusions per month, based on $57,750 in fixed overhead plus Medical Director and Nurse Practitioner payroll and about $358 contribution per treatment. Here’s the quick math: $57,750 ÷ $358 ≈ 162. This is a scenario break-even, not a universal claim. If you want profit, add owner draw, debt service, reserves, and any missing clinical payroll to the numerator.
Break-even math
$57,750 fixed monthly costs
$358 contribution per infusion
162 infusions to break even
Use $57,750 ÷ $358
Profit check
Add owner draw to costs
Add debt service too
Add reserves if needed
Add missing clinical payroll
How much profit does an IV ketamine clinic make?
An IV Ketamine Therapy Clinic can show about $85,450 in monthly operating profit, or roughly $1.03M annually, before owner pay. Here’s the quick math from How Much To Start An IV Ketamine Therapy Clinic Business?: $179,000 monthly collected revenue minus 20.0% variable costs, $19,000 fixed overhead, and $38,750 Medical Director/Nurse Practitioner payroll.
Profit bridge
$179,000 monthly collected revenue
$35,800 variable costs at 20.0%
$143,200 monthly contribution
$85,450 operating profit before owner pay
Take-home caveats
$2.15M annual collected revenue
$1.03M annual operating profit
RN and medical assistant wages reduce cash
Taxes, debt, reserves, and reinvestment reduce distributions
Does the owner need to be a physician for a ketamine clinic?
No, not always. For an IV Ketamine Therapy Clinic, the owner does not have to be a physician in every state, but the structure must match state ownership, supervision, and prescribing rules, plus corporate practice of medicine limits. If the owner provides licensed services, owner income can rise with billable clinical work; if not, income comes from hiring clinicians and running the business. With staffing rising from 1 to 4 Psychiatric Nurse Practitioners, 2 to 6 Registered Infusion Nurses, 1 to 3 Clinical Psychologists, and 1 to 3 Medical Assistants, legal and compliance review matters before you scale.
Ownership rule
State-specific rules control ownership.
Physician owner is not always required.
Supervision rules can limit control.
Medical Director: 1 anesthesiologist at $320,000.
Income and staffing
Licensed owner can earn more directly.
Non-physician owner depends on hired clinicians.
Clinical team expands as volume grows.
Legal review comes first, before hiring.
IV Ketamine Therapy Clinic Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
What really moves owner take-home?
1
Treatment Volume
400-470/mo
This is the core revenue engine: the model starts at 400 treatments a month in year 1 and reaches 470 in the mature year, so small gains in starts and repeats lift owner income fast.
2
Collected Revenue
$44.8K-$52.3K
The model's monthly collected revenue rises from $44,750 in year 1 to $52,255 in the mature year, so pricing and payer mix drive owner take-home.
3
Labor Load
200%-152%
The mix of clinician hours controls labor burn, and the model's variable cost load moves from 200% to 152% as staffing gets more efficient.
4
Retention
60-70/mo
The psychologist line grows from 60 to 70 treatments a month, which is a clean proxy for maintenance retention and repeat cash.
5
Chair Use
40%-85%
Capacity rises from 40% to 85% across roles, so fuller schedules turn the same room time into more billable visits.
6
Overhead
$19K/mo
Fixed overhead is about $19,000 a month, and the clinic also needs reserve cash, so profit is not fully distributable even after breakeven in month 2.
IV Ketamine Therapy Clinic Core Six Income Drivers
Monthly Treatment Volume
Monthly Treatment Volume
Monthly treatment volume is the first income lever because revenue starts with billable visits. In the model, 400 treatments per month supports about $179,000 in monthly revenue, and 470 treatments supports about $245,600. More visits lift gross profit, but only if staffing, room time, and recovery flow keep each session safe and on schedule.
The visit base comes from induction starts, repeat maintenance visits, and chronic pain protocols. First-year capacity is modeled at 400%-500%, and mature-year capacity at 800%-850%, so volume has to match clinician coverage, infusion time, and turnover. If chairs are filled before workflow is safe, payroll and overhead rise before cash does.
Track Volume Before You Add Staff
Track scheduled starts, completed treatments, cancellations, and repeat visits each week. The clean test is treatments per staffed hour and treatments per chair day, because those show whether demand or workflow is limiting cash flow. Use collected revenue per treatment, not posted price, when you forecast owner pay.
Watch treatment count by protocol.
Match staffing to booked demand.
Protect recovery and turnover time.
Measure cancellations against rebook rate.
Do not add a clinician just to chase a forecast. Add capacity only when booked volume is steady enough to cover payroll and the $19,000 monthly overhead base. That keeps more revenue available for taxes, reserves, and owner draw instead of leaking into idle labor.
1
Average Collected Revenue Per Treatment
Collected Revenue Per Treatment
Collected revenue per treatment is what the clinic actually keeps per infusion, not the posted price. In year one, the model implies $447.50 per treatment from $179,000 monthly revenue over 400 treatments. In the mature year, it rises to about $522.55 from $245,600 over 470 treatments.
