How Much Does a Pain Management Clinic Owner Make at $146K/Month?
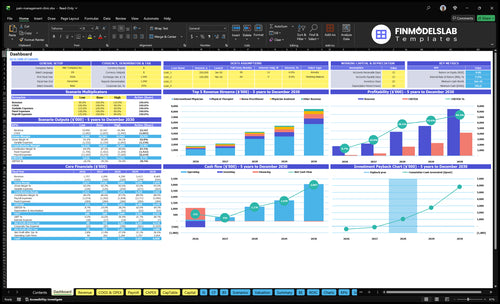
You’re estimating owner take-home from a US pain management clinic, so start with collections, not billed charges The provided first-year model shows $146,445 in monthly revenue and about $49,743 in monthly operating profit before owner pay, reserves, debt, and taxes This excludes personal taxes, debt structure, state ownership rules, and individual reimbursement contracts
Owner income$49.7k/moNet margin34%Revenue for target pay$103.1k/moBusiness difficultyHard
Want to test your owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay for a pain management clinic.
!
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want the six biggest income drivers?
1
Procedure Mix
$1.5K
More interventional visits lift revenue per slot, so the owner keeps more profit than a therapy-heavy mix.
2
Payer Mix
6.0%-5.0%
Cleaner collections and lower billing drag keep more billed revenue as cash for owner pay.
3
Provider Capacity
65%-85%
Moving utilization from 65% in Year 1 to 85% in Year 5 spreads fixed cost over more visits and raises take-home.
4
Staffing Model
$930K
First-year payroll is about $930K, so adding full-time staff too early can wipe out EBITDA.
5
Fixed Overhead
$23.7K/mo
The clinic carries $23.7K a month in fixed overhead, and every empty slot hurts owner cash.
6
Referral Flow
2 mo
Fast referrals and authorization keep schedules full, which is what gets the clinic to breakeven by Month 2.
Want to check owner pay in the Pain Management Clinic model?
What costs most affect pain management clinic profit margin?
For a Pain Management Clinic, the biggest margin hits are provider payroll, clinical staff, lease, billing, supplies, pharmaceuticals, EHR software (electronic health records), insurance, and denials; first-year known payroll is $52,500/month and fixed overhead is $23,700/month, so fixed burn starts at $76,200/month before variable costs. For startup cost context, see How Much Does It Cost To Open A Pain Management Clinic? The cash-risk part is just as important: denials and authorization delays slow collections, not just margin.
Fixed costs
$52,500/month payroll is known.
$23,700/month overhead is fixed.
Lease and insurance hit early.
Billing and EHR keep running.
Cash leaks
Variable costs are 140% of revenue.
At $146,445/month, each 1% cost rise cuts profit by about $1,464/month.
A 10% revenue drop cuts contribution by about $12,595/month.
Denials and delays slow cash timing.
How much revenue is needed to pay a pain management clinic owner?
A Pain Management Clinic needs about $88,605/month to break even before owner pay. To add a $150,000 annual owner paycheck, plan for about $103,140/month in revenue. That math uses $23,700 monthly overhead, $52,500 payroll, and 140% variable costs.
Break-even load
$23,700 fixed overhead
$52,500 monthly payroll
140% variable costs
$88,605 break-even revenue
Owner pay target
$150,000 annual owner paycheck
$103,140 monthly revenue target
Separate salary from distributions
Keep reserves and retained cash apart
How does the owner’s role change pain clinic income?
An owner’s income changes fast in a Pain Management Clinic because clinical pay and ownership profit are not the same thing. If the owner fills the $300,000 interventional physician role or the $150,000 clinic director role, that pay should be tracked separately from distributions. Here’s the quick math: going from 1 to 3 interventional physicians lifts modeled monthly revenue from $146,445 to $705,713 by year 5; state ownership and supervision rules vary, so this is not legal advice.
Pay is role-based
$300,000 physician role pay
$150,000 clinic director pay
Separate salary from profit
Track each role cleanly
Scale drives profit
1 to 3 physicians
$146,445 to $705,713
50 million+ adults have chronic pain
Rules vary by state
Key Takeaways
Procedure mix drives the biggest revenue swing.
Collections depend on payer mix and clean claims.
