This guide separates ophthalmology clinic CAPEX from total launch funding, because equipment and build-out are only part of the startup budget In the first operating year model, fixed overhead and payroll total $138,458 per month, before working capital for reimbursement delays and before any CAPEX inputs not provided in the data ASC build-out, hospital-based surgery center costs, real estate purchase, debt service, owner draws, and taxes sit outside the base clinic scope
Estimate Startup Costs with Calculator
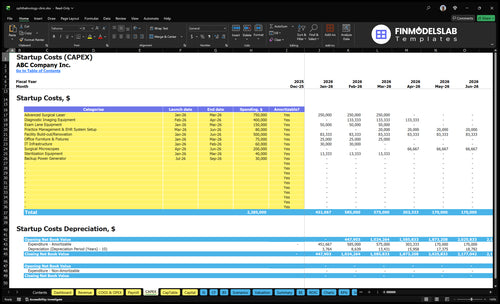
Startup CAPEX Calculator
Estimates startup capital expenditures for capitalized assets only, using user-entered quotes for equipment and build-out.
!
CAPEX limits This tool estimates startup CAPEX only. It excludes payroll runway, working capital, inventory, deposits, debt service, marketing, and ongoing operating expenses. The source data gives operating cost assumptions, not CAPEX unit prices, so use vendor quotes for final inputs.
Calculate Fuding Needs
Startup cost summary
This table summarizes the main startup CAPEX and the excluded working capital reserve for an ophthalmology clinic.
Highlighted CAPEX$1,880,000Base planning example
Excluded cash needs$832,000Outside CAPEX total
Funding need$2,712,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Facility Build-out / Renovation
$500,000
Leasehold improvements and clinical space build-out
Yes
Advanced Surgical Laser
$750,000
Surgical equipment cost and installation
Yes
Diagnostic Imaging Equipment
$400,000
Imaging system spec and calibration
Yes
Exam Lane Equipment
$150,000
Exam room count and ophthalmic instruments
Yes
Practice Management & EHR System Setup
$80,000
Software setup, IT integration, and licensing
Yes
Working Capital Reserve
$832,000
Month 1-6 cash gap from payroll, rent, insurance, and variable costs
Startup cost jumps fast when you add lanes, imaging, and staffed specialists. Lean trims the build; Base matches the Year 1 model; Full adds more procedure depth and cash needs.
Lean, Base, and Full launch cost bands
Scenario
Lean LaunchSmaller build
Base LaunchYear 1 match
Full LaunchBigger build
Launch model
Starts with fewer lanes, basic diagnostics, and a smaller care team for core eye exams and simple visits.
Runs the Year 1 model at 65% capacity with 2 ophthalmologists, 1 ophthalmic surgeon, 1 optometrist, 1 retina specialist, and 1 glaucoma specialist, plus about $326,625 monthly revenue.
Adds deeper imaging, more procedure capacity, more lanes, and more working capital, but stays short of an ambulatory surgery center.
Typical setup
Uses a tighter clinic footprint, lighter imaging, and lower equipment spend.
Single-clinic buildout with standard exam lanes, imaging, surgical tools, EHR setup, and the listed specialty mix.
Uses a larger clinic footprint with more equipment, more staff, and higher inventory and cash support.
Cost drivers
Fewer exam lanes
basic diagnostics
smaller staff
lighter IT setup
lower equipment needs
Core specialist staffing
advanced surgical laser
diagnostic imaging
facility build-out
working capital
More lanes
deeper imaging
more procedure capability
larger staff
higher working capital
Planning rangeCAPEX only
$1,000,000 - $1,600,000Lowest funding
$2,250,000 - $3,250,000Core funding
$3,250,000 - $4,750,000High funding
Best fit
Best for founders who want a narrower service mix and a lower first raise.
Best for operators who want the modeled launch plan and a balanced service mix from day one.
Best for groups planning a broader specialty mix and enough cash to support a heavier launch.
!
Planning note: These ranges are researched planning assumptions, not exact vendor quotes or bids.
How much money do I need to open an ophthalmology clinic?
You need total launch capital equal to CAPEX plus startup costs plus working capital, not equipment alone; the model shows a $432,421 monthly operating gap before CAPEX. For context, What Is The Most Important Metric To Measure The Success Of Your Ophthalmology Clinic? matters because capacity and payer cash timing drive whether this Ophthalmology Clinic can absorb that gap.
