How Much Do Ophthalmology Clinic Owners Make? A $39M Case
An ophthalmology clinic owner may earn strong take-home income, but the supplied data supports collections and contribution profit, not a guaranteed paycheck In the researched case, annual clinic collections rise from $392M in the first year to $2926M in the mature year Listed supplies, pharmaceuticals, insurance processing, and marketing total 190% of revenue in the first year and 155% in the mature year, leaving $317M to $2472M before provider payroll, rent, equipment financing, admin costs, reserves, taxes, and owner pay
Owner income$1.33M to $19.88MNet margin34% to 68%Revenue for target pay$3.92MBusiness difficultyHard
Want the six income drivers?
1
Provider Utilization
65%-90%
Moving each clinician from 65% to 90% capacity raises visits and procedures without a like-for-like jump in fixed cost, so owner take-home scales fast.
2
Revenue Mix
$4.8M-$32.5M
Annual collections run from about $4.8M in Year 1 to $32.5M in Year 5, and the surgery-heavy mix is what creates that step-up.
3
Margin Control
81%-84.5%
Direct costs sit near 15.5% to 19.0%, so tighter supply and injection spend turns more collected revenue into EBITDA.
4
Staffing Load
9.5-31 FTE
Payroll expands from 9.5 FTE to 31 FTE, so cross-training and smart scheduling matter as much as more volume.
5
Fixed Overhead
$42K/mo
Fixed overhead is about $42K a month, so every open slot has to cover rent, insurance, and software before the owner sees cash.
6
Cash Runway
-$832K
The model bottoms at negative $832K in Month 6, so reserve funding protects take-home during the buildout.
Want to test your clinic owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
!
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to see the income model for an Ophthalmology Clinic?
How does owner role change ophthalmology clinic take-home income?
In an Ophthalmology Clinic, the owner usually keeps the most take-home income when they also produce clinical revenue, because that cash comes in without paying another doctor. But that setup ties the owner’s time to patient care and management, while a management-supported practice can scale collections and still needs more payroll and tighter supervision. In the supplied model, the practice grows from 6 providers in year 1 to 20 providers in the mature year, so absentee ownership is hard and succession risk rises if one doctor drives most collections.
Owner-led income
More take-home if owner sees patients
Less payroll, more direct margin
Time limit comes from clinic load
Management still needs the owner
Scaled ownership risk
6 to 20 providers changes payroll
Collections can grow with support staff
Supervision gets harder fast
One doctor creates succession risk
How much revenue does an ophthalmology clinic need to pay the owner?
You can’t pin down one revenue number for an Ophthalmology Clinic until you model provider payroll, rent, equipment debt, admin, and reserves. The right way is: owner pay + reserves + fixed costs + provider payroll, then divide by the clinic’s contribution margin (cash left after variable costs); in year 1, the model says collections are $392M, but payer mix and procedure volume still change the cash math. So the answer is not a universal threshold.
Set pay from cash math
Start with owner pay target
Add reserves and fixed costs
Add provider payroll next
Divide by contribution margin
What changes the answer
Payer mix changes cash
Procedure volume changes cash
Rent and debt matter
Admin and reserves matter too
Is owning an ophthalmology clinic worth it?
Owning an Ophthalmology Clinic can be worth it only if owner cash flow beats employed ophthalmologist income after payroll, rent, debt service, reserves, and taxes; for the core success gauge, see What Is The Most Important Metric To Measure The Success Of Your Ophthalmology Clinic?. The upside is scale: supplied collections move from $392M in year 1 to $2,926M at maturity, but the owner also carries hiring, payer, equipment, compliance, scheduling, and reinvestment risk.
Why it can work
Scale collections from $392M to $2,926M
Improve margin through procedure mix
Add ancillaries tied to patient demand
Build practice equity over time
What reduces return
Compare against employed physician pay
Subtract payroll, rent, and debt service
Fund reserves, taxes, and reinvestment
Count daily management as real work
Key Takeaways
More providers only help if slots fill and convert.
Collections beat charges; net cash is what matters.
Staff and equipment must match real throughput.
Owner pay comes after debt, payroll, and reserves.