Utilization and scheduling decide monthly revenue capacity.
Fixed overhead and staffing set the owner pay floor.
Compare low, base, and high owner take-home scenarios
Owner income scenarios
Owner income changes fast as volume, staffing, and fixed overhead scale. These cases test the gap between first-year ramp, mid-scale operations, and mature-year throughput.
Compare low, base, and high owner income cases for the clinic.
Scenario
Low CaseDownside case
Base CaseModeled case
High CaseUpside case
Launch model
This is the lower-earnings path built from first-year assumptions and lighter scale.
This is the modeled middle case built on year 3 scale.
This is the stronger earnings path built on year 5 scale and fuller capacity.
Typical setup
It uses $146,445 in monthly revenue, 140% variable costs, $23,700 fixed overhead, $52,500 known payroll, and $49,743 in monthly operating profit before reserves.
It uses $360,675 in monthly revenue, 128% variable costs, $90,833 known payroll, and $199,909 in monthly operating profit before reserves.
It uses $705,713 in monthly revenue, 120% variable costs, $132,500 known payroll, and $464,827 in monthly operating profit before reserves.
Cost drivers
First-year volume
high variable-cost load
fixed overhead
known payroll
missing reserve input
Year 3 volume
broader staffing
lower cost ratio
known payroll
missing reserve input
Year 5 volume
larger staff base
better capacity use
known payroll
missing reserve input
Owner income rangeBefore owner reserves
$49,743/moThin cushion
$199,909/moBase income
$464,827/moHigh income
Best fit
Use this to stress-test early ramp, tight cash, and weak utilization.
Use this as the planning case for steady growth and normal clinic throughput.
Use this to test upside if the clinic scales faster and keeps throughput high.
!
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. Missing payroll, debt, tax, and reserve inputs can move take-home materially.
Pain Management Clinic Core Six Income Drivers
Procedure Mix
Procedure Mix
Procedure mix is the biggest income lever because the model prices interventional physician treatments at $1,500 in year 1, versus $120 for physical therapy, $180 for a nurse practitioner, $180 for a physician assistant, and $170 for clinical psychology. Shift more visits into higher-priced procedures, and monthly collections rise faster than headcount alone.
Here’s the quick math: the model says 100 interventional treatments at 650% utilization produce $97,500/month before costs. What this hides is the extra load on supplies, procedure rooms, documentation, and prior authorization flow, so the mix can lift profit only if those operating steps stay tight.
Track the mix
Track procedure mix by slot type, collections per slot, and denied claims. One clean metric is revenue per utilized treatment slot, because it shows whether the schedule is shifting toward the services that fund owner pay.
Measure interventional share weekly.
Watch authorization lag days.
Track supply cost per procedure.
Separate room time by provider type.
If interventional volume rises before authorizations, staffing, and rooms are ready, cash can get tighter even while billed revenue looks strong. Keep the mix aligned with the steps that collect money, not just the steps that fill the calendar.
Fixed Overhead And Equipment
Fixed Overhead Floor
$23,700/month in fixed overhead sets the revenue floor before owner pay starts to look attractive. The named items total $20,700 from the $15,000 lease, $2,500 utilities, $2,000 fixed marketing, and $1,200 insurance, so the rest sits in other fixed costs. That is $284,400/year before distributions.
Here’s the quick math: this cost stays on even if rooms are empty, so idle procedure rooms and unused provider time hit profit fast. Add equipment, malpractice, software, supplies, or debt service, and the owner’s take-home falls dollar for dollar unless volume and collections rise with it.
Match fixed cost to booked capacity
Track fixed cost per month and per filled treatment slot. Use the rule: don’t add a new lease, system, or payment until booked volume can support it.
Reforecast after every hire.
Watch room utilization weekly.
Delay costs until demand is steady.
If utilization slips, owner pay should tighten before fixed overhead grows.
Staffing Model
Staffing Load
Staffing is the gatekeeper between collections and owner take-home. First-year payroll is $52,500/month across the clinic director, office manager, receptionist, interventional physician, and physical therapist. Against modeled revenue of $146,445/month, payroll uses about 35.8% before billing fees, rent, supplies, and taxes, so a weak schedule can wipe out cash fast.