Model math
$326,625 planned monthly revenue
$620,588 monthly variable costs
$96,458 monthly payroll
$42,000 monthly fixed costs
Funding bucket
Add clinic buildout and equipment CAPEX
Fund deposits and pre-opening payroll
Cover credentialing lag and insurance
Stock initial supplies and injectables
What hidden costs come with opening an ophthalmology clinic?
The biggest hidden costs in an Ophthalmology Clinic are timing risk and reimbursement lag, not just the lease and equipment. If you’re sizing the downside, see How Much Does The Owner Of An Ophthalmology Clinic Typically Make? because cash can get tight before claims pay. In the model, malpractice insurance starts at $8,000/month, and Year 1 payroll starts at $96,458/month, so hiring too early can burn cash fast.
Upfront setup
Credentialing delays first payments
Payer enrollment can take weeks
Compliance setup adds real labor
EHR and billing setup cost time
Monthly cash drain
General liability: $1,000/month
IT and cybersecurity: $1,800/month
Practice software: $1,500/month
Staff training and disposables need cash
What equipment do you need to start an ophthalmology clinic?
For an Ophthalmology Clinic, start with the core exam-room set and scale the rest to your service mix. At minimum, you need exam chairs, slit lamps, phoropters, lensometers, autorefractors, and tonometers; with 2 ophthalmologists, 1 ophthalmic surgeon, 1 optometrist, 1 retina specialist, and 1 glaucoma specialist, diagnostic depth matters. Retina and glaucoma care can add optical coherence tomography (OCT), fundus imaging, visual field testing, and procedure equipment, and the budget should follow exam lane count, imaging volume, and whether you buy, finance, or lease, since CAPEX unit costs are not provided.
Core exam setup
Exam chairs for each lane
Slit lamps for eye exams
Phoropters for refraction work
Tonometers for pressure checks
Specialty imaging add-ons
OCT for retina and glaucoma
Fundus imaging for retinal views
Visual field testing for glaucoma
Procedure tools for surgical work
Key Takeaways
Equipment spend should match lanes and launch scope.
Build-out costs are separate from monthly lease payments.
Software, interfaces, and support need distinct line items.
Payroll and working capital drive the biggest cash need.
Ophthalmology Clinic Core Five Startup Costs
Ophthalmic Diagnostic And Exam Equipment Startup Expense
Largest spend
This is usually the largest clinic-specific CAPEX, meaning upfront equipment spend. Build the schedule by exam lane and clinical scope, then tag each item as buy, lease, or finance. Include exam chairs, slit lamps, phoropters, lensometers, autorefractors, tonometers, optical coherence tomography, fundus imaging, visual field testing, and any procedure gear needed on day one.
Lane-based list
Tie each line to lane count, room count, and the services starting in Year 1: ophthalmology, surgery, optometry, retina, and glaucoma. That mix means some devices are not optional if those services launch on day one. Keep the schedule user-entered so you can add quantities, acquisition method, and timing without hard-coded prices.
Spend control
Cut waste by matching equipment to actual volume, not wish lists. Start with the core exam set, then add advanced imaging and procedure tools only where the service line needs them. The mistake to avoid is buying duplicate devices for thin lanes; the better move is to stage purchases by opening date and use financing only where cash flow can support it.
Day-one rule
One clean rule: if a service starts on day one, its device should be in the opening budget. If it waits, the equipment can wait too. That keeps the capital plan aligned with clinical scope and stops underbuilding retina or glaucoma capacity while also avoiding unused spend in lower-volume lanes.
Licensing, Credentialing, Insurance, And Compliance Startup Expense
Launch gates
You cannot open and bill patients until the basics are done: state medical board rules, entity formation, National Provider Identifier enrollment, payer enrollment, CLIA review if in-house testing is planned, OSHA setup, and HIPAA compliance. The model carries $8,000 a month for malpractice, $1,000 for general liability, and $1,000 for professional fees, before any state filing costs.
Budget lines
Estimate this cost by counting required filings, months of coverage, and outside help. Here’s the quick math: recurring insurance and professional fees equal $10,000 per month, so every extra month before launch adds that much cash need. State fees and payer timelines are local variables, so verify them with your own advisors.