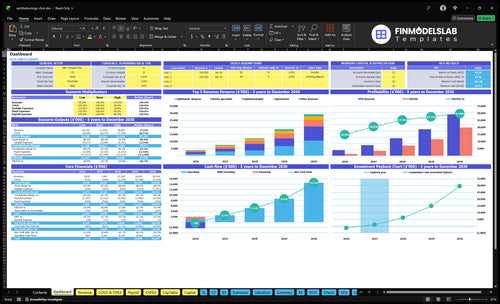
Compare low, base, and mature ophthalmology clinic income scenarios
Owner income scenarios
Income shifts with provider count, capacity, collections, and overhead, so the owner's take-home can swing a lot even when the clinic is profitable.
A quick read on low, base, and high owner income paths.
Scenario
Low CaseLow Case
Base CaseBase Case
High CaseHigh Case
Launch model
This is the slower first-year ramp, with owner income tied to early collections and a smaller provider base.
This is the mid-ramp case, where the clinic is scaling but still carrying meaningful overhead.
This is the stronger upside case, where the clinic is near mature throughput and the owner is benefiting from scale.
Typical setup
The clinic runs with 6 total providers at 65.0% capacity, about $392M in collections, and tight cash after payroll and fixed overhead.
The model reaches 12 total providers at 80.0% capacity, with about $1,232M in collections and a stronger spread of revenue across specialties.
The model reaches 20 total providers at 90.0% capacity, with about $2,926M in collections and the highest contribution before fixed overhead.
Cost drivers
6 total providers
65.0% capacity
$392M collections
payroll
fixed overhead
12 total providers
80.0% capacity
$1,232M collections
staffing scale
fixed overhead
20 total providers
90.0% capacity
$2,926M collections
staffing scale
reserve needs
Owner income rangeBefore owner reserves
Year 1: about $1.3MLow Case
Year 3: about $7.1MBase Case
Year 5: about $19.9MHigh Case
Best fit
Use this to stress-test the opening year and see how much income survives a slow ramp.
Use this as the working case for lender decks, staffing plans, and owner draw planning.
Use this to test upside, expansion timing, and how much cash the owner can pull after reserves.
!
Planning note: Scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions; owner take-home still depends on fixed costs, payroll, financing, and reserves.
Ophthalmology Clinic Core Six Income Drivers
Provider Productivity
Provider Productivity
Provider productivity is the share of provider time that turns into collectable treatment volume. The model is simple: provider count × monthly treatments × price × capacity. Year one assumes 2 ophthalmologists, 1 surgeon, 1 optometrist, 1 retina specialist, and 1 glaucoma specialist; mature year scales to 6, 4, 5, 3, and 2 in the same role order, so staffing drives revenue before fixed costs even show up.
What this hides is the gap between booked visits and paid work. The model’s capacity assumption rises from 650% to 900%, but no-shows, technician support, schedule design, and procedure conversion decide what gets collected. A fuller calendar does not always mean higher owner pay; empty exam lanes or unused procedure slots can leave revenue on the table even when demand is strong.
Track the lanes
Measure collected treatments per provider, not just appointments booked. Keep a simple weekly view of no-show rate, procedure conversion, and exam-lane fill so you can see where provider time leaks out of cash flow.
Track visits per provider, per month
Track no-shows and same-day fills
Track procedure slots used vs open
Track technician hours by provider
Manage exam lanes and procedure slots first. If technician support is thin or the schedule is built around raw appointment count, collections fall before the day ends, and that cuts gross margin, slows cash in, and lowers what the owner can safely take home.
Equipment, Facility, and Financing Costs
Equipment, Facility, and Financing Costs
Fixed cash commitments can cap owner income fast in an ophthalmology clinic. Optical coherence tomography (OCT), visual field machines, exam lanes, lasers, EMR, buildout, rent, leases, and debt service all come before owner distributions, so a paper profit can still leave weak cash. Capital expenditures are purchases, while depreciation is only an accounting expense.
The key inputs are monthly collected revenue, lease and loan payments, rent, and replacement reserves. One line says it clearly: cash out before owner pay. If collections slow or equipment sits underused, break-even rises and the owner’s draw gets pushed back.
Match each payment to volume
Build the schedule around expected exams, procedures, and collections, not around what the vendor approves. Track monthly utilization for each lane and machine, then compare it with the related lease or debt payment. If an OCT or laser is paid from current cash, it should support enough billable volume to cover that fixed cost.
Track monthly collections vs. debt service.
Separate capex from depreciation.
Hold reserves for replacement.
Test payment timing against volume ramp.
