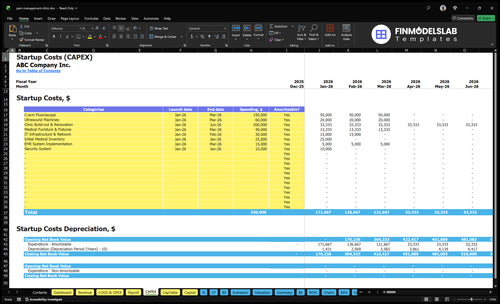
Pain Management Clinic Startup Costs: $520K+ Known CAPEX
A researched pain clinic startup cost estimate should separate upfront startup costs from total funding need In this plan, complete listed CAPEX, meaning capital expenditures for long-lived startup assets, is at least $520,000, led by a $200,000 clinic build-out, $150,000 C-arm fluoroscope, and $60,000 ultrasound machines Total funding need is higher because Month 1 overhead includes $77,500 in payroll and $23,700 in fixed costs, or $101,200 before supplies, billing fees, and collections lag Year 1 assumes 1 interventional physician, 1 physical therapist, 1 nurse practitioner, 1 physician assistant, and 1 clinical psychologist operating at 65% capacity
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for a pain management clinic launch.
!
CAPEX limits CAPEX only. Excludes payroll runway, debt service, working capital, deposits, marketing runway, and inventory runway. Use it to size startup assets, not total funding need.
Calculate Fuding Needs
Startup Cost Summary
Startup cost summary for a pain management clinic, showing key CAPEX items and excluded opening cash needs across low, base, and high cases.
Highlighted CAPEX$495,000Base planning example
Excluded cash needs$505,000Outside CAPEX total
Funding need$1,000,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Clinic Build-out & Renovation
$200,000
Leasehold improvements and clinical room build-out
Yes
C-arm Fluoroscope
$150,000
Procedure equipment spec and installation
Yes
Ultrasound Machines
$60,000
Imaging equipment count and model mix
Yes
IT Infrastructure & EHR Setup
$45,000
Network build, hardware, and system implementation
Yes
Medical Furniture & Fixtures
$40,000
Exam rooms, waiting area, and procedure-room fitout
Higher equipment and staffing intensity pushes launch cost up fast. Lean, base, and full scenarios separate a consult-first office, a standard outpatient clinic, and a more interventional build.
Lean, base, and full launch cost comparison
Scenario
Lean LaunchLower build
Base LaunchCore build
Full LaunchCapital heavy
Launch model
A smaller consult-first clinic with lighter equipment and a simpler service mix.
A standard outpatient pain clinic with core imaging and a full clinical support setup.
A larger interventional setup with the full equipment list plus startup runway for staffing and overhead.
Typical setup
A small office with core treatment rooms, basic IT, and no high-cost imaging line.
A mid-size clinic with treatment rooms, the listed imaging gear, and normal admin support.
A larger clinic with imaging, more providers, and six months of payroll and fixed-cost runway.
Cost drivers
Build-out
IT network
furniture
initial inventory
EHR setup
C-arm fluoroscope
ultrasound machines
build-out
IT network
EHR setup
Base CAPEX
six-month payroll
fixed costs
more providers
larger space
Planning rangeCAPEX only
$320,000+Lower CAPEX
$530,000+Core CAPEX
$1.14M+Highest build
Best fit
Best for smaller square footage, lighter equipment, and a consult-led staffing model with limited reserves.
Best for mid-size space, standard imaging, and a balanced provider mix with moderate reserves.
Best for larger square footage, high equipment intensity, and a multi-provider model with deep reserves.
!
Planning note: These scenario ranges are researched planning assumptions, not vendor quotes or guaranteed bids.
How do interventional pain clinic equipment costs change the startup budget?
A Pain Management Clinic with a consultative office needs far less startup cash than an interventional setup. In the interventional case, imaging alone adds $210,000 from a $150,000 C-arm fluoroscope plus $60,000 ultrasound machines. Add $40,000 medical furniture and fixtures, $30,000 IT infrastructure, and $15,000 EHR implementation, and you are at $295,000 before buildout, shielding, electrical work, and service contracts.