This driver matters because most overhead is already locked in at $19,000 a month. A small collection change moves owner pay fast: at 400 treatments, every $25 change in collected revenue per treatment shifts monthly revenue by about $10,000. Price, session length, indication mix, discounts, payment plans, and cash-pay versus payer mix all feed this number.
Measure Net Collections, Not Sticker Price
Track net collections per completed treatment by market, protocol, and payment type. Here’s the quick math: monthly collected revenue ÷ treatments delivered. If that number slips, owner profit drops even when chair count holds. One clean rule: watch collections, not posted price, because posted price can hide discounts and slow-pay accounts.
Use a simple split by cash-pay, payment plan, and any payer source, then compare it with session length and indication mix. If follow-up billing drifts or discounts widen, the clinic may still be busy but less profitable. Since fixed overhead stays the same, protecting collection per treatment is one of the fastest ways to protect take-home income.
Formula: revenue divided by treatments
Track: discounts and payment plans
Watch: cash-pay mix by month
Flag: any collection decline fast
2
Maintenance Retention
Maintenance Retention
When clinically appropriate, maintenance visits turn a one-time treatment series into repeat revenue. Moving from 400 to 470 monthly visits adds 70 treatments, or about 17.5%, which helps smooth cash flow, keep chairs full, and spread fixed costs like the $19,000 monthly overhead across more billable visits.
The risk is simple: if follow-up cadence weakens, the clinic loses recurring visits and must replace them with new-patient marketing. That usually costs more and makes owner income choppier, because revenue depends more on fresh leads and less on planned repeat care.
Track Return Visits Early
Measure how many patients come back for a clinically appropriate follow-up series, and do it by cohort. Here’s the quick math: 70 extra monthly visits at the same collected revenue per treatment raise revenue before adding much new overhead, so retention matters most when the schedule is already near capacity.
Track 30, 60, 90-day returns
Separate maintenance from new starts
Watch no-shows and canceled follow-ups
Document follow-up timing in the chart
If retention slips, forecast fewer repeat visits and more marketing spend to refill the calendar. If it holds, you get steadier chair use and a more predictable owner draw.
3
Clinical Staffing Model
Clinical Staffing Mix
Staffing changes owner income fast because this model carries a $320,000 Medical Director and Nurse Practitioners at $145,000 each. First-year Medical Director/NP payroll is $38,750 per month, before nurses, psychologists, and medical assistants. Hired clinical coverage lowers owner workload, but it also cuts distributable profit.
Here’s the quick math: every added clinician must be covered by enough treatments and collected revenue to leave money for owner draw. If the owner covers more clinical work, cash flow can improve, but licensing limits, role strain, and burnout risk rise fast.
Track Payroll Per Treatment
Measure clinical payroll per treatment and payroll as a share of collected revenue. Start with the model’s $38,750 monthly Medical Director/NP payroll, then add each new hire only when volume and chair use can support it. If staffing grows ahead of visits, owner pay gets squeezed even when revenue looks better.
Watch payroll per treatment monthly
Match hires to booked volume
Separate owner labor from salary
Stress-test draw after each hire
Test two paths: more hired coverage or more owner-delivered care. Hired coverage reduces owner time, but it locks in fixed cost; owner care can lift near-term cash flow, but it adds role conflict and fatigue. Keep the staffing plan tied to treatments per month, not headcount alone.
4
Chair Utilization
Chair Utilization
Chair use turns demand into billable treatments. In this model, capacity assumptions start at 400%-500% in year one and rise to 800%-850% in the mature year, so the real question is not how full the room looks, but how many safe, billable infusions it can support.
Here’s the quick math: each idle chair still sits under $19,000 in monthly fixed overhead. If infusion time, recovery monitoring, cancellations, room turnover, or clinician coverage are off, owner pay drops fast because revenue stays flat while the same rent and insurance keep hitting cash flow.
Track Safe Density
Measure chair use against the real inputs: scheduled treatments, infusion time, recovery time, cancellations, turnover, and clinician coverage. The goal is safe density, not max throughput, because a packed schedule without staff coverage can create delays, lost visits, and weaker collections.
Track booked vs available chair time.
Watch cancellations and turnover gaps.
Forecast against $19,000 fixed overhead.
If utilization slips, the same fixed base has to be spread across fewer billable treatments, which cuts gross margin and the cash left for owner draw. Tight room flow helps more than adding more rooms too early.
5
Fixed Overhead And Reserves
Fixed Overhead Cuts Distributions
$19,000 of monthly overhead must be paid before the owner can take home more cash. The biggest line is the $12,000 clinic lease, or about 63% of fixed overhead, followed by $3,500 malpractice insurance and smaller items like software, utilities, property coverage, supplies, and training. If revenue softens, this cost base stays put, so owner pay drops fast.