Count state filings
Price insurance months
Quote legal and consulting help
Control spend
Keep this lean by getting one local quote set for malpractice, liability, and professional help, then reuse the same credentialing packet for the board, NPI, and each payer. Don’t skip HIPAA or OSHA work; fixing gaps after launch usually costs more than doing it once. Verify state rules locally.
Approval file
Your pre-opening file should show the approvals, policies, and certificates that prove you are ready to see patients. That means the medical board path, NPI, payer IDs, insurance binders, CLIA status if needed, and written HIPAA and OSHA controls.
Ophthalmology EHR And Practice Management Startup Expense
Core software stack
A clinic EHR budget should split one-time setup from monthly fees. The source model carries $1,500 per month for practice management software and $1,800 per month for IT support and cybersecurity, or $3,300 per month total before any interface hosting. Add separate lines for implementation, hardware setup, and device interfaces.
Setup cost lines
This cost covers scheduling, billing, claims setup, patient portal setup, image management, cybersecurity setup, hardware, networking, and diagnostic-device interfaces. Price it with vendor quotes for implementation, hardware setup, and any interface build. Keep each line separate so startup cash needs stay clear and you do not bury a one-time build inside monthly software spend.
Quote implementation as one-time.
Quote hardware separately.
Price each device interface.
Lower the burn
Cut this expense by phasing noncritical interfaces, but do not delay the links that move imaging and diagnostic results into the clinical record. Ask for bundled onboarding, then compare the monthly run rate after go-live. A clean target is to keep recurring software and IT fees at the quoted $3,300 per month unless added modules clearly drive revenue or compliance.
Phase low-use modules later.
Bundle onboarding where possible.
Test result flow before launch.
Interface risk
If imaging and diagnostic data do not flow into the chart, staff will re-enter results by hand, which slows visits and raises error risk. Budget the interface build as its own startup line, then verify every device feed before day one. That is the part that protects both workflow and documentation quality.
Ophthalmology Office Build-Out Startup Expense
Leased Fit-Out
For a leased ophthalmology clinic, this line covers the tenant build-out, not buying the building or building an ambulatory surgery center. It includes reception, waiting room, exam lanes, testing rooms, storage, staff space, ADA access, lighting, electrical, plumbing, medical-grade finishes, signage, and patient flow. Use it to size the space before equipment spend.
What It Covers
Start with $25,000 monthly rent from Month 1 and keep deposits separate from capital improvements. Build-out should be estimated from square footage, landlord allowance, number of exam lanes, imaging rooms, and any procedure space. A bigger clinical scope means higher fit-out needs, even before the first patient is seen.
Price by square foot.
Separate rent from improvements.
Design for day-one lanes only.
How To Control
Keep the layout tight to day-one volume and ask for tenant improvement dollars in the lease. Don’t overbuild optical space or procedure rooms you won’t use yet. Common mistake: mixing rent, security deposits, and build-out in one line. Separate quotes make landlord offers easier to compare.
Cash Timing
The cash hit is front-loaded: you may start paying $25,000 a month in rent while construction is still underway, so fund both occupancy costs and fit-out at once. If landlord allowance is weak, the clinic needs more working capital to bridge the gap until opening.
Staffing, Supplies, And Launch Working Capital Startup Expense
Launch payroll
Pre-opening payroll is a launch cash item, not normal operating payroll. For this clinic, the Year 1 payroll run rate is $96,458 per month, and the staffing list implies about $1.19M a year in salaries. Fund training and ramp-up before collections start, because early patient volume rarely matches full staffing on day one.
Year 1 team
The Year 1 team combines clinical and front-office coverage: 1 lead ophthalmologist or medical director, 1 surgeon, 1 optometrist, 2 technicians, 1 practice manager, 2 front desk coordinators, 1 billing specialist, and 1 marketing coordinator.
Clinical care drives capacity
Front desk protects flow
Billing protects cash
Working cash
Launch working capital covers training, supplies, drugs, disposables, signage, local launch marketing, and the collection-delay reserve. A collection-delay reserve is cash held for the gap between treating patients and getting paid. The model assumes variable costs equal 190% of revenue, so this cushion matters.
Pay for launch before collections
Keep supplies separate from payroll
Build a payer delay buffer
Cash bridge
With variable costs at 190% of revenue, early sales can still leave a cash gap. Keep launch cash separate from capex, and size the reserve for slower collections, not best-case billing. That keeps payroll, consumables, and patient flow funded while the clinic ramps.