Imaging costs
$150,000 C-arm fluoroscope
$60,000 ultrasound machines
$210,000 imaging total
No imaging line item in consultative office
Other startup items
$40,000 furniture and fixtures
$30,000 IT infrastructure
$15,000 EHR implementation
$295,000 before buildout
How should a pain management clinic financial plan support startup funding?
A Pain Management Clinic funding plan should map startup spend month by month, because lenders care more about timing and runway than one big total. Show the $200,000 build-out across Months 1 to 6, and the $150,000 C-arm, $60,000 ultrasound, $40,000 furniture and fixtures, and $15,000 EHR in Months 1 to 3. Then prove whether $930,000 of Year 1 staffing cost fits the planned volume, payer mix, and collections lag.
Uses of funds
$200,000 build-out in Months 1 to 6
$150,000 C-arm in Months 1 to 3
$60,000 ultrasound in Months 1 to 3
$40,000 furniture and $15,000 EHR
What lenders test
Month-by-month cash use
Provider hiring timing
Payer mix and collections lag
Runway against Year 1 staffing
How much money do I need to open a pain management clinic?
Compliance and insurance start before patient revenue.
Staffing and software costs rise before launch.
Pain Management Clinic Core Five Startup Costs
Facility and Buildout Startup Expense
Buildout
$200,000 covers clinic build-out and renovation from Month 1 through Month 6. It includes leasehold improvements, rent deposits, design, construction, plumbing, electrical, ADA access, waiting area, exam rooms, procedure space, recovery area, signage, and security. This line moves most with location, square footage, procedure capability, and landlord contribution.
Cost Drivers
Estimate this from suite size, room count, trade quotes, and the 6-month build window. Here’s the quick math: one buildout budget, then layer in the lease term and any tenant-improvement credit. If the landlord funds part of the work, upfront cash drops, but the layout still has to support safe patient flow.
Square feet and room count
Trade bids by scope
Landlord contribution terms
Keep It Lean
Keep the plan tight: size the space to the first-year procedure mix, ask for landlord contribution, and phase nonessential finishes after opening if the lease allows. Don’t overbuild recovery or waiting space before demand is proven. The wrong move is paying for unused square footage; that burns cash without improving care.
Match space to procedure volume
Push for tenant-improvement credit
Avoid oversized rooms early
Lease Load
$15,000 per month in facility lease expense runs from Month 1 through Month 60, or $900,000 over five years. This is the fixed cost that hits cash every month, so the lease should match expected visit volume and procedure capacity. The main risk is signing for more space than the clinic can fill.
Medical Equipment and Procedure Asset Startup Expense
Imaging First
The biggest swing is imaging. A launch with interventional capability can add a $150,000 C-arm fluoroscope and $60,000 ultrasound machines. If you stage imaging, the opening budget can stay focused on essentials like procedure tables, exam tables, monitoring, sterilization, emergency supplies, and clinical furniture.
Core Room Assets
Budget the room build as a separate asset list. The base package includes $40,000 in medical furniture and fixtures plus procedure tables, exam tables, monitoring equipment, sterilization equipment, emergency supplies, and clinical furniture. Estimate it from vendor quotes and the number of rooms needed at opening.
Count rooms before buying
Get itemized vendor quotes
Separate must-haves early
Stage Advanced Gear
To reduce upfront spend, launch with essential clinical equipment and add advanced imaging after demand is proven. That keeps cash tied to revenue-producing rooms instead of a full interventional stack on day one. The tradeoff is slower procedure breadth until the $150,000 C-arm and $60,000 ultrasound are in place.
Start with core rooms
Delay imaging buys
Protect cash runway
Track the Budget Split
Track each asset by unit count, quote, and install date. A clean budget separates essentials from optional interventional gear, so you can see whether the opening plan is a room-based clinic or a full imaging launch. That choice drives the first check size and how much cash stays reserved for working capital.