The pay map matters. The interventional physician is budgeted at $300,000/year, or about $25,000/month, and the physical therapist at $80,000/year, or about $6,667/month. That leaves about $20,833/month for the clinic director, office manager, and receptionist. Any missing salary line for other provider types must be added before final owner income is set.
Model Every Salary Line
Track payroll by role, not as one blended number. Separate owner labor pay from investor distributions, then test whether monthly collections can cover payroll and fixed costs. If staffing is built for volume that does not show up, owner draw should wait until cash flow proves the clinic can support it.
Use a simple coverage check: payroll divided by monthly collected revenue. If that ratio climbs while rooms sit open, trim hours, delay hires, or move to part-time coverage until utilization improves. Add every missing compensation line before forecasting take-home, or the model will overstate distributable profit.
Payer Mix And Collections
Payer Mix & Collections
Payer mix and collections decide how much billed revenue turns into cash. The model uses service prices as planning inputs, including $1,500 for interventional physician treatments in year 1, but owner income depends on collected revenue, not charges. Commercial, Medicare, Medicaid, workers’ compensation, self-pay, denials, and authorization rules all change cash timing.
Billing service fees take 40% of revenue in year 1 and 35% later, so weak collections hit margin twice: slower cash and less net revenue. If claims are denied or paid late, staff and overhead still run first, which delays owner draw. Payer concentration risk should lower confidence in the forecast.
Track Cash by Payer
Track collections by payer, not just visits. Watch net collection rate, denial rate, days in accounts receivable, and the share of cash from the top payer. If one payer drives most receipts, a rule change can move monthly owner pay fast. Build the forecast from expected cash receipts, then test slower payment timing and denied claims.
Use $1,500 as a planning price, then compare billed, allowed, and collected dollars each month. Tight coding, prior authorization checks, and clean claim submission protect margin better than volume alone. As billing fees fall from 40% to 35%, owner take-home improves only if collections hold and bad debt stays low.
Provider Capacity
Provider Capacity
This driver is the number of billable treatment slots your team can actually fill. In the model, utilization—booked capacity used—rises from 650% in year 1 to 850% in year 5, and monthly revenue climbs from $146,445 to $705,713. More filled slots lift revenue before overhead, so owner pay improves only when capacity turns into paid visits.
No-shows, unused procedure slots, authorization delays, and provider downtime cut contribution fast. $23,700/month of fixed overhead keeps running even when rooms sit empty, so weak scheduling turns into lower profit and less cash available for the owner draw.
Track Filled Slots Weekly
Measure booked slots, completed visits, no-show rate, and days lost to authorization or downtime. Those are the inputs that show whether capacity is converting into collected revenue. If one provider or room is the bottleneck, the revenue gap hits margin first, then cash flow, then owner pay.
Protect the schedule with reminders, waitlists, tighter authorization timing, and same-week fill rules for open slots. The goal is simple: keep rooms used often enough that fixed overhead is spread across more billed visits, not fewer.
Referral And Authorization Flow
Referral and Authorization Flow
Referrals and prior authorizations decide whether booked demand turns into collected cash. If approvals lag, procedure slots stay empty, utilization drops, and collections slide into later months. With $23,700/month of fixed overhead still running, slow approvals raise the cash break-even point even when patient volume looks strong. One key metric is days in accounts receivable; when it rises, owner pay usually gets squeezed first.
Claim denials hurt twice: they delay cash and can erase revenue tied to staffed rooms and provider time. This driver includes documentation, coding, claim submission, and denial management. If billing is sloppy, take-home income falls because collected revenue, not billed charges, pays rent, payroll, and owner draws.
Tighten the approval-to-cash path
Track referral-to-authorization time, authorization approval rate, denial rate, and days in accounts receivable each week. Here’s the quick math: fewer denials and faster approvals mean more procedure slots turn into cash in the same month, which protects gross margin and keeps owner distributions from slipping behind payroll and rent.
Use a pre-bill check for eligibility, medical necessity notes, codes, and submission timing. If one payer or referral source slows down, cap exposure fast; concentration risk can make monthly distributions look better than they are. Clean claims and fast follow-up matter more than raw patient count when overhead is $23,700/month.