Use reserve rules for future replacement, working capital, and delayed insurance cash. When the clinic adds a fixed cost before the schedule fills, margin may still look fine on paper, but actual cash for owner pay shrinks. The clean check is simple: does this payment earn its keep this month?
Payer Mix and Collections
Paid Collections
This driver is about cash collected, not billed charges. Average collection assumptions here range from $150 per optometry visit to $3,500 in first-year surgery and $4,100 in mature-year surgery. Payer mix, deductibles, denials, prior authorization, billing accuracy, and collection timing all move the cash that supports owner pay.
What this hides is local contract detail. If claims sit unpaid, days in accounts receivable rises and cash gets tighter even when volume looks strong. One clean line: collections drive pay, not posted charges.
Track the Cash, Not the Charge
Track net collection rate, denial rate, days in accounts receivable, and patient balance follow-up by payer and service line. Use local data before quoting reimbursement, and fix prior auth and coding before the claim leaves the door. Faster clean claims mean better cash flow and a safer owner draw.
Net collection rate by payer
Denial rate by service line
Days in A/R each week
Patient balance follow-up speed
Slow collections can squeeze payroll, debt service, and distributions at the same time.
Staffing Efficiency
Staffing Efficiency
Staffing efficiency is the fit between labor and patient flow. Technicians, scribes, front desk, billing, call handling, and training support need to match provider volume; if they don’t, rooming slows, authorizations slip, and collections lag. That lowers owner take-home because payroll goes out before cash comes in.
Overstaffing hurts too. Extra hours in low-volume months raise payroll with no extra collections. The key check is visits per tech hour, claims per billing employee, schedule fill rate, and turnover cost. Right-sized labor protects margin; the wrong ratio turns growth into wage drag.
Right-Size Labor to Volume
Build staffing by provider type, then map each role to one output measure. Use techs for rooming and prep, scribes for documentation, billing for clean claims, and front desk for fills and recalls. If a hire does not speed rooms, clean claims, or keep the schedule full, it is cutting into profit and owner draw.
Track rooming time by provider.
Watch claim lag and denials.
Review fill rate every week.
Price turnover into hiring plans.
If onboarding takes too long or no-shows rise, labor stays fixed while collections fall, so trim hours before cutting service quality.
Procedure, Diagnostic, and Ancillary Mix
Procedure, Diagnostic, and Ancillary Mix
This driver is the split of procedures, diagnostics, visits, and ancillary sales each patient generates. It affects owner income because higher-acuity cases usually collect more per patient and can improve gross margin, while visit-heavy mix can cap cash even when volume looks healthy.
In the model, first-year surgery contributes $109M and retina $140M, while glaucoma is $351k, ophthalmology visits are $780k, and optometry is $293k. Mature-year surgery reaches $1,063M and retina $998M, so the real swing is case mix, not just patient count.
Track mix, not just volume
Measure procedure mix, diagnostic capacity, referral flow, and ancillary gross margin by service line. Here’s the quick math: if more patients convert to surgery, retina work, or compliant co-managed care, collections per patient rise and fixed overhead is easier to cover.
Track collections per patient.
Watch diagnostic slot fill rate.
Measure referral conversion monthly.
Separate optical and contact margin.
What this estimate hides is payer mix and claim timing. If diagnostics bottleneck or referrals slow, the clinic loses higher-value cases and owner pay drops even when exam volume stays steady.
Owner Role, Draws, and Reserves
Owner Draws and Reserves
Owner pay is the cash left after payroll, debt service, and reserve rules. In this model, contribution rises from $317M in year one to $2,472M in the mature year before fixed costs, so the owner’s draw depends on how much cash survives staffing, rent, and claim timing.
Clinical owners may take wages plus distributions; managing owners often rely on residual profit; multi-provider owners may keep more cash for growth. Reserves should cover equipment replacement, working capital, claim delays, and hiring. If cash is thin, reported profit can look fine while take-home pay stays low.
Set Pay After Cash Rules
Set a fixed rule for owner pay after payroll, debt service, and reserve funding. Track collected cash, not just booked revenue, and review claim lag before increasing draws. That keeps owner income tied to real cash, which matters more in a clinic with surgery, diagnostics, and longer billing cycles.
Track cash after claims.
Fund equipment replacement first.
Hold cash for hiring.
Separate wages from distributions.
One clean rule helps: if reserves drop below plan, pause the draw increase. That protects the clinic’s ability to replace equipment and absorb slow collections without cutting patient access or leaning on debt.