Here’s the quick math: fixed costs are about 32% of a $59,000 month, or about 8% of a $245,600 month. That gap matters because net profit is not the same as spendable cash. Debt service, reserves, working capital, and reinvestment come off the top too, so profit can look healthy while owner distributions stay tight.
Protect Cash Beyond Profit
Track fixed overhead as a share of monthly collected revenue, then stress-test it against slower volume. One clean rule: keep a separate cash plan for reserves, working capital, and reinvestment so you do not overdraw the business. If collections slip, the lease and insurance still hit the bank account.
Build a monthly cash forecast that shows overhead, debt service, and owner draw side by side. Watch the lease, malpractice premium, and staffing-related admin costs first, since they drive most of the fixed load. If overhead rises faster than collections, owner income shrinks even when the clinic is profitable on paper.
6
IV Ketamine Therapy Clinic Business Plan
30+ Business Plan Pages
Investor/Bank Ready
Pre-Written Business Plan
Customizable in Minutes
Immediate Access
Compare low, base, and high owner-income cases
Owner income scenarios
Owner income rises as treatment volume and collected revenue scale, but staffing, supplies, and fixed clinic overhead cut into take-home. These cases show how fast the clinic can support the owner.
Low, base, and high cases for planning owner take-home.
Scenario
Low CaseLow Case
Base CaseBase Case
High CaseHigh Case
Launch model
Uses the first-year operating run rate and the weakest modeled take-home path.
Uses Year 3 volume and pricing with a steadier mid-cycle take-home path.
Uses mature-year volume and pricing with the strongest modeled take-home path.
Typical setup
About 400 monthly treatments at about $447.50 average collected revenue per treatment, or about $179,000 monthly revenue, with about 20.0% variable costs and $19,000 fixed overhead before unprovided wages, reserves, taxes, and debt.
About 435 monthly treatments at about $484.88 average collected revenue per treatment, or about $210,975 monthly revenue, with about 17.1% variable costs and the listed staffing base before unprovided wages, reserves, taxes, and debt.
About 470 monthly treatments at about $522.55 average collected revenue per treatment, or about $245,600 monthly revenue, with about 15.2% variable costs and fuller capacity before unprovided wages, reserves, taxes, and debt.
Cost drivers
400 monthly treatments
$447.50 collected average
20.0% variable costs
$19k fixed overhead
full clinical payroll
435 monthly treatments
$484.88 collected average
17.1% variable costs
mid-cycle staffing
stronger capacity use
470 monthly treatments
$522.55 collected average
15.2% variable costs
fuller capacity
mature staffing mix
Owner income rangeBefore owner reserves
$34kLow case
$1.7MBase case
$5.2MHigh case
Best fit
Use this to stress-test a slow start, weaker referral flow, or a softer payer mix.
Use this as the main planning case for a clinic running near the Year 3 model.
Use this to test upside if the clinic reaches mature volume and holds unit costs down.
!
Planning note: Scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. Unprovided clinical wages, reserves, taxes, and debt will reduce take-home.
The provided model supports a first-year operating profit ceiling of about $103M before owner compensation, taxes, debt, reserves, reinvestment, and unprovided staff wages That comes from $215M annual revenue, 200% variable costs, $228,000 fixed overhead, and $465,000 listed Medical Director/Nurse Practitioner payroll Actual owner take-home is lower
The data supports a volume test, not a date Using first-year assumptions, break-even on listed costs is about 162 treatments per month The math is $57,750 in monthly fixed overhead plus listed Medical Director/Nurse Practitioner payroll divided by about $358 contribution per treatment Missing staff wages and debt raise that target
Not always, but the answer depends on state law and the operating structure The model includes one Medical Director Anesthesiologist at $320,000 per year and growing licensed clinical staff Non-physician ownership, supervision, prescribing, and corporate practice rules need legal and compliance review before you assume owner distributions
Treatment volume, collected revenue per visit, and staffing drive most of the result The first-year model uses 400 monthly treatments, $44750 average collected revenue, and 400%-500% capacity use Mature-year assumptions reach 470 monthly treatments and about $52255 per treatment, but payroll, reserves, and debt still control distributions
Protect distributions by separating profit from cash Keep reserves for payroll, malpractice coverage, medical supplies, software, marketing, and debt service before taking draws In the model, fixed overhead is $19,000 per month and variable costs start at 200% of revenue, so thin cash planning can turn strong revenue into weak take-home
About the author
Emma Blake
Entrepreneurship Researcher
Emma Blake is an entrepreneurship researcher at Financial Models Lab who focuses on expense and revenue planning for people opening a new small business. She helps founders with limited capital turn big business questions into clear, practical planning steps, with a special focus on first-year business planning. Emma’s work connects business ideas with realistic startup budgets, making it easier to plan with confidence from day one.
Choosing a selection results in a full page refresh.