Healthcare Technology, EHR, Billing, and IT Startup Expense
Core System
EHR, medical billing software, practice management, phones, secure messaging, computers, networking, cybersecurity, and clearinghouse links need to be live before the first visit. Here’s the quick math: $15,000 EHR implementation plus $30,000 for IT infrastructure and network, plus $800/month for admin software. Then add EHR subscriptions at 20% of Year 1 revenue and billing fees at 40% of Year 1 revenue.
Cost Drivers
The main inputs are provider count, months of coverage, and how much billing you outsource. If claims, scheduling, and revenue cycle management are not ready on day one, cash collection slows. The fixed build sets the floor, but the revenue-based fees rise with Year 1 sales, so launch timing and billing readiness matter as much as software choice.
Keep It Lean
Keep the first build tight: schedule, billing, secure messaging, and claim flow first; add extras after live use proves demand. Do not cut cybersecurity or clearinghouse setup, because cheap shortcuts can delay payment. The cleanest savings come from staging nonessential features, not from skimping on the core tools that get claims out.
Go-Live Ready
If the clinic opens before the tech stack is ready, staff end up doing manual work and patients wait longer for bills and follow-up. That is why implementation should finish before go-live, not after. One line: no working EHR and billing links, no clean launch.
Licensing, Credentialing, Compliance, and Insurance Startup Expense
Setup and coverage
This cost covers state entity setup, provider licensing, Drug Enforcement Administration (DEA) registration where needed, National Provider Identifier (NPI) setup, payer enrollment, credentialing, Health Insurance Portability and Accountability Act (HIPAA) compliance, malpractice insurance, and general liability. The fixed number here is $1,200 per month for general business insurance; state rules, ownership, provider mix, and service mix drive the rest.
Budget inputs
Build this line from quote-based inputs: number of providers, number of payers, state filings, legal review hours, and months of coverage. Treat $1,200 per month as the recurring insurance base, then add one-time credentialing and licensing fees before opening cash. This is a launch gate, so timing matters as much as price.
Cost control
Reduce spend by sequencing work in order: form the entity, license providers, then enroll payers and finalize malpractice only for the services you launch first. Don’t overbuy coverage for a future service mix. The cleanest benchmark is simple: keep the insurance base at $1,200 per month and tie every added line item to a needed filing or contract.
Watchouts
What this estimate hides is state-by-state fee spread and credentialing delay. If provider mix changes, payer enrollment and malpractice needs can change too, so build a small buffer around the $1,200 per month insurance base and keep legal work scoped to the launch services only.
Staffing Readiness, Supplies, and Launch Preparation Startup Expense
Pre-open payroll
Before the first patient, budget for recruiting and onboarding the clinic director, office manager, receptionist, interventional physician, physical therapist, nurse practitioner, physician assistant, and clinical psychologist. Year 1 payroll is $930,000, or $77,500 per month. This is pre-opening working capital, not equipment spend, and it starts draining cash before revenue lands.
Opening stock
The launch cash need includes $25,000 of initial medical inventory, plus clinical consumables, medication storage supplies if needed, office supplies, uniforms, and launch marketing. The big inputs are opening stock units, refill timing, months of coverage, and your first-month patient volume. Medical supplies run at 50% of Year 1 revenue, and pharmaceuticals at 30%.
$25,000 initial inventory
50% supplies tied to revenue
30% pharmaceuticals tied to revenue
Hold the line
Keep the first order lean and set reorder points from actual visit volume, not wishful demand. The fastest way to waste cash is overbuying supplies and drugs before scheduling stabilizes. $2,000 per month for fixed marketing is manageable, but only if it is tied to booked consults and referral flow.
Order to opening demand only
Track stock-outs weekly
Link marketing to bookings
Budget bucket
Classify recruiting, onboarding, supplies, uniforms, and launch marketing as pre-opening expenses or working capital. Do not treat them as CAPEX unless the model specifically labels them that way. For a clinic, cash tied up in inventory and start-up payroll matters more than depreciation.